
Abstract
Background and Purpose:
This is the third publication that updates clinical outcomes using a novel technique to apply locoregional hypothermia to the pelvis during robot-assisted radical prostatectomy (RARP) to reduce inflammatory injury. This report updates urinary and sexual clinical outcomes with a minimum of 1 year follow-up.
Patients and Methods:
Regional pelvic cooling (<30°C) was achieved with a prototype endorectal cooling balloon (ECB) during the course of RARP. All clinical data were entered prospectively into an electronic database for historic (cases 1–666) and hypothermic groups (115 pts). Urinary and sexual outcomes were obtained using self-administered validated questionnaires. Continence was defined as no pads, and potency was defined as two affirmative answers to “erections adequate for penetration” and “were the erections satisfactory.”
Results:
Six patients were excluded: three ECB malfunction, three previous radiation/surgery. Median time to zero pad use was 39 days vs 62 days (hypothermic vs controls, P = 0.0003). At 1 year, overall pad-free continence was 96.3% (105/109) vs controls of 86.6%, P < 0.001. Potency was evaluated in all men (40–78 years) with preoperative International Index of Erectile Function-5 scores of 22 to 25. At 3 months, potency results were unchanged between groups: 24% vs 23%. At 15 months, the potency rates were significantly better for the hypothermic group, 83% vs controls 66%, P = 0.045. No difference in oncologic outcome was noted with cooling.
Conclusions:
Using a prototype cooling balloon, hypothermic RARP significantly improved time to continence and overall continence. Hypothermia also resulted in a modest but statistically significant improvement in potency at 15 months. Once cooling parameters have been optimized, a randomized multicenter clinical trial will be needed for validation.
Introduction
We hypothesized that a contributing factor to the delay in recovery of postprostatectomy continence and potency was because of inflammatory reaction secondary to surgical trauma, such as mechanical forces and thermal energy. This is the third publication of our ongoing experience using local pelvic hypothermia to reduce inflammation resulting from pelvic surgical trauma. In our initial publication with 50 patients, we noted a reduction of median time to continence from 60 days to 38 days. 12 Our second article updated and expanded this experience with hypothermia and its impact on continence in the initial 115 patients using a prototype endorectal cooling balloon (ECB). 13
Beginning with patient 116, we began using a standardized, manufactured ECB and a cooling console approved by the Food and Drug Administration (data not presented in this series). We have now accrued long-term follow-up since the introduction of hypothermic RP 2 years ago; here we report on the long-term follow-up of the first 115 patients, (minimum of 1 year, maximum of 2 years), allowing for a more complete analysis of time to continence and overall continence. In this report we also present our first formal evaluation of potency outcomes with hypothermia.
Patients and Methods
Locoregional hypothermia of the pelvis has been described previously using an ECB and cold intracorporeal irrigation. 12,13 During our initial experience (cases 667–739), hypothermia was initiated before nerve sparing and continued until completion of the vesicourethral anastomosis. As our technique evolved, we cooled for longer periods. Specifically, cooling was initiated preemptively—after intubation but before incision (case 740–781). Hypothermia was often transiently discontinued during rectal dissection or creation of the anastomosis because of space limitations; cooling was restarted during lymph node dissection or inguinal hernia repair (when indicated) and continued until the patient was ready to be transported to the recovery room. In addition, throughout the dissection of the neurovascular bundle (NVB) or when thermal energy was used during other portions of the case, active cold irrigation was used concurrent with cautery to minimize collateral thermal spread.
One hundred and fifteen patients were evaluated with the initial prototype ECB (February 2008–December 2008). Hypothermia was successfully achieved and maintained in 112 of the 115 patients. Six patients were excluded; three because of ECB malfunction and three for clinical reasons (two, previous radiation therapy; one, previous incomplete prostatectomy), leaving 109 for analysis. The control group for continence included our initial 666 patients who underwent normothermic robot-assisted radical prostatectomy (RARP).
Potency outcomes at 3 and 15 months in the hypothermia group were compared with 157 matched controls (age and normal International Index of Erectile Function [IIEF-5] scores of 22–25) selected from cases 168 to 666. Standard baseline clinical characteristics such as age, IIEF-5 score, American Urological Association Symptom Score, urinary bother score, body mass index, prostate specific antigen, pathologic parameters Gleason score, clinical T-stage, prostate weight, and intraoperative variables (ie, estimated blood loss (EBL), nerve sparing, cooling depth and duration) were collected from data that were entered prospectively into an electronic database. This study was undertaken with the approval of our Institutional Review Board. The technique was standardized, because it was performed by one surgeon (TA). Independent statistical analysis was performed by a clinically removed third party biostatistician (KO). Baseline characteristics between the hypothermia group and the control group were analyzed with unpaired two-tailed t tests. The Kaplan-Meier method was used to calculate the time to zero pads; the log-rank statistic was used to assess for differences. Multivariate modeling (Cox proportional hazards regression) was performed to examine the impact of baseline characteristics, learning curve bias, and change in operative technique (posterior urethral plate reconstruction - Rocco). Statistical Analysis Systems software was used (SAS, Cary, NC) with statistical significance set at P < 0.05.
Continence was strictly defined as the use of no pads. Patients needing any security pad or liner were considered incontinent. Urethral catheters were removed on postoperative day 7 in all patients. Continence was assessed by a validated patient self-administered questionnaire. In addition, patients were sent home postoperatively with self-addressed postcards to be mailed on the date when they became pad free. Patients also reported pad status on validated self-administered questionnaires longitudinally at 3, 6, and 12 months. Patients were contacted by telephone if they were not responding to either of the above means.
Qualitative assessment of potency was defined by affirmative responses to two questions: (1) “Do you have erections adequate for vaginal penetration?” (2) Are the erections “satisfactory”? Quantitative assessment was evaluated by IIEF-5 scores.
Results
Patient baseline characteristics are listed in Table 1 for the control and hypothermia cohorts. There was no statistically significant difference in EBL, hospital stay, or complications between groups. For three patients, the ECB leaked or failed to cycle properly. There were no complications related to ECB placement or use such as rectal injury. In addition, there were no patient reported complaints of rectal pain, urgency, fecal incontinence, or bloody bowel movements. In addition, all respondents reported either “no problem” or “a very small problem” with overall bowel habits, consistent with control group responses. There was no difference in overall positive surgical margin rate between the cooling and noncooling cohorts (Table 2).
Data presented as mean (standard deviation) or percentages.
AUASS = American Urological Association Symptom Score; IIEF-5 = International Index of Erectile Function; PSA = prostate-specific antigen; BMI = body mass index.
One patient was censored for undergoing salvage prostatectomy after cryosurgery.
Six patients were excluded because of inadequate cooling.
We modified our surgical margin (SM) technique (Borin 34 ) at case 251. Table 2 presents the +SM rate for three groups: Early technique cases 1 to 250, current technique noncooled cases 251 to 666, and hypothermia cases 667 to 781. The overall margin rate for the entire series was 12.1% (94/774), pT2 = 5.6% (31/556), and pT3/T4 = 28.9% (63/218). The +SM rate for hypothermia is similar to the noncooled technique described by Borin and associates. 34 Note that all six of the excluded hypothermia patients had negative margins.
Continence
We previously reported that in men who were undergoing hypothermic RARP (hRARP), the median time to continence was significantly reduced from 62 days in controls to 39 days. These data were reconfirmed in the present study. Over a minimum of 12 months of follow-up, 105 of 109 (96.3%) who underwent hRARP achieved 0-pad status compared with 86.6% of the control group (Fig. 1, P < 0.001). To ascertain the impact of age on continence, we stratified the cohorts into quartiles. Figure 1 depicts continence rate vs age by decade for both groups and demonstrates significant risk of permanent incontinence with advancing age in the control group. Continence improved to approximately 95% across age groups in men who underwent hypothermia; the most profound difference was observed in the 70+ age group (73% vs 92%).
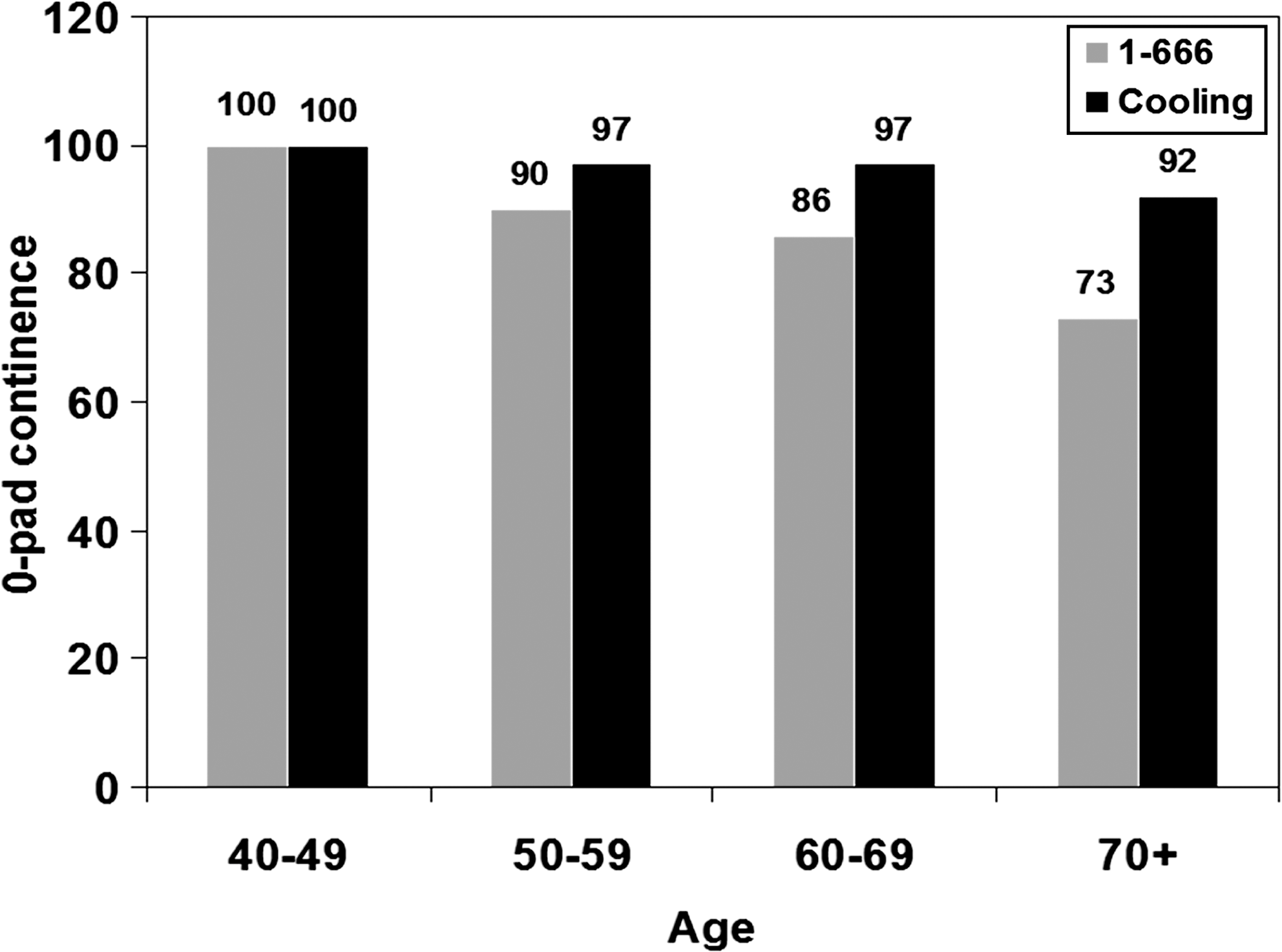
Long-term (minimum 12 months) zero-pad continence rates—control vs cooling groups.
Potency
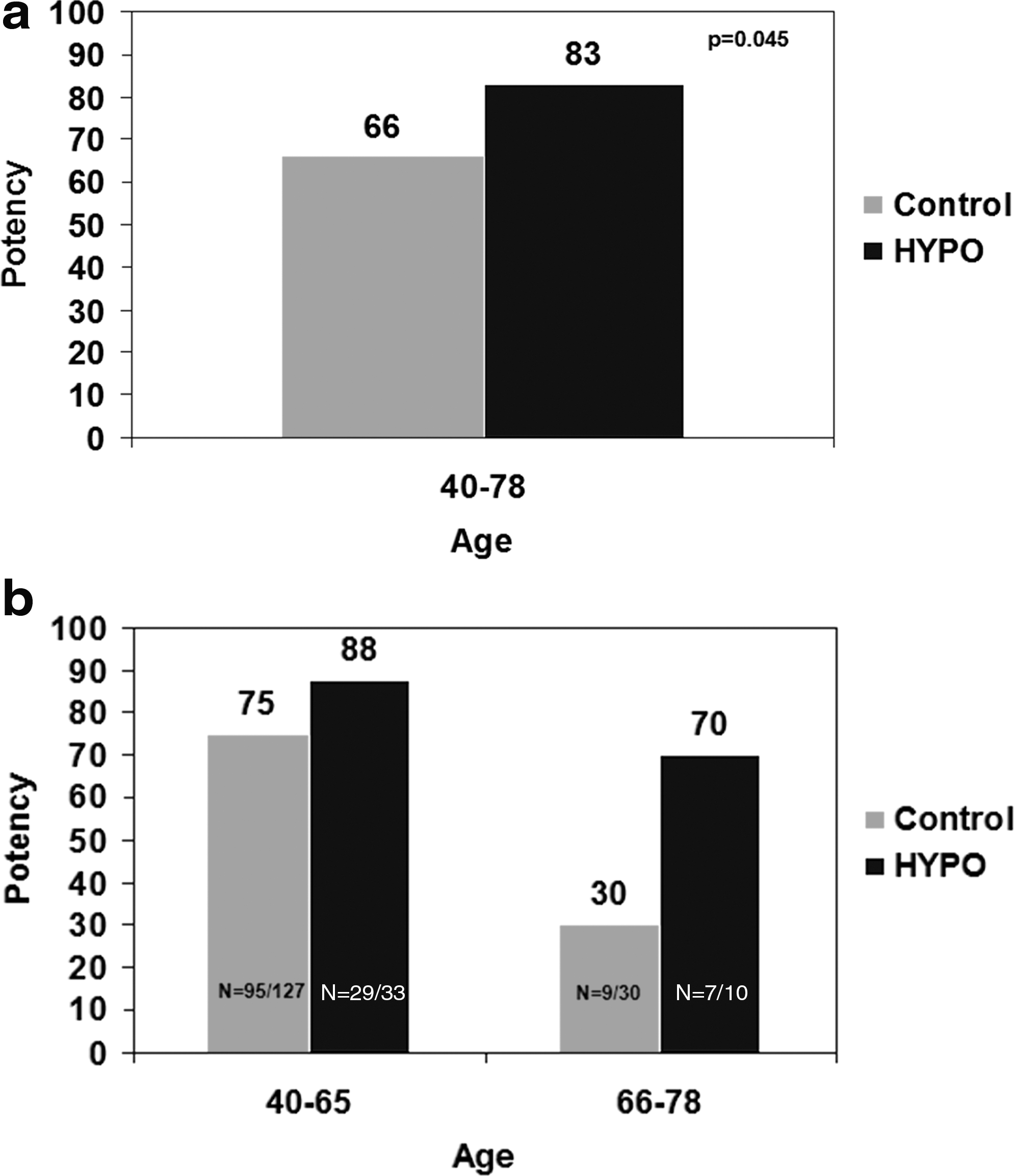
No difference in early potency rates at 3 months was observed between groups (Fig. 2). Among all prepotent men (ages 40–78) (ie, normal preoperative IIEF-5 scores of 22–25), over a median follow-up of 15 months, there was a statistically significant increase in potency recovery from 66% to 83% (P = 0.045) with the use of hypothermia. Subanalysis revealed a modest improvement in men 65 years and younger (75% vs 88%). Consistent with our continence results, however, older men (eg, 66–74 years) experienced a much more obvious benefit from hypothermia, achieving twofold higher potency rates of 70% compared with 30% of controls, (P = 0.06).

Potency outcomes at 3 months—control group (matched for age and normal International Index of Erectile Function-5 scores) vs hypothermia.
Discussion
This is the third and final communication that specifically addresses our pilot findings with hypothermia using our initial prototype ECB. In our first publication, we presented the rationale for hypothermia and demonstrated that we could cool the pelvis reasonably well (<30°C) without complications or patient discomfort. Based on the overwhelming basic science and clinical literature that demonstrates the beneficial effects of hypothermia in essentially all organ systems, we found evidence of quicker recovery of continence that was clinically and statistically apparent after analysis of just 50 patients. One might query, why continence? From a practical viewpoint, every man who undergoes RP places high importance on getting off urinary pads, whereas potency is not a prime focal point.
From a thermodynamic view, muscle is much easier to cool than the NVB because of blood supply. Intraoperatively, we could feel excellent cooling of the muscles of the perineum when giving perineal pressure during the anastomosis. When cutting muscle, there is limited bleeding because there are only the occasional small arteries. In contradistinction, the nerve fibers in the NVBs are just microns in size and are constantly supplied by warm blood pumped in via 2 to 4 mm arteries and 4 to 7 mm veins.
Our second publication expanded and confirmed our initial findings regarding time to continence in the 115 patients who were cooled with the prototype ECB. There was some evidence that longer and colder cooling was better, but these findings were not statistically significant, which may have been because of inadequate statistical power or true lack of thermodynamic effect. Importantly, in that series, we had not accrued sufficient follow-up to comment on potency.
Continence
The present report reveals a new important finding regarding overall continence. Of the 109 men evaluated, 96.3% (105/109) became pad free (Fig. 1) vs just 86.6% in the controls (P < 0.001). Based on age-adjusted risk for incontinence derived from our control group, we would have expected 14 incontinent men out of the 109. In addition, we observed that older men (eg, ≥70 years) enjoyed the greatest improvement in overall long-term continence. In other words, all men undergo exactly the same procedure (eg, apical dissection, Rocco plication, and van Velthoven anastomosis) regardless of age, yet as men get older, they do not fully recover from the (trauma of ) surgery and hence have more permanent incontinence. This suggests that hypothermia reduces inflammation. resulting in less overall incontinence.
There is widespread evidence that hypothermia mitigates all inflammatory pathways and improves repair mechanisms. Controlled hypothermia impacts a range of biochemical, histologic, and physiologic effects that include a temperature dependent reduction in cellular metabolism, leading to reduced energy demands, 14 decreased free radical production, 15 interruption of the apoptotic cascade preventing cellular injury from leading to irreversible apoptosis, 16 –20 and perhaps most importantly, decreased inflammation by reducing polymorphonuclear leukocyte invasion and chemotaxis 21 as well as reducing proinflammatory cytokine production. 22 –26
Potency
Neurologic injuries that occur to peripheral nerves were classified by Seddon 27 in 1943 as grade 3, permanent (neurotmesis); grade 2, intermediate (axonotmesis); or grade 1, transient (neurapraxia). 4,27,28 Grade 3 injuries, such as wide excision, transection, partial excision, and incision result in permanent injury when no continuity exists in the perineural tissue for remaining axons to regrow. 4,27,28 In grade 2 or temporary injuries, in contrast, there will be regrowth if the surrounding physical platform of the nerve is preserved. These injuries usually take months for recovery (axonotmesis). Grade 1 injuries are similar in concept to a concussion. The axon is preserved, with mild injury to the perineural tissue, and the tissue recovers in a few weeks (neurapraxia).
Initially, based on patterns of peripheral nerve injury, we had speculated that the number of men with preserved potency seen at 3 months would increase significantly. Specifically, we hypothesized that hypothermia would prevent/convert some of the grade 2, axonometic injuries, to short-lived grade 1 or neurapraxic injuries.
Mechanistically speaking, the hypothermia would have needed to shield the axon from disruption either vascular, stretch, or other mode of injury; as Figure 2 demonstrates, this was not observed. At 15 months, however, we did see significant improvement in potency recovery in men with normal baseline IIEF-5 scores who were aged 40 to 78 (83% hypothermia vs 66% control, Fig. 3a-3b). Thus, in men with grade 2 injuries in which the NVB was preserved, if the patient was young and/or healthy enough, he should recover potency. By contrast, if the patient was not “healthy” enough to tolerate the inflammatory insult because of age or vitality, impotence results. This could account for the increased benefit of hypothermia seen in men as they get older both with continence and potency and supports that cooling reduces the degree of inflammatory injury from surgical trauma, resulting in improved urinary and sexual outcomes.
(
As patients get older, physical deterioration results in tissue repair and remodeling systems that are less efficient and faulty. That is, over time, aging reduces one's ability to cope with injury, increasing the probability and degree of morbidity. In addition, immune responses may be more severe in the elderly. For example, neuroinflammation is more pronounced in the older patients. 29,30 Immune cells in the brain become more reactive with age, creating an exaggerated inflammatory cytokine response after immune activation, leading to more severe long-lasting deficits. 30 –33 Thus, the increased susceptibility to inflammatory damage and a hyperactive inflammatory response, coupled with defective repair mechanisms and overwhelming demands of injured tissue in the setting of compromised blood flow and ischemia, therefore results in a longer recovery and higher overall rate of damage (eg, to the continence and erectile mechanisms) in older patients.
There are a number of weaknesses to this study and pilot and feasibility studies of this nature in general. A primary goal of our study was to optimize (actually, improve is more accurate) procedural issues, and hence, clinical outcomes were not specifically powered (fortunately, continence outcomes were dramatic enough that statistical significance was easily achieved). Procedural issues we focused on included ECB volume and shape to maximize thermodynamic efficacy, depth and duration of cooling, use of adjunctive intracorporeal irrigation, and measurement of both intracorporeal and intrarectal temperatures.
As we continue to explore and optimize our technique based on the findings of the present study, we recognize that confirming temperatures in the NVBs and both the bladder neck and external striated sphincters is paramount. We also will need to determine if longer duration of cooling is practical and if the clinical outcomes are significantly better. Clearly, with optimized technique and a standardized fourth generation cooling balloon driven by a cooling console approved by the Food and Drug Administration, the benefit of hypothermia will need to be evaluated in a well powered, multicenter randomized clinical trial.
Conclusions
We present long-term outcomes of our initial series of patients using a novel ERB for regional hypothermia during RARP to mitigate inflammatory damage from surgical trauma. With at least 1 year of follow-up, the overall continence in the hypothermia group was 96% compared with our controls' continence rate of 86.6%. Potency results at 15 months for all men with normal preoperative IIEF-5 scores improved from 66% in controls to 83% for men undergoing hypothermia. These results are in line with a wide body of literature that supports the benefit of hypothermia as a means to reduce both direct traumatic and inflammatory related injury.
Footnotes
Disclosure Statement
Thomas Ahlering and David Finley are co-inventors of a University of California-owned patent on a device related to this or the subject of this publication. The University of California currently has a licensing agreement with Innercool Therapies, a division of Philips Healthcare. No competing financial interests exist for the other authors.