
Abstract
Purpose:
To evaluate cases of gallbladder injury, a rare and potentially serious complication, in the setting of percutaneous nephrolithotomy.
Patients and Methods:
We report two cases of gallbladder injury after percutaneous nephrolithotomy and review the literature on this rare complication.
Results:
Both cases of gallbladder injury at our institution along with the four other case reports in the literature all necessitated cholecystectomy. Medial right-sided collecting system access during percutaneous nephrolithotomy may increase the risk for biliary injury.
Conclusions:
Both recognized and unrecognized gallbladder injury may lead to biliary peritonitis necessitating subsequent cholecystectomy.
Introduction
Patients and Methods
We retrospectively reviewed two cases of gallbladder injury after percutaneous nephrolithotomy at our institution. We performed a MEDLINE literature search for all reported cases of gallbladder injury after percutaneous nephrolithotomy to better evaluate risk factors and outcomes in these patients.
Results
Case 1
A 49-year-old woman with a right partial staghorn calculus was scheduled to undergo right percutaneous nephrolithotomy. With consultation, an interventional radiologist performed an upper-pole access into the collecting system without any difficulty, a 30F access sheath was placed, and percutaneous nephrolithotomy was performed without any difficulty. A 16F reentry Malecot was left in place at the end of the procedure, with antegrade contrast injection showing good nephrostomy tube placement and flow into the bladder. The patient did well postoperatively. An antegrade study showed delayed drainage, so the nephrostomy tube was downsized to 8F, and the patient was discharged home on the first postoperative day with plans for a repeated nephrostomy tube study and tube removal within the week.
The patient presented to the emergency department on postoperative day 3 with increased right upper quadrant pain. On physical examination, she was afebrile, tachycardic, and had right upper quadrant tenderness. She had signs of an ileus and was admitted for pain control and hydration. The patient's pain initially improved with her return of bowel function but ultimately worsened with generalized abdominal tenderness on postoperative day 5. CT revealed fluid in the pelvis, the right paracolic gutter, and surrounding the liver as well as gallbladder wall thickening with no gallstones (Fig. 1).

Case 1—CT reveals thickened gallbladder wall with pericholecystic fluid.
General surgery was consulted, and exploratory laparoscopy was performed followed by a laparoscopic cholecystectomy. Intra-abdominal bilious fluid was noted and was suctioned, followed by irrigation of the peritoneal contents. Examination of the gallbladder revealed a hematoma along the mucosal aspect of the gallbladder fundus with a serosal defect marking the puncture site. A Jackson-Pratt drain was left at the end of the procedure.
The patient's remaining hospital course was unremarkable, and she was discharged home after drain and nephrostomy tube removal two days after the cholecystectomy.
Case 2
A 55-year-old woman with a history of bilateral nephrolithiasis was scheduled to undergo right percutaneous nephrolithotomy for a 10-cm right renal stone burden. She had a surgical history of a perforated gastric ulcer with open repair and had recently had a nephrostomy tube placed into the right renal pelvis at an outside institution.
Interventional radiology was consulted to obtain upper-pole caliceal access. The original nephrostomy tube was used to inject contrast followed by air to identify the upper-pole calix. During attempted access of the upper pole, the gallbladder was punctured and opacified with contrast. With the needle in place, 20 mL of bile were aspirated, and the needle was removed. A subsequent attempt at upper-pole access beneath the 12th rib was successful and the tract was dilated, a 30F access sheath was placed, and successful percutaneous nephrolithotomy was performed. A 24F reentry Malecot catheter was placed at the end of the procedure, and injection of contrast showed patency of the collecting system with flow into the bladder. Postoperative chest radiography revealed no pneumothorax.
The patient's postoperative course was complicated by right upper quadrant discomfort that worsened on postoperative day 2. On physical examination, the patient's entire abdomen was diffusely tender, prompting a general surgery consultation.
Abdominal CT revealed retained contrast within the gallbladder, no gallstones, and fluid along the porta hepatis with perihepatic ascites (Fig. 2). Laparoscopy revealed significant intra-abdominal adhesions and bilious ascites throughout the intra-abdominal cavity. A laparoscopic cholecystectomy with peritoneal irrigation was performed. The patient recovered without any further complication, had removal of the nephrostomy tube on postoperative day 3, and was discharged home.
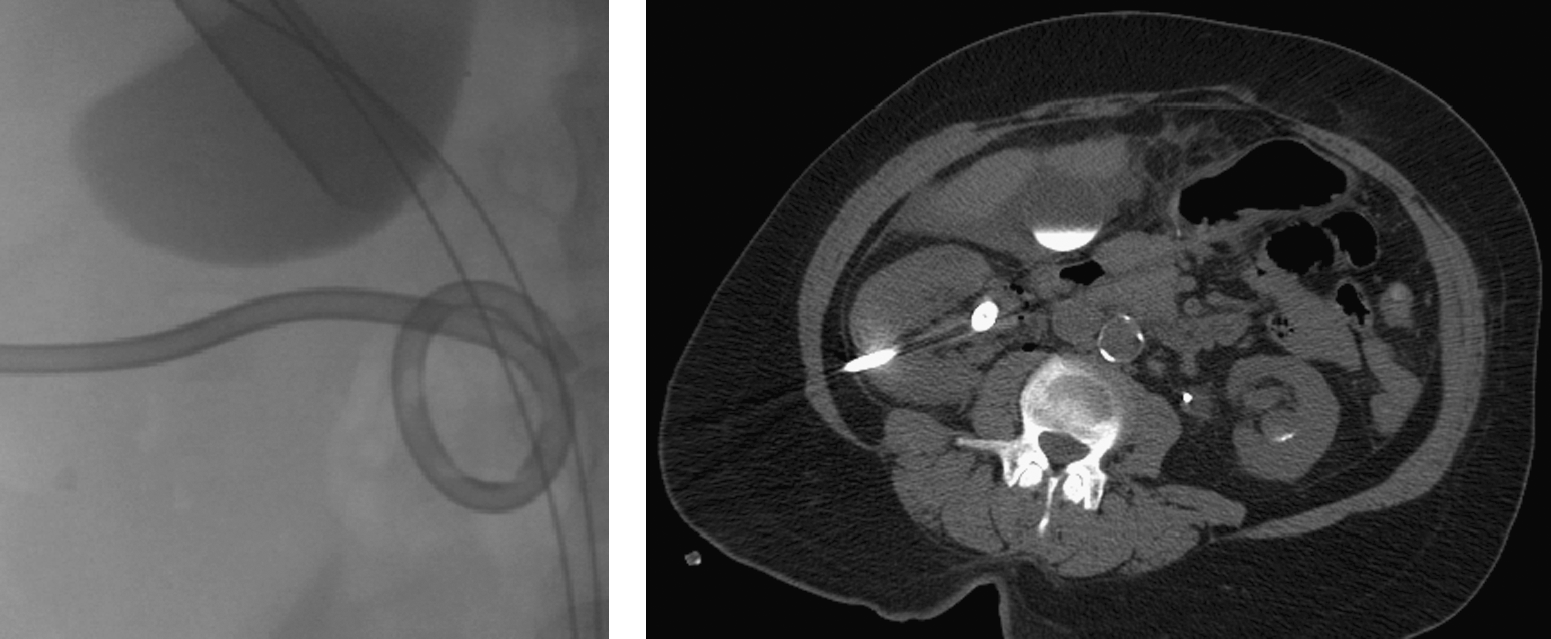
Case 2—(Left) Retained contrast in the gallbladder on fluoroscopy; upper pole access with previous interpolar nephrostomy tube in place. (Right) CT reveals previous residual contrast in the gallbladder along with pericholecystic fluid.
Discussion
Four cases of gallbladder injury during percutaneous nephrolithtomy are reported in the literature with all of the cases necessitating cholecystectomy (three open, one laparoscopic). 1 –4 Biliary peritonitis can be a surgical emergency with a mortality rate of up to 20%. 5 Most authors believe that gallbladder injuries are generally managed by cholecystectomy. 5 Some patients with biliary ascites without peritonitis, however, may be treated with percutaneous cholecystotomy tube placement and drainage.
Chiverton and associates 6 describe a series of 60 patients who underwent percutaneous cholecystolithotomy for the treatment of symptomatic gallstones. Gallbladder access was performed with the patient in the supine position after oral cholecystography, which allowed fluoroscopic localization of the gallbladder, as well as under ultrasonographic guidance. On gallbladder access, bile was aspirated to minimize leakage and subsequent peritoneal irritation; a pigtail drain was left in place for 10 days after treatment of the gallstones. The authors reported two postoperative bile leaks in their series. One was controlled with a percutaneous drain placement into the gallbladder because the initial drain had become dislodged. The second leakage resulted in a subphrenic fluid accumulation that was percutaneously drained. Neither of these two complications resulted in cholecystectomy, which may be attributed to the fact that the patients' gallbladders were drained of bile on access and that a drain was left in place at the end of the procedure.
We present two cases of biliary peritonitis after right percutaneous nephrolithotomy. Both cases resulted in laparoscopic cholecystectomy, highlighting the gravity of gallbladder puncture or injury during the procedure. Both patients' postoperative course was significant for right upper quadrant abdominal pain, eventually developing into peritonitis.
Just as lateral collecting system access (lateral to the posterior axillary line) increases the risk of colonic injury, medial percutaneous access is associated with an increased risk of hemorrhage via injury to the branch of the posterior segmental artery and may also increase the risk of gallbladder injury. 7 –9 The majority of patients with colonic injuries can be treated without open surgical intervention if the penetration is retroperitoneal and the patient does not have peritonitis or sepsis. 7 The intraperitoneal leakage of bile, in cases of biliary injury, leading to peritonitis may not allow for conservative management of this complication.
The location of both of our initial access placements was slightly medial because we targeted the upper-pole calix. The depth of puncture is also an important factor because both of our medial accesses were likely relatively deep in order to injure the gallbladder. Although the details regarding collecting system access in relation to gallbladder injury are not well reported in the literature, gallbladder injury may also occur during a lower-pole access. 4
Conclusions
If gallbladder injury is recognized during collecting system access during percutaneous nephrolithotomy, we recommend that general surgery should be consulted because a cholecystectomy may be necessary. In patients with persistent or worsening right upper quadrant pain after right percutaneous nephrolithotomy, it is important to consider the possibility of an unrecognized gallbladder injury during access, and there should be a low threshold for further imaging of the abdomen.
Disclosure Statement
Dr. Patel has no competing financial interests; Dr. Nakada is a consultant/advisor for Cook Urological.