
Abstract
Background and Purpose:
It is well known that hypothermia protects renal tissue from ischemic damage. So far, no standardized cooling method for laparoscopic surgery has been established. The traditionally used cooling method during open partial nephrectomy (OPN) is crushed ice applied around the kidney; for laparoscopic use, transarterial and transureteral perfusion cooling are described. We compared these three cooling methods with Freka-Gelice (FG), a new gel-like cooling material, and present our initial preliminary results in an ex-vivo porcine model.
Materials and Methods:
To prove cooling effectiveness, FG was compared with superficial crushed ice (NaCl-ice), with transureteral perfusion (TUP), and with transarterial perfusion (TAP) cooling in ex-vivo porcine kidneys. The temperature decrease over 120 minutes and practical application were evaluated.
Results:
No significant difference was found for the mean value distribution at different time points for NaCl-ice and FG (P = 0.18). TUP and TAP showed insufficient temperature decrease. Mean temperatures for NaCl-ice and FG were 4.75°C and 7.02°C at 30 minutes, 0.72°C and 2.47°C at 60 minutes, and −0.19°C and 2.35°C at 120 minutes, respectively. FG was easy to use because of its gel-like consistence.
Conclusion:
TUP and TAP did not provide a fast and sufficient temperature decrease for renal hypothermia in this ex-vivo model. FG shows sufficient cooling qualities comparable with conventionally used NaCl-ice. Because of its gel-like consistence, FG can be used for laparoscopic partial nephrectomy, because insertion through a trocar is possible.
Introduction
We present a promising new material and initial results of inducing hypothermia for OPN and especially LPN by using a gel-like ice: Freka-Gelice. We evaluated the effectiveness of Freka-Gelice with respect to maintaining hypothermia over time. Freka-Gelice was compared with conventional crushed ice, and cold saline transureteral and transarterial cooling in an ex-vivo porcine kidney model.
Materials and Methods
Freka-Gelice
Freka-Gelice is based on nontoxic, modified sterile gelatin and consists of sodium chloride, magnesium chloride, potassium chloride, and sodium lactate; it has a pH between 5.8 and 7.0 and an osmolality of 295 mOsm/kg.
Ex-vivo porcine kidney model
Only freshly sampled porcine kidneys from a slaughterhouse with preserved renal artery, renal vein, and ureters were used. Immediately after slaughter, to prevent venous embolism, the ex-vivo porcine kidneys were arterially perfused through a thin plastic tube (Heidelberger Verlängerung®) that was fixed to the renal artery. The kidneys were perfused over a connected perfusion syringe filled with 4°C cold saline until the blood was washed out, which was checked by a clear color of the perfusate of the renal vein and a kidney color change from red to white. To have baseline temperature in all experimental setups, the porcine kidneys were then slowly heated in a 37°C water bath.
Temperature measurement was performed by a digital multimeter (Keithly Instruments 2001) with thermocouple sensors placed 0.5 cm into the renal parenchyma. To reproduce an intraoperative situation, kidneys with in-placed temperature sensors were packed in a plastic sac like the ones used during OPN.
Experimental ex-vivo setup
Ten kidneys each were covered by crushed ice (−16°C NaCl solution, NaCl-ice) and by Freka-Gelice (FG, −8°C to −10°C); 10 kidneys each were cooled with transureteral (TUP) and transarterial (TAP) saline perfusion (4°C).
For ureteral perfusion, a double-lumen Nelaton 18F Foley bladder catheter (Norta) was inserted through the open end of the ureter up to the renal pelvis where the catheter was blocked with 1 to 3 mL Aqua dest. in the pyeloureteral junction; the right position of the catheter was controlled by palpation of the catheter balloon. Perfusion was performed over a 1-L bag of 4°C cold 0.9% saline (Freeflex,® Fresenius) suspended 100 cm above the kidney. The 1-L bag was connected to a conventional infusion dispositions system. The efflux from the other lumen of the catheter was collected, and a volumetric flow rate of 20 mL/min could be measured.
For arterial perfusion, an infusion extension flexible tube (Heidelberger Verlängerung, with a diameter of 3 × 4.1 mm, Oriplast Gmbh) was cut down, leaving imately 5 cm. The cut end was inserted into the renal artery, placing it approximately 1 cm before entering the kidney. The infusion tube was fixed with suture, so no solution could drain beside the catheter. Perfusion was performed identically as described for transureteral perfusion. The perfusate for the renal vein was collected, and a volumetric flow rate of approximately 16 mL/min could be measured.
Kidney temperature decrease over time every 5 minutes over 120 minutes and practical application have been evaluated.
Results
Freka-Gelice
Freka-Gelice is liquid at room temperature (Fig. 1). Between −3°C to −5°C, the formation of ice crystallization can be observed; even in an ice consistence up to −5°C, it is formable and easy to cut into cubes up to a temperature of −10°C. If it is stored cooler than −12°C, its consistence becomes icelike and is hard to crush. At a temperature of around −2°C, it can be applied through a trocar for laparoscopic use. After warming up to room temperature, it becomes liquid again.
Freka-Gelice (liquid, room temperature).
Ex-vivo setup
The mean temperatures for NaCl-ice, FG, TUP, and TAP were measured as 4.75°C, 7.02°C, 23.8°C, and 23.2°C at 30 minutes; 0.72°C, 2.47°C, 20°C, and 20°C at 60 minutes; and −0.19°C, 2.35°C, 16.8°C, and 18°C at 120 minutes, respectively. Detailed temperature decrease is listed in Table 1. No significant differences were found for the mean value distribution at different time points for NaCl-ice and FG (P = 0.18). The largest decrease in temperature after 120 minutes was found for NaCl-ice and FG, with the lowest mean value of 5.8°C and 4.1°C, whereas for TUP and TAP, this effect was less substantial (22°C and 21°C, respectively) (Fig. 2). FG was easy to handle because of its gel-like consistence.
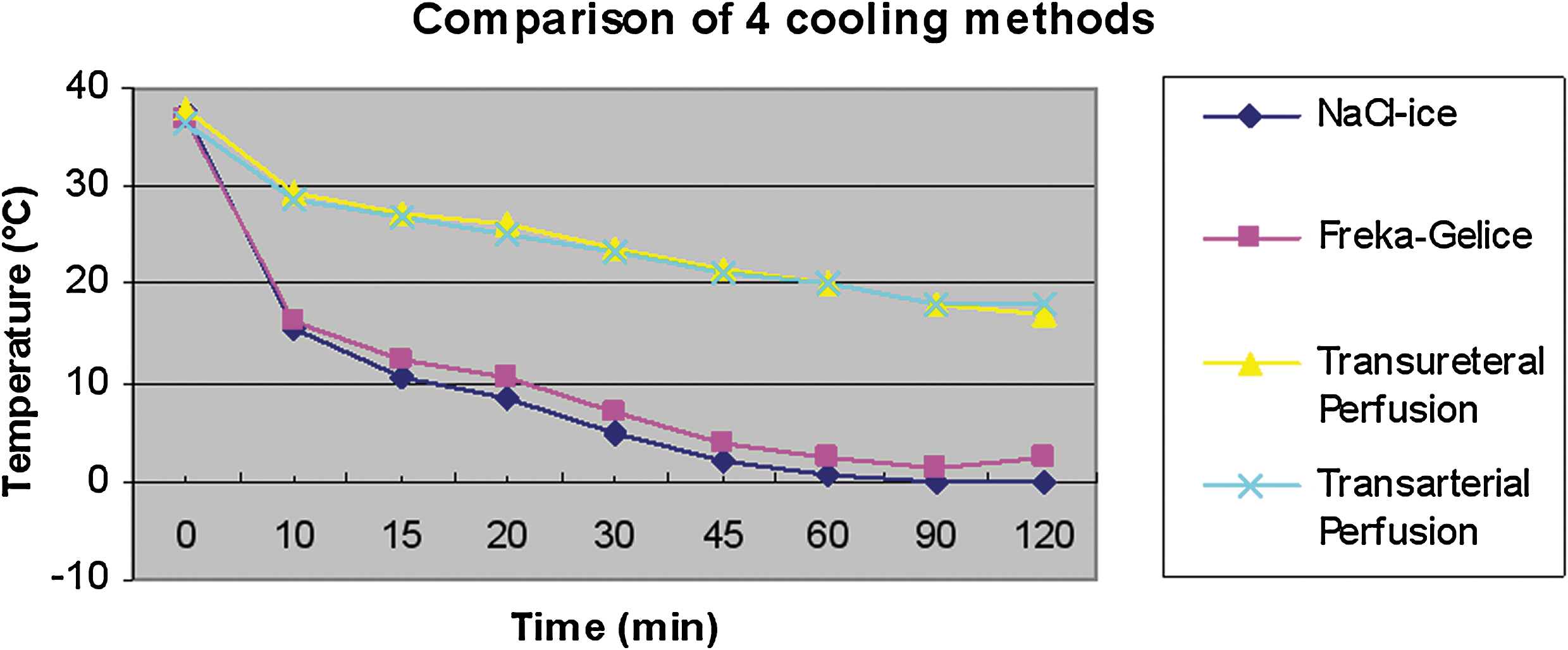
Comparison of temperature decrease over time of the four cooling methods: Conventional ice (NaCl-ice); Freka-Gelice; transureteral perfusion cooling; and transarterial perfusion cooling.
NaCl-ice = conventional ice; FG = Freka-Gelice, TUP = transureteral perfusion cooling; TAP = transarterial perfusion cooling.
Discussion
Since the first laparoscopic partial nephrectomy was performed in a porcine model in 1993, 3 refined techniques and more advanced instrumentation have facilitated LPN as a feasible alternative to OPN. 4 LPN has evolved to copy OPN even for tumors up to 4 cm. 5,6 Despite the apparent advantages in convalescence to patients and recent studies on nephron-sparing surgery demonstrating higher life expectancy because of parenchymal preservation, 7,8 the procedure is technically demanding and therefore recommended in the European Association of Urology guidelines 2007 4 for experienced centers only.
Excision of larger tumors in a bloodless field necessitates longer hilar clamping and prolonged warm ischemia time, which may result in renal failure. It is well documented that renal hypothermia protects the kidney from ischemic damage. 9 A significant decrease in renal metabolic activity occurs when cortical temperature is less than 15°C to 20°C. Rapid immediate lowering of the core temperature of the kidney is necessary to reduce the metabolic activity of the tubular cells, so no anaerobic process can occur. The ischemia time of tolerance in humans without resulting in kidney damage under warm ischemia is accepted as between 20 1 and 30 2 minutes. Under hypothermic conditions, the time of tolerance can be extended up to 35 1 minutes and up to 120 10 minutes in animal models.
The standard method for inducing regional renal hypothermia in OPN is surface cooling with crushed ice. At present, there is still no standardized cooling method for inducing hypothermia during a laparoscopic operation. Several efforts have been made to find the ideal material that could be used easily for a laparoscopic approach, such as surface cooling with ice slush 11 using an Endocatch bag or ice slurry, 12,13 and transarterial 14,15 or transureteral 16,17 cold saline perfusion. These methods, however, emerged as laborious or invasive and therefore are used for selected patients only.
The optimal temperature for regional renal hypothermia during temporary renal ischemia is supposed to be 15°C, 9,18 because renal metabolic activity is almost suspended at temperatures lower than 20°C.
With the conventional surface cooling used during OPN, fast and sufficient cooling could be achieved after 10 minutes in this study. Almost the same results were presented by Naya and associates 19 in a porcine model, where a temperature lower than 20°C could be maintained over 47 minutes. Orvieto and colleagues 13 and Gill and coworkers 11 showed similar good results by laparoscopic use of ice slurry and ice slush, respectively.
Transureteral perfusion cooling in this study did not show a sufficient temperature decrease before 90 minutes, which would not be at all sufficient for renal protection during laparoscopic surgery, where the average clamping time is 30 and 40 minutes for small tumors. 20,21 Naya and associates 19 showed fast and longer temperature decrease over time by combining transureteral with surface cooling. Landman and colleagues 17 present a very fast temperature decrease by transureteral perfusion cooling after 5 to 10 minutes to ∼ 23°C and measured minimum temperatures of 21.3°C. To compare the effectiveness of retrograde “intercavitary” saline perfusion, they used a 12/14F ureteral access sheath over which a 7.1F pigtail was placed into the renal pelvis. Irrigation then was initiated with a 3-L bag of −1.7°C cold 0.9 % saline suspended 60 cm above the kidney, resulting in a circulation of 85 mL/min.
Using a somewhat different infusion method and using an ex-vivo instead of an in-vivo experimental setup might explain the results regarding the different infusion rate of 85 mL/min compared with 20 mL/min in the present study. Higher infusion rates of more than 20 mL/min were not feasible because of high “tissue resistance” in this study. Even the effort of using a circulation pump failed by either overpressure in the pump system or by high pressure in the kidney tissue because the kidney became too hard and resulted in microinjuries of the parenchyma.
Crain and coworkers 16 described similar flow rates through the catheter into the renal pelvis and confirm our results of slow temperature decrease with transureteral perfusion cooling, as a minimum temperature of ∼25°C could be reached after 30 minutes. They used a 10F dual-lumen catheter, with the tip placed in the renal pelvis; 4°C cold saline was infused using a standard intravenous infusion pump running at 999 mL/hr. Martins and colleagues 22 compared surface ice-slush cooling and transureteral irrigation cooling with different flow rates from 5, 10, and 15 mL/min and could not find any significant difference in the renal cortex temperature decrease for each flow rate and confirmed better renal protection with surface cooling.
Steffens and associates 15 and Janetschek and coworkers 14 describe continuous perfusion cooling through the renal artery in the open and laparoscopic approach, respectively. The perfusion was performed over a 16 gauge, 1.7 mm venous cannula with 120 mm Hg pressure, and 50 mL/min over an angiocatheter, respectively. Both studies show the feasibility of arterial perfusion cooling. Apart from the advantage of a bloodless operation field and the outwashing of toxic radicals after reperfusion, this method is associated with additional technical and personal effort (angiocatheter, radiologist, invasiveness).
The results of transarterial perfusion cooling of this study were somewhat unexpected. The mean flow in a single kidney is 642 mL/min ± 190 mL/min 23 ; in our study, the infusion rate could not exceed 16 mL/min. This again might be explained by the tissue or vascular resistance that we observed in transureteral perfusion. Because of unknown reasons, the ex-vivo vascular and tissue resistance must be different to in-vivo vascular and resistance, so that we could not achieve higher perfusion rates.
The results of transarterial perfusion cooling elucidate that the impact of this study is limited because of the ex-vivo setup and cannot easily be adapted to an in-vivo situation, where, for example, the effect of outwashing radicals after reperfusion could be measured.
Conclusion
The ex-vivo experiment shows that Freka-Gelice qualified to be a perfect material for inducing renal hypothermia by surface cooling and therefore enables prolongation of the cold ischemia time. Because of its gel-like consistence, it seems to be perfect for laparoscopic use because it can be applied through a trocar. An extended study on a porcine model is in preparation by our research group to prove the feasibility and effectiveness during intraoperative laparoscopic use.
Footnotes
Disclosure Statement
The research group received financial support from Fresenius Kabi, Germany, by a nonspecific grant. This financial support was reserved to buy study-related materials (ie, porcine kidneys, infusion systems, laboratory material, etc.) and to pay study-related Congress visits and Congress fees.
Congress visits and fees have been paid for Gita Schöppler and Johannes Hell. All the other authors have not received this allowance.
None of the authors received nor will receive financial support related to the profits of selling Freka-Gelice. Fresenius Kabi, Germany, did not have any influence on the results of the study.