
Abstract
Background and Purpose:
To assess the feasibility and efficacy of percutaneous nephrolithotomy (PCNL) in patients with spinal deformities.
Patients and Methods:
Between 1999 and 2008, eight patients (nine renal units) with spinal deformities underwent 10 PCNLs. Mean stone burden was 372 mm2 (160–840 mm2). Preoperative investigation of the respiratory function, evaluation of anatomy by intravenous pyelography or CT spiral scan, and preoperative planning of the percutaneous access by ultrasonography (US) were performed in all patients. Patients were either in a prone (n = 5) or supine (n = 5) position during PCNL. US-guided fluoroscopic adjusted percutaneous puncture of the desired calix was performed in all the patients.
Results:
There was a 40% complication rate related to the number of procedures, with 20% of patients needing blood transfusion and 10% experiencing major complications. Complete stone clearance per kidney after one PCNL was 55.5% (5/9 PCNLs), increasing to 66.6% (6/9 PCNLs) after a second PCNL. Four of nine (44.4%) renal units needed additional procedures after one PCNL (shockwave lithotripsy [SWL], retrograde intrarenal surgery [RIRS], combined simultaneous PCNL and RIRS). At the 3-month follow-up, the overall stone-free rate was 88.8% (eight renal units).
Conclusion:
PCNL in patients with spinal deformities is challenging. Accurate preoperative evaluation of the anatomy and respiratory function and a precise preoperative planning are mandatory. US-guided puncture of the collecting system permits avoiding visceral injury. Supine PCNL offers advantages in terms of patient comfort, protection of cardiorespiratory function, and the ability to perform a simultaneous combined ureteroscopic approach, although the prone position, if feasible with the patient's body habitus, may offer a wider space for percutaneous access. Combination therapy with either SWL or RIRS after PCNL improves stone-free rates.
Introduction
We present our experience with PCNL in patients with marked spinal curvature and provide an assessment of technical difficulties, associated complications, and outcomes to evaluate PCNL as a valid option of urolithiasis treatment in this population.
Patients and Methods
After receiving approval from the Ethics Committee and written informed consent from patients, eight patients who were affected by spinal deformities underwent PCNL for renal stones between 1999 and 2008. The data were collected retrospectively and evaluated (Table 1). Spinal deformity was caused by kyphoscoliosis. Two patients also had severe hip ankylosis (cases 7 and 8). In three patients, the stone location corresponded to the concave side of the spine, where space for percutaneous access was very limited (cases 2, 4, 6) (Table 2).
PCNL = percutaneous nephrolithotomy.
Preoperative diagnostic evaluation of the urinary tract was performed by intravenous urography (IVU) in three patients and by spiral CT in five patients. Evaluation of the respiratory and cardiovascular systems (chest radiography or CT scan, pulmonary function tests, and echocardiography) was carried out in all patients (Figs. 1 –4). Feasibility of percutaneous access was confirmed preoperatively by means of kidney ultrasonography (US) with simulation of the percutaneous puncture. Broad-spectrum antibiotics were administered intravenously as a bolus on induction of anesthesia to ensure adequate prophylaxis.

(
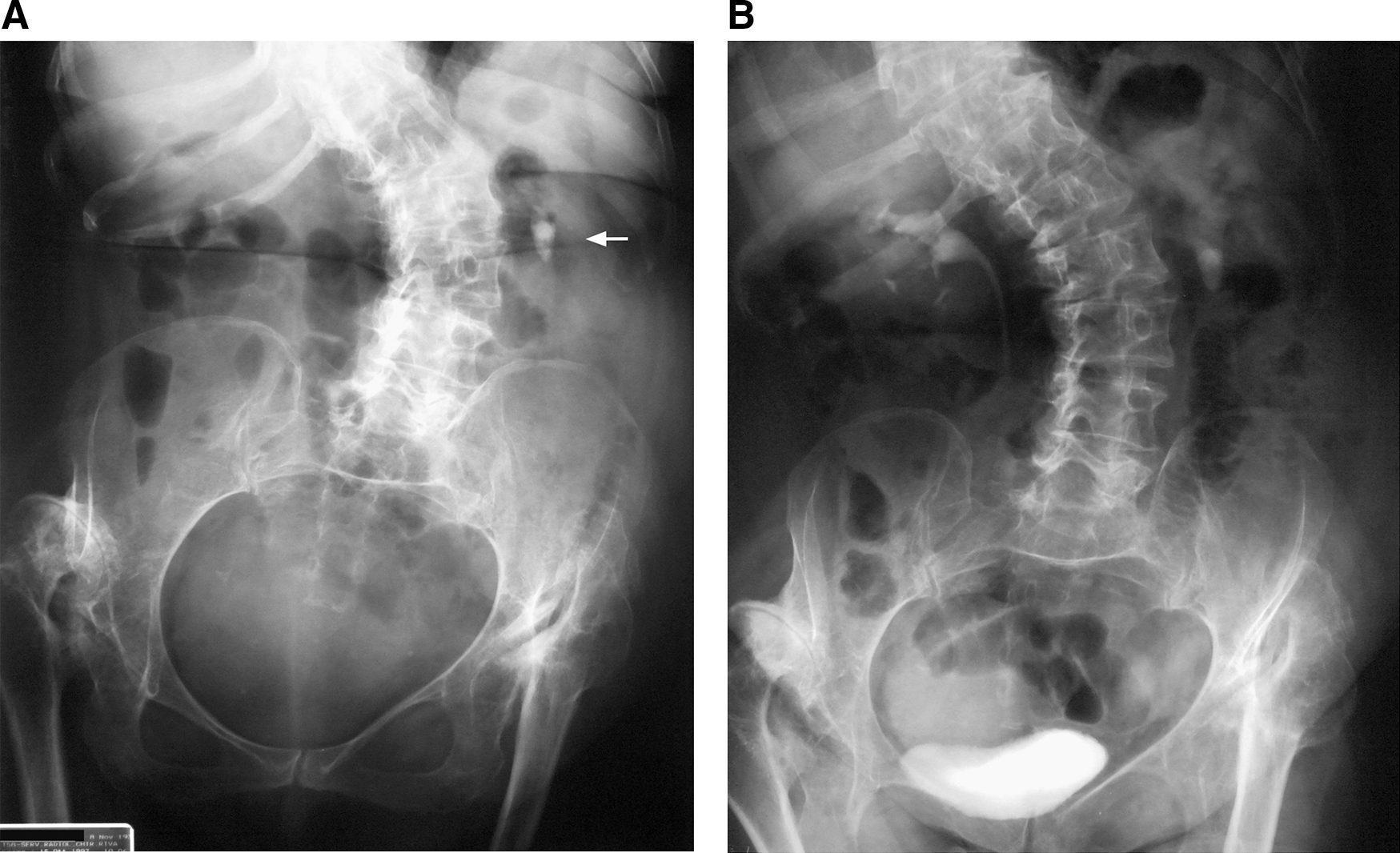
(
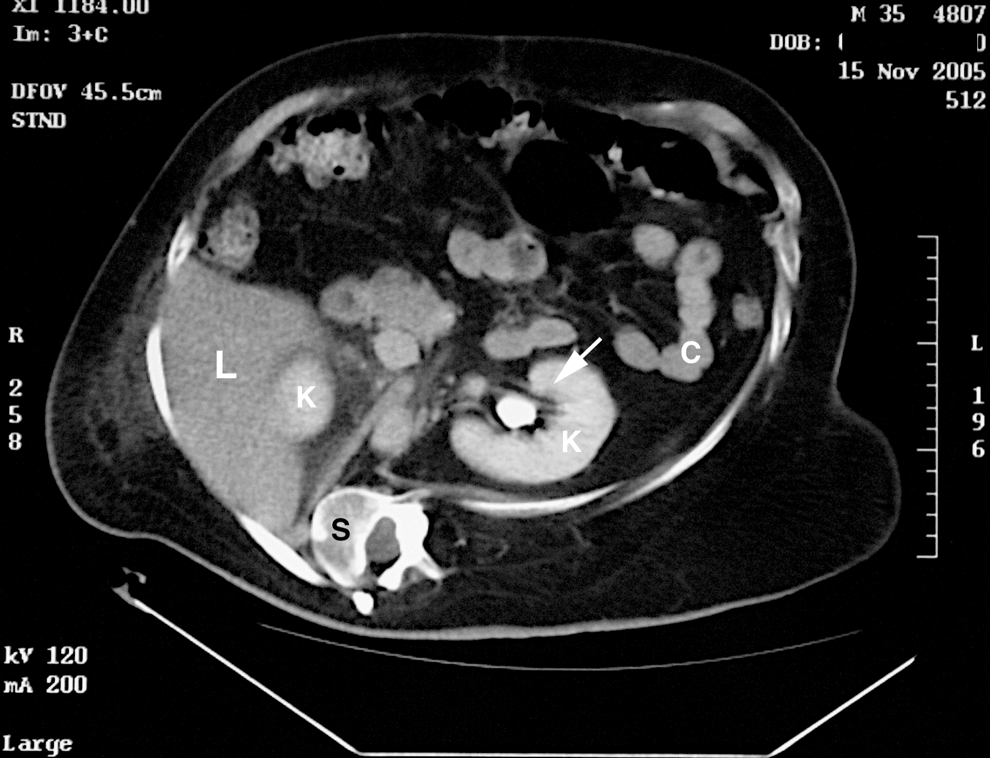
CT scan of a patient with thoracolumbar scoliosis and a calculus (white arrow) on the left renal pelvis. Notice the extreme rotation of the vertebra and the ribs. K = kidneys; L = liver; C = colon; S = spine.

CT scan of the thorax of a patient with kyphoscoliosis. Notice the extreme rotation of the vertebra and the ribs and the asymmetry and narrowing of the lungs. H = heart; L = lungs; S = spine.
The whole procedure, including initial puncture, was performed with the patient under general anesthesia. Each procedure was carried out by an experienced urologist in PCNL (EM). All patients except the two with hip ankylosis were first placed in the lithotomy position, and cystoscopy with a rigid or flexible instrument was performed. Retrograde pyelography was then carried out, and a simple ureteral catheter was advanced to the renal pelvis and left in place.
In the first two cases, PCNL was performed with the patient in the prone position because of lack of experience with the percutaneous approach in the supine or lateral decubitus position. In cases 4 and 6, the prone position was preferred because of a high stone burden or an extremely reduced area for the percutaneous access. In cases 3, 5, 7, and 8, PCNL was carried out with the patient in the supine position. Appropriate structural support with soft padded bolsters and silicone rolls was crucial to obtain the best position for percutaneous access (Fig. 5). A US-guided fluoroscopic adjusted puncture was performed to the most appropriate calix based on preoperative imaging and patient positioning.

Positioning of a patient with scoliosis and hip ankylosis. Notice the pillows under the spine and under the lower extremities.
As soon as the 18-gauge needle reached the renal cavities and drained urine, a 0.097-mm hydrophilic guidewire was passed through the needle into the collecting system. The tract was then dilated by the Amplatz fascial dilator with the one-shot technique under radiologic control, and a 28F or 30F Amplatz sheath (Boston Scientific Corp, Boston, MA) was inserted. A standard 26F nephroscope was placed, and the stone was disintegrated by ballistic and ultrasonic energy combined (Lithoclast Master,® EMS, Nyohn, Switzerland). Flexible nephroscopy was available only for the last five cases and used if stone fragments or additional stone burden was present. Fragments were retrieved by suction or grasping forceps. At the end of the procedure, a 22F reentry nephrostomy in the first three cases or an 8F nephrostomy tube in the last five cases were placed and removed if there was no extravasation or ureteral obstruction seen on a nephrostogram.
Intraoperative and postoperative data and presence of technical difficulties were evaluated. The success rate, combination therapy, and hospital stay were also compared. The procedure was considered successful if the patient was free of targeted calculi. Postoperative evaluation of stone-free status was assessed at 3 months by means of either a CT scan (3 patients) or radiography of the kidneys, ureters, and bladder plus kidney US (5 patients). The incidence and types of complications were evaluated using the modified Clavien grading system, 9 with special attention to bleeding and adjacent organ injuries. Bleeding was considered a complication when it was severe enough to quit the procedure and/or necessitate blood transfusion and/or further intervention. Stone analysis was performed with infrared spectroscopy.
Results
Table 3 summarizes intraoperative and postoperative parameters. Eight patients who were affected by spinal curvature underwent 10 PCNLs on nine renal units (1.1 PCNL/renal unit). Multiple accesses were performed in two cases (cases 4 and 8; ie, that is, 1.33 access/renal unit and 1.2 access/PCNL). All accesses were subcostal. The mean operative time was 103 minutes (range 90–240 min), and the mean hospital stay was 13.2 days (range 4–32 d). There were three struvite stones, three calcium oxalate monohydrate stones, one brushite, one mixed uric acid and brushite stone, one mixed calcium monohydrate-dihydrate and phosphate stone.
PCNL = percutaneous nephrolithotomy.
The overall success rate for complete stone clearance (absence of any fragments) per kidney after one PCNL was 55.5% (5/9 PCNLs) and 66.6% (6/9 PCNLs) after a second PCNL. Of the kidneys with residual stone fragments, cases 2 and 4 had 5- to 6-mm fragments; case 7, a 10-mm fragment; and case 8 had intact stone after the first PCNL. All of these patients had further stone treatments. Overall, four of nine (44.4%) renal units needed auxiliary measures after one PCNL: Cases 2 and 4 underwent one shockwave lithotripsy (SWL) treatment, case 7 underwent one retrograde intrarenal surgery (RIRS), and case 8 had a combined simultaneous PCNL and RIRS. At the 3-month follow-up, the overall stone-free rate was 88.8% (eight renal units) (Table 1).
Overall, there were four complications in 10 PCNLs (44%); one grade 1 complication (case 6)—the patient presented with transient fever with no need for additional antibiotics other than prophylactics; two grade 2 complications (case 4) because of fever that necessitated additional antibiotics and one blood transfusion; and one grade 3a complication (case 7) because of perioperative bleeding that necessitated quitting surgery, superselective angiographic embolization, and transfusion of 6 units of packed red blood cells.
Overall, the blood transfusion rate was 20%. We did not observe any injury of surrounding organs or pneumothorax.
Discussion
The treatment of urolithiasis in patients with abnormal body habitus, such as morbidly obese or spinal cord injury patients, presents severe, unique challenges for the urologist because of technical difficulties and a higher rate of complications, often necessitating creativity and innovation. 4 –8
Spinal deformity (scoliosis, kyphosis, or kyphoscoliosis) is caused by the pathologic curvature of the thoracic and/or lumbar regions of the spine. It is estimated that scoliosis affects 2% of women and 0.5% of men in the general population, although rates may vary quite significantly based on the specific definition of scoliosis and which patient population is being studied.
There are many causes of scoliosis, including congenital spinal deformities, genetic conditions, neuromuscular problems (cerebral palsy, spina bifida, muscular dystrophy, spinal muscular atrophy, spinal cord injury, tumors), and limb length inequality. More than 80% of scoliosis cases, however, are idiopathic and occur in otherwise healthy people. Hip ankylosis and pelvic tilt are often associated with spinal deformities. In addition, pulmonary function can be markedly affected. 10 In our study, there were five patients affected by idiopathic scoliosis and three by neuromuscular scoliosis (spinal muscular atrophy in case 6, tetraplegia in cases 7 and 8). Patients with spinal cord injuries may develop stature deformity through the years and may also have a significantly increased risk of urolithiasis because of metabolic changes from immobilization, poorly draining urinary systems, and higher incidence of urinary tract infections. 11
In previous reports regarding PCNL, specifically in patients with stature deformity, there are only case reports 4 or these patients are part of a more generic category of patients defined as “high risk.” 5 Therefore, the specific problems that can be encountered or the proposed solutions are not evaluated thoroughly. In our opinion, patients with spinal deformities and urolithiasis who are undergoing PCNL should be considered a special category, because even if there are some common risks and issues with other comorbidities such as obesity or paraplegia, these patients present unique and extreme anatomic variations that require a different approach in planning and performing percutaneous procedures.
Approach to PCNL in patients with spinal deformity
PCNL in patients with spinal deformities may be challenging and risky. We identified three major issues that should be addressed before undertaking percutaneous surgery in this population: Anesthesiologic and cardiorespiratory issues, patient position on the operating table, and percutaneous access modality.
Anesthesiologic and cardiorespiratory issues
Anesthesia-related difficulties depend on the type and severity of skeletal deformities and may be exacerbated by the use of the prone position during PCNL. 12 In the case of severe scoliosis, and particularly in cases of involvement of the dorsal region (kyphoscoliosis), respiratory dysfunction from the altered conformation of the rib cage frequently occurs (Fig. 4) because of restrictive lung disease with reduced lung volume, total lung capacity, vital capacity, or resting lung volume, and eventually impaired ventilatory function, atelectasis, and ventilation-perfusion mismatch. 13 Five of eight patients had respiratory dysfunction and underwent respiratory function tests, arterial blood gas analysis, and further pneumologic evaluation. If the American Society of Anesthesiologists score was III or more, cardiac US was also performed to estimate cardiac index.
Moreover, spinal deformities may cause difficulties with tracheal intubation. 1 The type of anesthesia and patient positioning during PCNL have to be evaluated carefully. In our series, all patients underwent general anesthesia with tracheal intubation. There were no anesthesia-related, pulmonary, or cardiovascular complications, even in patients with preoperative ventilatory dysfunction. The supine position of the patient during PCNL allows better airway control and improved ventilation. Manohar and associates 5 assessed PCNL efficacy in a population of 62 high-risk and morbidly obese patients and stated that PCNL in a supine position achieves better airway control and fewer ventilatory problems.
In our series, we performed five supine and five prone PCNLs, and none of the procedures was interrupted for cardiorespiratory problems.
Even if there are clear advantages for respiratory function with the patient supine, we cannot state that prone PCNL in patients with spinal deformities is contraindicated and that supine PCNL is always the best choice, because there are also other factors that determine the final choice for patient positioning.
Regional anesthesia can be a valid alternative to general anesthesia in patients who are undergoing PCNL 14 and can be very useful in high-risk patients. 15 Even if spinal or epidural anesthesia is technically feasible, 1 it can be extremely challenging in patients with scoliosis because of the profound anatomic changes of the spine. Furthermore, the prone position with regional anesthesia in this population may present great risk because it offers poor airway control and it could be problematic if sedation or conversion to general anesthesia is necessary. 16
Patient positioning
The patient's position is crucial for PCNL, because the area of access is limited, especially in patients with abnormal body habitus. Furthermore, because of the extreme curvature of the spine, often associated with pelvic tilt and hip ankylosis, it may be troublesome to position and to stabilize the patient on the operating table. 4
Sometimes it may be easier and more natural to position a patient with stature deformity in the supine or lateral decubitus position. On the other hand, this may cause difficulties for percutaneous access, especially when the stone is located on the concave side of the spine, which may leave the space between the ribs and the iliac crest dramatically reduced. In fact, the prone position provides a larger area for percutaneous renal access and a wider space for instrument manipulation. 17
Supine PCNL has less risk of postural damage, an important issue in these patients because there is no need to change the position of the patient from supine to prone during the operation, and prolonged pressure on the forehead, knees, and toes is avoided. In addition, if necessary, a more familiar approach for simultaneous ureteroscopic access is readily obtained, allowing combined PCNL and ureteroscopy for management of complex stone disease.
We performed PCNL using both the prone (five procedures) and the supine (five procedures) position. Soft bolsters, cushions, or silicone rolls were used to protect the pressure points and fill the empty spaces between the patient's body and operating table (Fig. 5). The choice between the supine and the prone position depended on the experience with the supine PCNL, the difficulty in accessing the kidney based on the side of the kidney involved with respect to the concave side of the spine, the cardiopulmonary status of the patient, and the stone burden.
The main advantage of the supine position in our experience is its versatility, which allows a combined percutaneous and ureterorenoscopic approach to the kidney, useful in complex cases in which the creation of multiple tracts is difficult because of the anatomy of the renal cavities, in cases where a flexible nephroscope cannot reach the stone because of the angulation of the calyx, or in case of an abnormal body habitus. 18 –20
Percutaneous access
The access to the pelvic system via the desired calix is the most important step during the entire procedure, and the success of PCNL is critically dependent on achieving suitable percutaneous access. The renal puncture can be made under US, fluoroscopic, or CT control. 21 Certain clinical situations may require special access techniques. The emergence of CT as the imaging modality of choice for detecting renal calculi and the ability of CT urography with or without three-dimensional reconstruction to delineate the collecting system makes this the most versatile and sensitive imaging modality for preoperative and postoperative evaluation. 22
In our series, an accurate preoperative evaluation of patient anatomy was a priority. The rotation and curvature of the spine caused modifications of the anatomic relationships between the ribs and the spine, kidneys, and surrounding organs and limited the percutaneous exposure of the renal cavities (Fig. 4). In this situation, there was great risk of visceral injury during the puncture of the renal cavities. We believe that CT with intravenous contrast in patients with spinal deformities is the best imaging modality because it accurately defines all the anatomic changes and details and helps in planning the puncture.
Despite this, the first three patients were evaluated only with IVU. This happened for two reasons: First, in the past (late 1990s), CT was not always available at our institution, and it was not considered a first-line imaging modality for stone disease; second, some of the patients were previously evaluated elsewhere with IVU, so we figured that CT may expose the patient to a repeated high dose of radiation.
To overcome the problem of evaluating the surrounding organs in these cases, we used US preoperative and intraoperative planning of the tract. The US-guided fluoroscopic adjusted puncture through the cup of the desired calix offers many advantages, allowing the surgeon to safely identify the kidney and the pelvic system, as well as surrounding organs, to avoid visceral injury and permit a peripheral puncture; it also permits the surgeon to traverse minimum cortical tissue, establish the shortest straight tract between the skin and calix, and minimize radiation exposure. 23 –25 All punctures were performed by one experienced urologist (EM) and, as stated in other reports, we believe that the puncture and the access should be performed by an experienced urologist rather than a radiologist. 26
Access for PCNL using conventional fluoroscopic guidance may carry an increased risk of damage to surrounding organs in patients with renal calculi and aberrant anatomy. Matlaga and colleagues 27 successfully performed four percutaneous nephrostomies under CT guidance, used because of severely distorted patient anatomy that was associated with spinal dysraphism. The authors stated that CT offers cross-sectional imaging with precise anatomic details; therefore, there is a select group of patients who would benefit from CT-guided percutaneous access for safe and effective PCNL. We agree with these advantages, but believe that CT-guided puncture may be less available because it requires a two-step procedure, exposes the patient and the physician to more radiation, and depends on a radiologist being present.
Complications
The total complication rate of PCNL is reported to be between 3% to 18% and 83% and is generally attributable to inadequate patient selection, lack of adequate treatment, and technical errors. 28 Renal bleeding after percutaneous surgery is common, and according to previous reports, 1% to 23% of patients need a blood transfusion. 28 Severe hemorrhage with symptoms such as hypotension, shock, or renal insufficiency that necessitate intervention, however, may occur in <3% of patients. The frequency of other major complications is reported as 0.9% to 4.7% for septicemia, 2.3% to 3.1% for pleural injury, and 0.2% to 0.8% for colonic injury. 28
In patients with dysmorphic body habitus, the difficulty of percutaneous access and the frequent presence of respiratory dysfunction may be issues with most PCNL complications. In the literature, there are very few reports that specifically report the complication rates in patients with stature deformities. Lawrentschuk and coworkers 8 performed 54 PCNLs in 26 patients with spinal cord injuries, a population with a higher risk of postoperative complications than ambulatory patients. 6 Major complications occurred in 12% of the patients or 6% of PCNLs (two pneumothorax, one urosepsis). Minor complications occurred in 77% of the patients, with most (58%) being a postoperative fever that resolved with no extension of routine perioperative prophylactic antibiotic use. The blood transfusion rate was 6%. Manohar and associates 5 treated 62 high-risk patients with PCNL. Among them, two patients had hip ankylosis, but no complications were reported for these two patients. Gofrit and colleagues 4 treated one patient with severe kyphosis with PCNL. A nephrostomy tube was first inserted, and after 2 years, an uneventful PCNL was performed.
In our series, we had an acceptable overall rate of complications (ie, 4 complications in 10 PCNLs [40%]), classified by the modified Clavien grading system as 10% grade 1, 20% grade 2, and 10% grade 3a. Overall, the blood transfusion rate was 20% for 10 PCNLs. Interestingly, there were no injuries of surrounding organs or anesthesia-related complications. Tefekli et al. 9 in their report stated that the more significant complications graded as Clavien 3b and 4 are quite rare and are related to anatomic as well as technical factors and coexisting medical disorders.
In our series, we observed a higher rate of severe renal hemorrhage than usually has been reported and an acceptable rate of blood transfusion, although it seems high when compared with the relatively low mean stone burden. Even if the number of cases is low and we cannot draw definitive conclusions, our impression is that in patients with spinal deformities, there is a higher risk of bleeding during PCNL, and this is caused mainly by the difficulty of percutaneous puncture because of the deformity itself.
Indications and Outcomes
In the present series, PCNL was performed in patients who were affected by spinal deformities with a mean stone burden of 372 mm2. In four patients with pyelic calculi, the mean stone burden was 137 mm2, which is lower than the usual cutoff value of 300 mm2 for performing PCNL. 2 The decision to perform PCNL in these patients was based on the presence of symptomatic hydronephrosis (pain and/or infection) and because we believed that other treatment modalities such as SWL, RIRS, or surgery may not offer the same advantages as the percutaneous approach in this population of patients. In one patient with a 160-mm2 pyelic stone, SWL was first performed because of patient preference.
The stone-free rate of 66.6% after PCNL is lower than the stone-free rate of 74% to 83% reported by the American Urological Association (AUA) Urolithiasis Guidelines Panel, 29 especially if we consider that only 33% of the cases in our series had staghorn calculi. Based on panel data, the need for further PCNL procedures varies from 10% for simpler stones to up to 50% for more complex stones, and patients average 1.3 PCNL procedures. Combining primary, secondary, and adjunctive procedures on average, PCNL requires 1.9 total procedures while combination therapy and SWL requires 3.3 and 3.6 total procedures, respectively.
We believe that the lower stone-free rate and the high rate of auxiliary procedures (considering also combination therapy as an adjunctive procedure) in our series is caused mainly by two factors. First, the number of patients was limited and included patients who were treated with PCNL over a 10-year period. In the beginning, there was a lack of experience with the stone treatment in patients with spinal deformities, and flexible instruments were not available. Second, as we have mentioned, patients with spinal deformities represent challenging cases from a technical point of view. The AUA panel states that standards, recommendations, and options for the treatment of patients with staghorn calculi apply to an “index patient,” and one of the criteria to define an index patient is a normal body habitus. Because of the deformity, the initial puncture of the renal cavities may not be the ideal one, and this fact, in our opinion, is the main reason for difficulties reaching the stones and a higher risk for hemorrhagic complications, which ultimately affects the stone-free rate. On the other hand, combination therapy with SWL or RIRS improved outcomes in our experience.
SWL as a first-line treatment in patients with spinal deformity may not be a better choice. Difficulty in localizing renal calculi for SWL may be encountered in patients with spinal bifida and spinal cord injury, who have significant spinal curvature. Because of problems in the positioning of a patient with marked curvature of the spine and pelvic tilt, and consequent difficulties in accurate localization of renal calculi for lithotripsy, these patients may be at increased risk of renal parenchymal and vascular damage developing after SWL. 7 Still, two patients underwent one post-PCNL SWL treatment and, despite some difficulties in localizing the stone, fragmentation and stone clearance were optimal. We believe that for small residual post-PCNL fragments (diameter <1 cm) SWL treatment may still have a role if used with caution—hence, avoiding multiple treatments or aborting the procedure if serious difficulties of stone localization are encountered.
There is still a debate as to whether RIRS can be considered a first-line treatment for patients with renal stones. According to the European Association of Urology and AUA guidelines there is a lack of data to indicate such a recommendation. 2,29 Nevertheless, there are several reports from various authors that flexible ureteroscopy with holmium laser lithotripsy is a minimally invasive treatment modality that can be used to manage large intrarenal calculi (stone dimensions larger than 2 cm or even 4 cm) with the potential to decrease morbidity, while maintaining a high level of efficacy. 30 –32
One of the main indications for RIRS is an abnormal body habitus, as with morbid obesity or musculoskeletal deformities. A disadvantage of ureteroscopy is that multiple procedures may be necessary to clear a large stone, and a stent is usually placed postoperatively. 29 –31
Another treatment option for complex cases is a simultaneous combined PCNL and flexible ureteroscopy, because it reduces the number of access tracts and the morbidity of the percutaneous approach. 18 –20,32 In our series, one patient had an incomplete PCNL because of major bleeding and underwent flexible ureteroscopy as a second procedure, which yielded complete clearance of a 1-cm residual stone. A second patient had a PCNL in which the percutaneous tract was inadequate for stone removal, although we used a flexible nephroscope. A simultaneous combined percutaneous and ureteroscopic approach was performed later: First, a laser lithotripsy was performed via the ureteroscope and the fragments subsequently were dislocated in the pelvis and removed via the percutaneous tract. With this approach, we achieved complete stone clearance.
With advances in SWL and endourologic surgery, the indications for open surgery have markedly declined. Nevertheless, there are some clinical situations in which open surgery may still be applied, such as in patients with skeletal deformities, contractures, and fixed deformities of hips and legs. 2 Satoh and coworkers 33 proposed a modified retroperitoneal approach to the kidney in patients with a highly deformed thorax, obtaining a wide operative field through subperiosteal resection of the 10th, 11th, and 12th ribs.
The final decision for the kind of treatment may also depend on the invasiveness of the procedure. For any given stone situation, it is logical to select a method with the lower invasiveness and morbidity. 2 In patients with spinal deformities, the invasiveness of surgery may be excessive and, in our experience, it was not necessary to choose an open surgical approach. Laparoscopic surgery may be another attractive option, but it is a highly specialized skill and should be performed by surgeons trained in the technique, in well-equipped, dedicated centers. 2
Conclusion
A retrospective study was undertaken to determine the effectiveness of PCNL in patients with spinal deformities. The limited number of cases—eight patients with nine renal units, and 10 PCNLs—makes it impossible to draw definitive conclusions and recommendations. In spite of this, as far as we know, this is the first study that specifically deals with the percutaneous treatment of kidney stones in patients with spinal deformities. The treatment of renal stones in such patients is complex. Indications are not clear and are based on personal experience. Issues such as respiratory dysfunction, difficulty in positioning and stabilizing the patients, and profound anatomic variations are the main contributors to the complexity.
In a small number of patients, we demonstrated that PCNL is challenging but feasible in experienced hands. Accurate preoperative evaluation of the anatomy and respiratory function, together with precise and extensive planning of the procedure are mandatory. US-guided puncture of the collecting system offers many advantages, allowing the surgeon to safely identify the kidney and the pelvic system, as well as surrounding organs, avoiding visceral injury. The best position for PCNL cannot be defined from our data. Supine PCNL seems to offer more advantages in terms of comfort of the patient, protection of the cardiorespiratory function, and the possibility to perform easier a simultaneous combined ureteroscopic approach, although the prone position, if feasible with the patient's body habitus, may offer a wider space for the percutaneous access.
Outcomes may be suboptimal with a lower stone-free rate and a higher incidence of bleeding, but PCNL still has a significant role in the management of larger stones in this population of patients, and combination therapy with either SWL or RIRS still has an important role in improving stone-free rates.
Footnotes
Disclosure Statement
No competing financial interests exist.