
Abstract
Purpose:
To present experience with the percutaneous management of iatrogenic ureteral injuries.
Patients and Methods:
Eighteen women and six men with a mean age of 59.3 years (range 33–80 years) received a diagnosis of ureteral injury sustained during gynecologic, urologic, and general surgical procedures. In a total of 25 injured ureters, 12 had interruption of continuity of their lumen, 10 were associated with contrast extravasation, and 3 were related to both. A standard percutaneous nephrostomy tract was established on the side of the afflicted kidney. Combined use of hydrophilic guidewires and balloon dilations were performed to achieve antegrade recanalization of the ureteral lesion. Then, a ureteral stent was inserted to assure patency.
Results:
Average stricture length was 1.21 (range 0.5–1.9 cm). Success of the aforementioned technique was possible in 18 ureters. Successful management in one session took place in 14 ureters. Average hospitalization time was 1.8 days (range 0–5 d). The follow-up period ranged between 12 and 18 months, with mean follow-up time of 12.9 months. Ureteral patency was evident at 1 week follow-up in six patients with obstructed ureters. In the remaining patients, balloon dilation of the stricture was repeated, and another stent was placed. Extravasation of contrast was observed in two patients with extravasating ureters in the same period. Nephrostomy tubes were removed after a mean indwelling period of 5.9 weeks (range 1–12 wks). Two patients treated by the described method died during their hospitalization in the intensive care unit because of sepsis from peritonitis that was related to colon injury and multiple concomitant injuries. Major complications were not observed in the remaining 22 patients during the follow-up period.
Conclusion:
The minimally invasive management of ureteral injuries is a safe and effiecient method for both ureteral obstruction and/or laceration in a wide range of iatrogenic ureteral injuries.
Introduction
Iatrogenic ureteral injuries are associated with accidental ligation, crushing, laceration, avulsion, stretching, and devascularization. 7 The incidence of ureteral trauma increases during technically demanding laparoscopic and ureteroscopic manipulations and oncologic surgery. 2,5,7,8 Ligation of the ureter represents almost 50% of the cases. 3 Although ureteral injury could be recognized intraoperatively and managed appropriately without any sequelae, it can be overlooked, resulting in immediate or late postoperative detection of the lesion. An undetected ureteral lesion is associated with substantial morbidity. 7,9
Several surgical techniques have been introduced for the management of ureteral injuries. These techniques include end-to-end ureteroureteral anastomosis, ureteral reimplantation, or some combinations. 2,3 Recently, laparoscopic reconstruction of ureteral injuries has been introduced, and the experience is continuously expanding. 10,11 Endoscopic minimally invasive approaches represent an option for the management of ureteral lesions and are associated with reduced morbidity and duration of hospitalization. 8,12,13 We have previously reported our experience with 10 cases of gynecologic ureteral injuries managed by percutaneous nephrostomy and primary antergrade recanalization. The technical success was possible in all cases by the endoscopic minimally invasive approach. 14
We report our experience with the management of ureteral injuries that occurred during gynecologic, general surgical, and urologic procedures by the above minimally invasive approach.
Patients and Methods
Eighteen women and six men with a mean age of 59.3 years (range 33–80 years) had ureteral injury sustained during gynecologic, urologic, and general surgical procedures. These patients presented to our institution with symptoms related to hydronephrosis and/or compromised renal function and/or the presence of a retroperitoneal collection of fluid (urinoma). Symptoms included low-grade fever, chills, flank and/or abdominal pain. Oliguria or anuria as well as signs of septicemia were also observed. The patients had undergone procedures for both malignant and benign diseases, and none of the patients had received radiotherapy in the region of interest. Table 1 presents the operations during which the ureteral injuries took place. The ureteral injury diagnosis occurred in four patients from a high degree of clinical suspicion because of intraoperative incidents and findings. Three patients presented with symptoms and signs of sepsis.
All patients underwent blood chemistry examination. Imaging modalities were used to elucidate the presence of ureteral obstruction and/or laceration. The presence of pelvicaliceal dilatation was revealed by ultrasonography while intravenous pyelography and CT urography indicated the site of injury.
A detailed medical history of the patient, including any hypersensitivity to drugs or contrast media, and blood coagulation tests were performed in routine preoperative evaluation. Conscious sedation was used in all cases. Adjustment of medication dosage was performed according to level of consciousness and ventilation rate of the patient.
A standard percutaneous nephrostomy tract was established on the side of the afflicted kidney. The following intervention technique was used to achieve antegrade recanalization of the ureteral lesion. Then, an external-internal ureteral stent was inserted to assure patency.
Technique
The first step was the antegrade insertion of a long vascular sheath (7F diameter) in the ureter to the level of the obstruction to provide support. Bypassing of the ureteral obstruction by a hydrophilic 0.035-inch guidewire and an angled hydrophilic 5F catheter followed.
Precise opacification of the collecting system and the obstructed/injured segment was possible by the infusion of contrast medium through the sheath. The soft tip of the hydrophilic guidewire was pushed through the angled catheter against the site of obstruction with gradually increasing force. During the obstruction negotiation process, the wire should be pushed carefully to avoid penetration of the ureteral wall and the extraluminal route of the wire. When the obstruction was eventually bypassed, the wire was pushed to the bladder and the hydrophilic guidewire was replaced by an Amplatz Superstiff 0.035-inch guidewire. The latter was safely anchored into the bladder. We routinely use lidocaine instillation through the catheter in the bladder in an attempt to minimize patient discomfort from bladder irritation and distension by the guidewire.
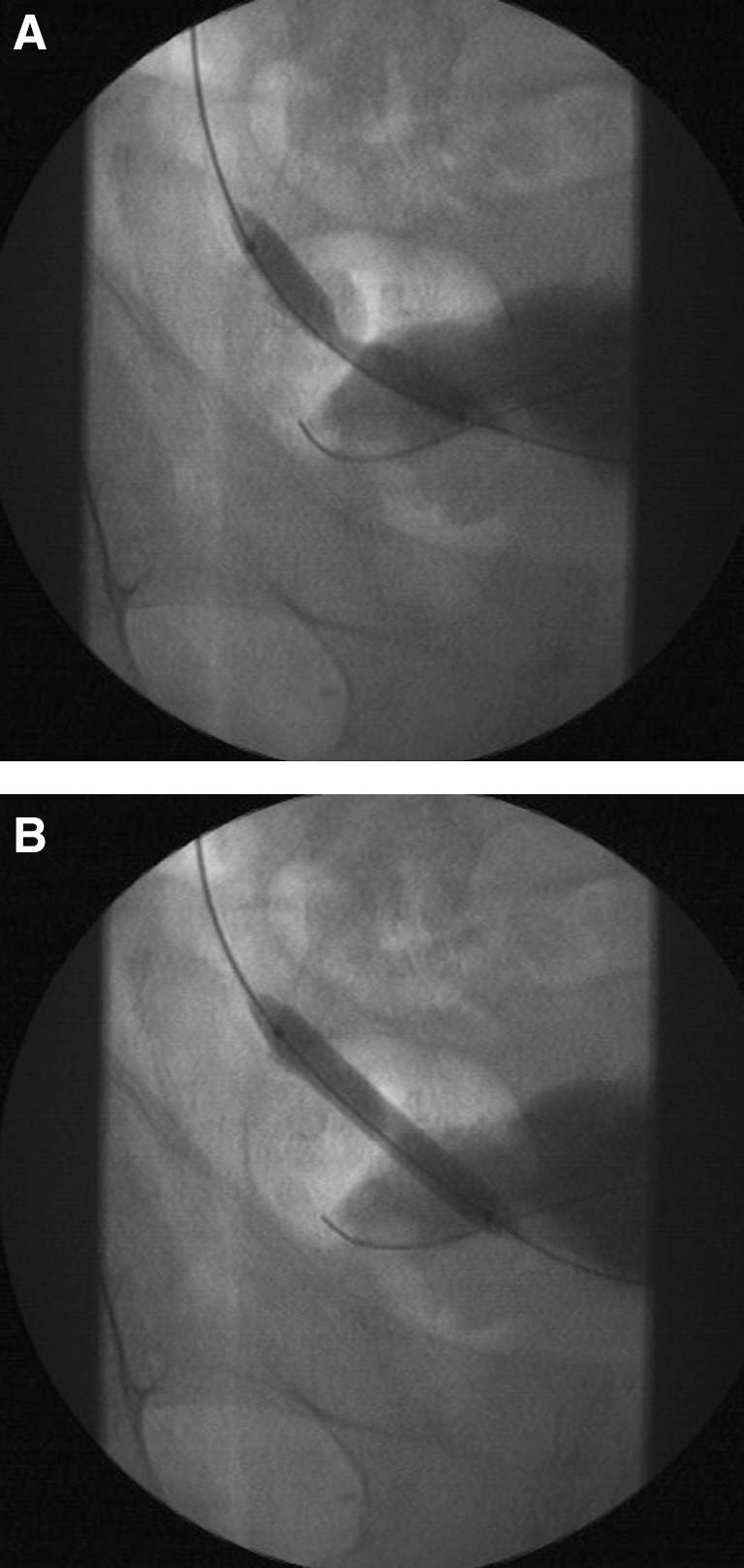
In obstructive injuries, dilation of the obstruction site with a high-pressure angioplasty balloon (approximately 6 mm diameter) follows. A maximum diameter between 5 and 7 mm and inflation to a pressure up to 20 atm was appropriate. The inflation pressure was gradually increased to a level that the “waisting” of the balloon was abolished (Fig. 1). Sutures ligating ureters were eventually fragmented by the high-pressure balloon dilation, and coagulated sites were distended to facilitate stent insertion. Cases of ureteral laceration did not necessitate balloon dilation.
Antegrade nephrostomography was performed for the confirmation of ureteral lumen patency, and the percutaneous insertion of an 8F percutaneous internal/external nephroureteral drainage stent of appropriate length took place. The latter stent is important for short-term patency. Repeated balloon dilations of the obstruction were performed if it was possible to insert the stent through the obstruction site.
Postoperative treatment of the patients included administration of ciprofloxacin 500 mg twice daily. Patients were routinely discharged on the first postoperative day. Clinical examination, blood biochemistry tests, and antegrade nephrostomography with contrast weekly after the procedure were performed until the nephroureteral stent was removed. Ultrasonographic control was performed for patient follow-up after stent removal. The weekly follow-up appointment included the retrieval of the drainage stent and the performance of antegrade nephrostomography, which was performed with the use of a 7F vascular sheath placed by an over-the-wire technique in the renal pelvis after stent removal. In the case of a patent ureter, the nephrostomy was removed, while nonpatent ureters were managed by repeated balloon dilation of the stricture. An internal/external nephroureteral stent was placed again. Successful management was based on the antegrade nephrostomography and ultrasonographic examination. Imaging modalities such as intravenous urography or CT urography were performed in the case of ultrasonographic evidence of hydronephrosis.
Results
Routine blood chemistry examination revealed abnormally increased levels of blood urea and creatinine. Average concentration of urea was 91.1 mg/mL (range 19–130 mg/mL), and average concentration of creatinine was 1.9 mg/mL (range 0.5–3.4 mg/mL). Renal ultrasonography revealed marked dilation of the renal pelvis and upper third of the ureter in 15 cases. Collection of fluid in the retroperitoneal space or in the abdomen or pelvis was observed in 13 cases. It should be noted that both renal dilation and extravasation could be present in the same patient. Intravenous urography or CT urography was used for the exact depiction of the level of ureteral obstruction and for the confirmation of extravasation from the ureteral laceration. Patients with creatinine values >2.5 mg/mL did not undergo any of the contrast-using imaging modalities. Nephrostomography after the establishment of the nephrostomy tract was performed in these patients.
In a total of 25 injured ureters, 12 had interruption of continuity of the lumen, 10 were associated with contrast extravasation, and 3 were related to both. One patient had ureteral lesions bilaterally. Obstruction was observed on the right ureter and extravasation on the left ureter. The level of obstruction or laceration was located on the lower third of the ureter in all cases but two. The latter cases were procedures performed on the upper urinary tract, which included a case of percutaneous nephrolithotomy and a case of pyeloplasty detected after the removal of the Malecot reentry tube and the ureteral stent, respectively. In the injured ureters, the underlying cause was absorbable-suture ligation or accidental coagulation of the ureter in 18 cases, while disruption of the ureter during manipulations was observed in 7 cases, as corroborated by the operating surgeons.
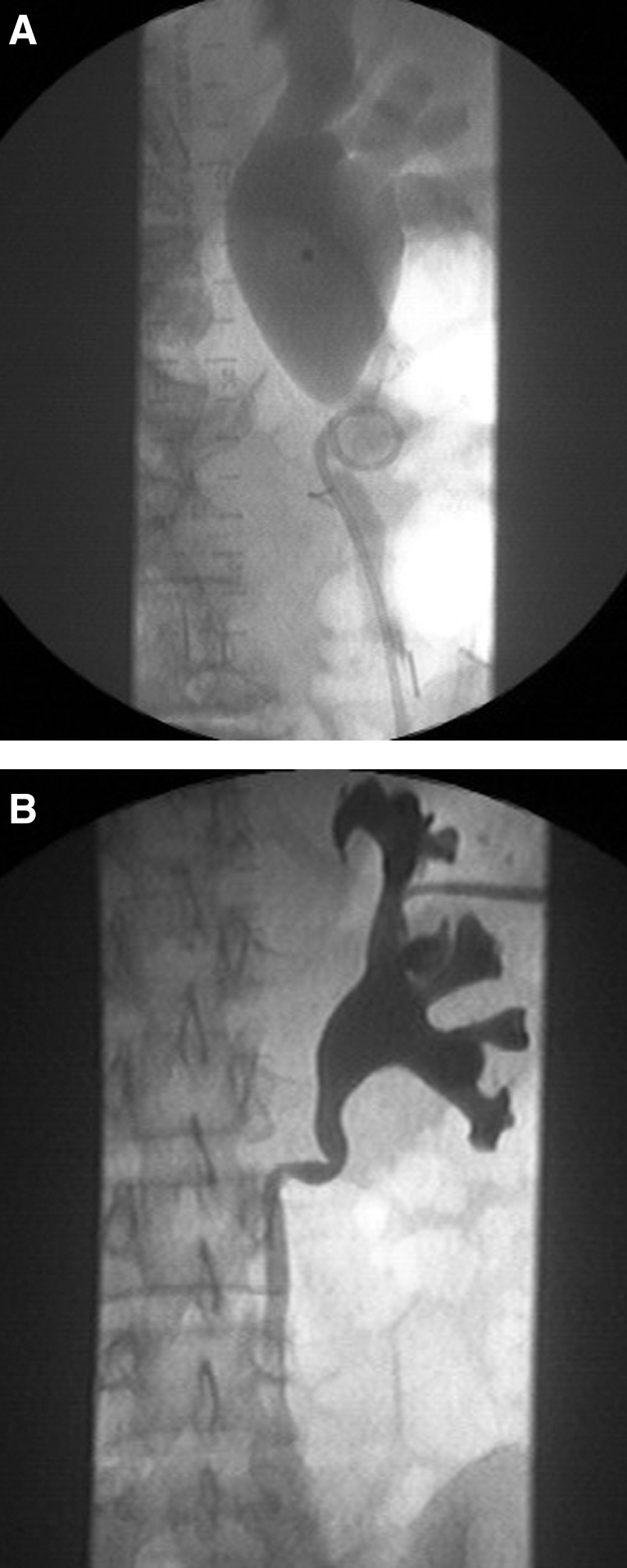
Average stricture length was 1.2 (range 0.5–1.9 cm). Success of the aforementioned technique was possible in 18 ureters. Successful management of the obstructed/lacerated segment took place in one session in 14 ureters (14 patients) (Fig. 2). The latter cases included nine ureteral lacerations and five strictures. Three patients with sepsis were treated by nephrostomy tube for at least a week, and the first session for recanalization of the injured ureter was performed after their overall condition was improved.
Bypass of the obstruction/laceration was not possible in four ureters (four patients) during the first session. In the latter cases, the negotiation of the stricture and recanalization of the ureter was not possible because of suture rigidity or the significantly lacerated ureteral wall. These patients were treated by external drainage for 5 days to 1 week and a second attempt to bypass the stricture according to the aforementioned technique was performed. All four ureters were successfully bypassed after 1 week of external drainage and an additional attempt for recanalization. The technique was not successful in seven cases because the stricture could not be bypassed or the laceration was not successfully repaired. These patients underwent nephrostomy placement as well as open or laparoscopic repair of the lesion. In fact, one patient underwent revision of the pyeloplasty, four patients reimplantation of the ureter, and two cases end-to-end ureteral anastomosis.
Average hospitalization time was 1.8 days, ranging between 0 and 5 days, except for two patients who eventually died. These patients were hospitalized in the intensive care unit for 8 and 30 days, respectively. A patient was discharged on the same day. Follow-up period ranged between 12 and 18 months, with a mean follow-up time of 13.1 months. Ureteral patency was evident at 1 week follow-up in six patients with obstructed ureters. In the remaining patients, balloon dilatation of the stricture was repeated, and a ureteral stent was placed again. Repeated balloon dilation for more than one time took place in two ureters (two patients) because ureteral patency was not achieved (Fig. 3). Extravasation of contrast was observed in two extravasating ureters at the same period. These patients also underwent stricture balloon dilatation and insertion of another ureteral stent. Nephrostomy tubes were removed after a mean indwelling period of 5.9 weeks (range 1–12 weeks).
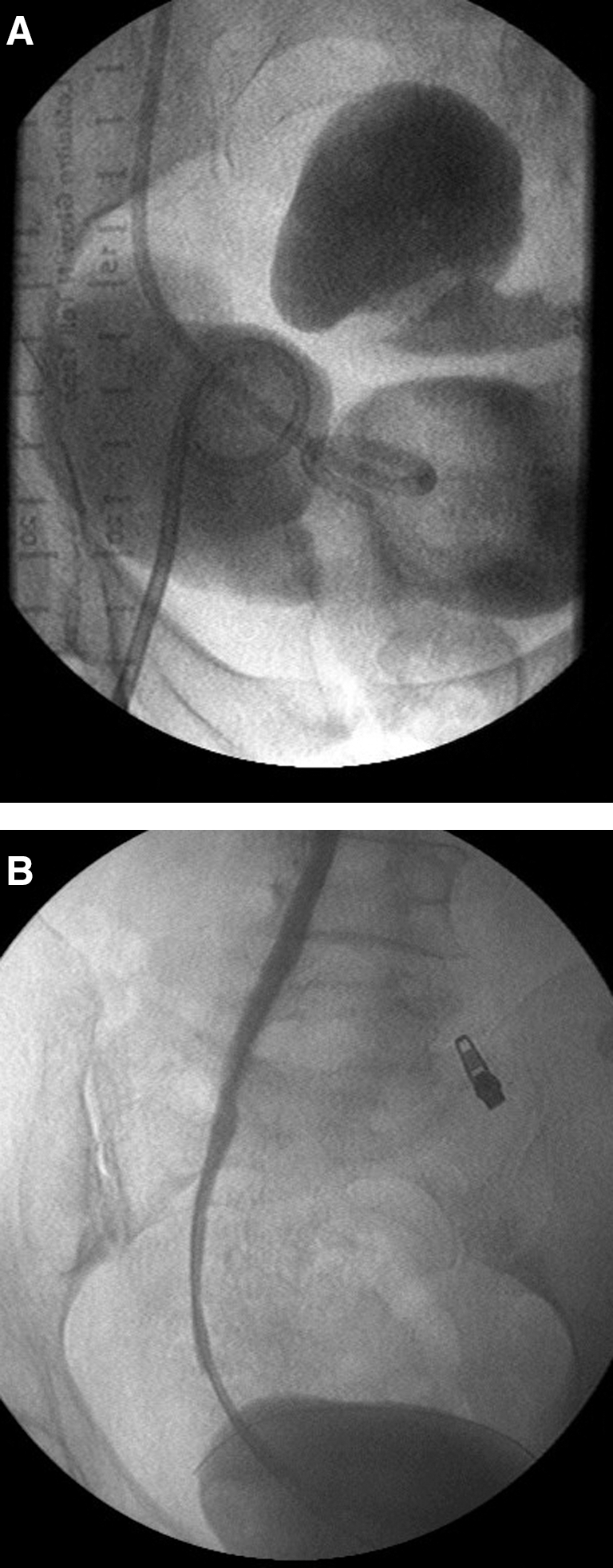
A 65-year-old patient who had multiple ureteral injuries during hysterectomy.
Two patients treated by the aforementioned method died during their hospitalization in the intensive care unit because of sepsis from peritonitis related to colon injury and multiple concomitant injuries. Major complications were not observed in the remaining 22 patients during the follow-up period, which was at least 12 months. Complications such as septicemia, hematuria >1 week, or significant hemorrhage from nephrostomy access or intraureteral manipulations were not encountered except for one case of hemorrhage from the nephrostomy tract several hours after the establishment of the tract. Ultrasonographic examination also revealed perirenal hematoma formation. The bleeding patient was treated conservatively without any sequel.
The most frequent complication encountered was dysuria amd suprapubic discomfort in 12 (54%) patients; these complications were managed by anticholinergic and analgesic medication. In all patients with hydronephrosis from obstructive ureteral injury, blood urea and creatinine values gradually returned to normal levels while renal function was restored. The follow-up period did not reveal compromised renal function (as depicted by the blood biochemistry examinations) while hydronephrosis was not evident on ultrasonography. Additional imaging evaluation took place when deemed necessary. Preoperative data are summarized in Table 2.
ICU = intensive care unit.
Discussion
Iatrogenic ureteral trauma represents the most common cause of ureteral injury. Up to 75% of all ureteral injuries are attributed to surgical manipulations, while only 18% and 7% are associated with blunt or penetrating trauma, respectively. 7,15 Penetrating ureteral injuries have been reported to have a higher incidence in the United States (up to 30%). 7 Intraoperative iatrogenic ureteral injury is encountered in 0.1% to 2.5% of surgical procedures. 3 –6 Gynecologic procedures are related to 73% of all intraoperative ureteral injuries, while general surgery and urology have the latter complication in 14% of their cases. 7 In gynecologic surgery, the highest incidence of ureteral injuries has been reported during total abdominal hysterectomy; intraoperative technical challenges and conditions increase the risk for ureteral trauma. 7,16 Moreover, the development of minimally invasive endoscopic and laparoscopic procedures is associated with higher incidence of ureteral trauma. 5,8,16 The incidence of ureteral trauma is probably higher during the learning curve of the surgeon with a technique.
Regional anatomy knowledge and extensive surgical training are necessary for the performance of procedures in the retroperitoneum, pelvis, and abdomen without ureteral injuries. 17 Moreover, the recognition of the injury during the procedure significantly improves the prognosis and minimizes injury-related morbidity. 3 Ureteral injuries occurring distally and near the bladder could be managed with surgical tension-free nonrefluxing ureter reimplantation. Injuries above the level of the iliac vessel crossing could be treated with an end-to-end ureteroureteral anastomosis. 3,7,17
Ureteral obstruction after gynecologic surgery is most often attributed to suture entrapment of the distal third of the ureter. At the latter, the ureter has a course laterally to the cervix. Ureteral ligature usually presents as costovertebral and abdominal pain secondary to distension of the ipsilateral urinary outflow, whereas bilateral ligation may manifest as anuria, vomiting, elevated urea/creatinine values, and electrolyte disorders. Gynecologists and urologists should bear in mind that ureteral trauma may even be asymptomatic and lead to silent progressive kidney loss. In extreme cases of bilateral ureteral ligation, acute renal failure and even death may ensue. 3,8,18
The management of an unrecognized ureteral injury is more complex and more difficult in comparison with injuries addressed during the procedure. 19 The majority of urologic ureteral injuries have been detected intraoperatively. 8 The currently presented urologic ureteral injuries are associated with minimally invasive approaches, such as ureteroscopy. The latter phenomenon could be attributed to lack of direct visualization of the ureter. Several approaches have been proposed for the management of ureteral injuries.
Open surgery remains the most frequent approach for the repair of ureteral injuries. Nevertheless, perioperative morbidity is still high, and hospitalization is long. 12 –14 The laparoscopic approach has been introduced during the last decade and has proven to be feasible. Currently, laparoscopic experience with the repair of ureteral injuries is limited and needs further clinical investigation. 10 Extensive laparoscopic skill and experience are necessary. 10
Injuries that are associated with sutures accidentally placed on the ureter could be managed by nephrostomy placement and intense follow-up because 80% of these cases are resolved by external urine diversion. 14,20 Accidental ligation of the ureter is the most common injury in gynecologic surgery. The current series presents the results of percutaneous management of cases of iatrogenic ureteral injury that took place during the performance of general surgical, urologic, and gynecologic procedures. Other methods, such as coagulation, are included in the mechanism of injury. Thus, waiting after the establishment of nephrostomy may not be the appropriate management method. In addition, minimally invasive approaches by endoluminal incision with cold knife, laser, electrocautery, Acucise balloon, as well as the ureteroureterostomy by the ureteroscopic approach for the reestablishment of ureteral continuity are related to success rates ranging between 61% and 100%. 13,21,22 The latter results are comparable to those currently presented but remain directly dependent on the length of strictures and patient age while short strictures and delayed treatment represent ideal candidates for endoscopic management. 13,14
We have already presented our experience with the management of gynecologic ureteral injuries with the currently presented method. 14 The current cohort includes ureteral injuries that occurred during several procedures. Thus, the mechanism of injury and the nature of injury differ among the currently presented cases. Gynecologic injuries are usually related to accidental ligation of the ureter while injuries by electrocoagulation and laser coagulation are the second most common mechanisms of injury. Surgical injuries are usually associated with devascularization and adhesion formation, especially in the cases of long strictures. In addition, direct injury of the ureter is also frequent. Urologic ureteral injuries usually occur during ureteroscopies and result in rupture of the ureter or lesion to the urothelium (strictures). 7
The current technique is based on the use of hydrophilic instruments that facilitate the traversal of the majority of strictures in the immediate postoperative period. Balloon dilation was useful for strictures by controlled rupturing of the suture and layer of the ureteral wall (serosal and muscular layers). The consecutive healing of these structures over a ureteral stent results in a larger final lumen. 7 The controlled dilation of the strictures should avoid rupturing the ureter because the extravasation of contrast is a significant etiologic factor for periureteral adhesion formation. 23
The aforementioned technique was also used in cases of ureteral lacerations and ruptured ureteral strictures. The technique was carefully performed in an attempt to avoid further extension of the laceration. Moreover, the extent of the laceration could not be determined before the procedure, and a total laceration of the ureter resulting in two separate ureteral segments cannot always be addressed adequately with the current technique. The cases that failed to be treated by the percutaneous approach could be attributed to the significant diversity of the ureteral injuries included in the current study. The technique provides promising results and reduces patient morbidity by avoiding surgical interventions. Nevertheless, some cases would eventually need further surgical management.
Our previous experience with the management of gynecologic injuries was accompanied by a 100% success rate. Because the latter results were obtained from a selected patient population, the current success rate of 71% could be expected for the inhomogeneous population presented in the study. The current method provides minimally invasive recanalization of the ureter regardless of the type of injury. Moreover, nephrostomy is routinely performed in these patients, and an attempt to recanalize the injured ureter by a minimally invasive approach during a single session is beneficial to the patient.
A traditional concept regarding the time that the repair should be attempted was 3 to 6 months after the injury. During the above period, the regional edema is significantly reduced, and any ligation suture has been absorbed. 3,12 Nevertheless, the delayed management of any ureteral injury represents an issue for the quality of life of the patient, because a nephrostomy tube is necessary to preserve drainage. We observed high effectiveness with immediate percutaneous management and restoration of ureteral continuity in our previous study including gynecologic injuries. 7 In the current study, we expanded the indications for percutaneous management of ureteral injuries in cases that were associated with colorectal and urologic procedures. The immediate management proved to be efficient for the majority of cases. Some cases eventually needed operative repair of the ureter. Nevertheless, operative treatment was avoided in 71% of the cases.
Because the nephrostomy procedure takes place in all cases to preserve the renal function of the injured renal unit, percutaneous treatment provides an invaluable tool to manage ureteral injuries in one session. Moreover, cases that are associated with pelvic inflammation and regional radiotherapy are candidates for the currently presented technique. 12
Although the current method was successfully used in both strictures and lacerations of the ureter, the exact indications remain to be elucidated. Further clinical investigation would provide additional integrity to the currently presented outcome and elucidate the aforementioned issue regarding the technique.
Conclusion
The minimally invasive management of ureteral injuries is a safe and efficient method for both ureteral obstruction and/or laceration in a wide range of iatrogenic ureteral injuries. Further clinical investigation would probably render the percutaneous approach as a first-line treatment modality for ureteral lesions.
Footnotes
Disclosure Statement
No competing financial interests exist.