
Abstract
Background and Purpose:
The AirSeal™ access system is a novel laparoscopic trocar that uses airflow to create insufflation pressure without the need for a physical seal or valve. By eliminating all valve elements within the lumen of the canula, the port provides a platform that accommodates multiple instruments of any diameter, shape, or combination and is ideally suited for laparoendoscopic single-site surgery (LESS). We present our initial experience with valveless trocars in traditional urologic laparoscopic cases and a porcine LESS nephrectomy series.
Materials and Methods:
Nine transperitoneal LESS nephrectomies were performed in a live porcine model using the 27-mm oval valveless trocar. All working instruments were placed through the single port, and the specimen was extracted through the 4-cm port site.
Results:
All cases were completed without technical or operative complications. The porcine single-port nephrectomy (n = 9) was successfully performed in a mean operative time of 24 minutes through the single 27-mm oval trocar. This accommodated a 5-mm laparoscope, multiple 5-mm instruments, the Endo GIA stapler, and the 15-mm Endocatch bag without loss of insufflation pressure. Condensation and smudging of the laparoscope were minimized, improving visualization and efficiency. The system allowed for use of suction without significant loss of insufflation pressure.
Conclusion:
The initial experience with the AirSeal valveless trocar system in LESS is encouraging. This technology may offer significant benefits over traditional laparoscopic trocars and single -port platforms and appears particularly suited to facilitate LESS.
Introduction
The AirSeal™ system (Surgiquest, Orange, CT) is a novel technology that combines advances in port design and insufflation. Current trocars use a one-way gasket to form a seal around the laparoscopic instrument or camera. The AirSeal trocar uses a valveless design, generating an insufflation pressure that uses airflow to create an air curtain (Fig. 1).

The elimination of the valve elements within the lumen of the trocar offers several potential advantages. 3,4 First, insufflation is obtained using a recirculating closed airflow system. This system monitors the insufflation pressure in real time, rapidly adapting to fluctuations in pressure. Consequently, there is minimal loss of insufflation pressure when changing instruments or when using suction within the surgical field. The recirculating airflow also automatically evacuates and filters any smoke generated within the field. Second, the lack of a physical barrier within the trocar eliminates the smudging and condensation that can occur when passing a laparoscope through a traditional port. This reduces the time needed to attend to the camera. Third, the lack of a physical seal mechanism also eliminates drag on laparoscopic instruments, reducing instrument wear and improving instrument freedom of movement. Tissue specimens and needles are also more easily retrieved because there is no physical barrier to be traversed. Finally, the valveless trocar also provides the freedom to insert multiple and irregularly shaped instruments through the same trocar without losing insufflation pressure (Fig. 2). This unlimited flexibility in instrumentation is ideally suited for LESS.

View through a 27-mm oval valveless trocar with a 5-mm laparoscope illuminating the fully insufflated abdomen and peritoneal contents.
In this report, we tested the AirSeal system using a prototype 27-mm elliptical trocar to perform the first series of true single-port, single-lumen LESS nephrectomies in a porcine model.
Materials and Methods
True single-port, single-lumen LESS porcine nephrectomy model
Approval was obtained from the UCLA Animal Research Committee. Five 1-year-old female Yorkshire pigs weighing 50 kg were used in this study to perform single-port, single-lumen nephrectomies in nine renal units. The animals were anesthetized, maintained on ventilatory support, and monitored by veterinary staff. The animals were positioned in a modified flank position. A 4-cm skin incision was made along the lateral border of the rectus line, the fascia was exposed, and the peritoneum was entered. The 27-mm oval trocar was inserted using a Hassan technique and attached to the Surgiquest insufflator to establish a pneumoperitoneum of 15 mm Hg (Fig. 3).
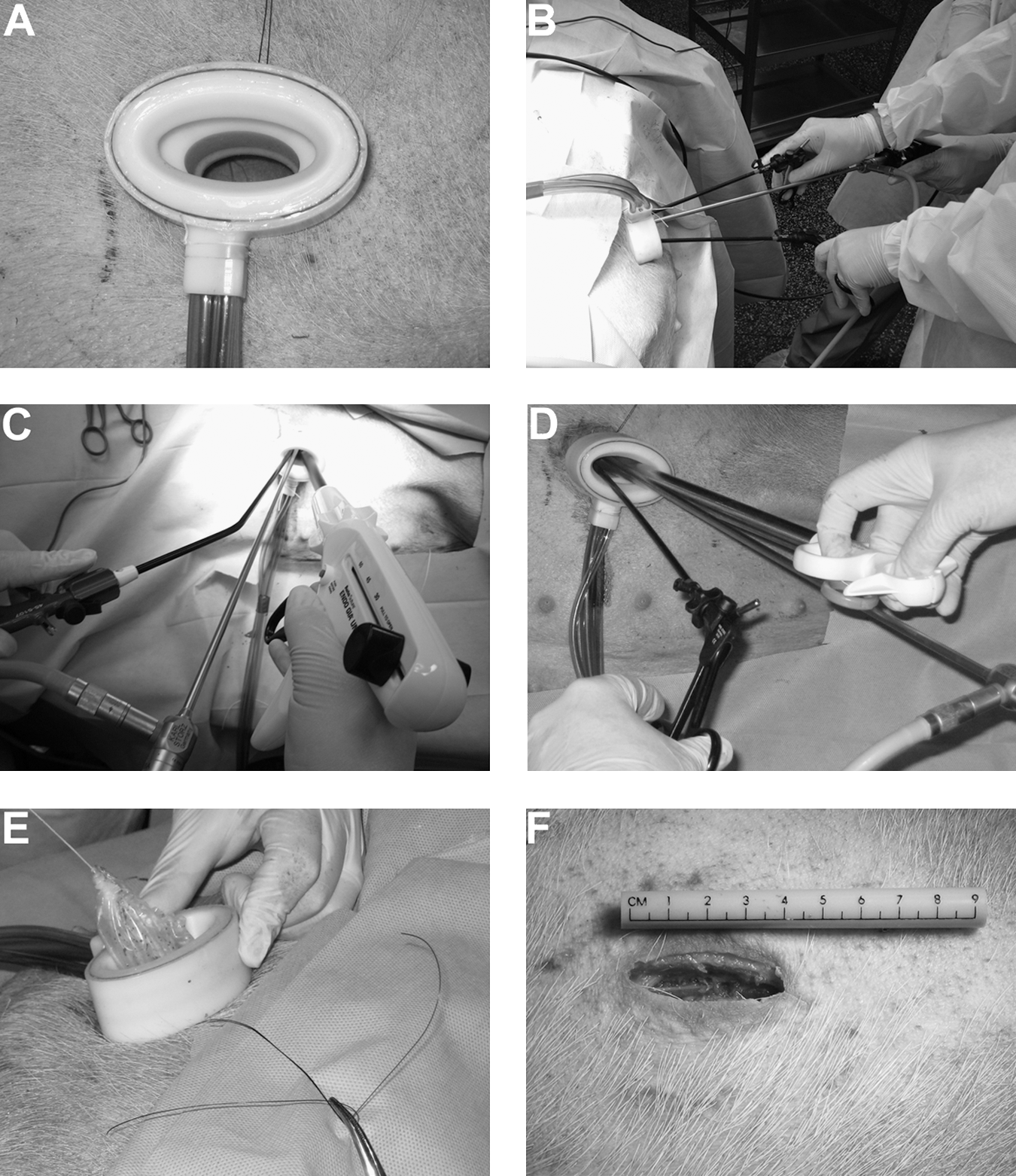
Images highlighting the valveless trocar in a laparoendoscopic single-site porcine nephrectomy.
Standard and bariatric extended-length 5-mm 30-degree laparoscopes (Karl Storz, Tuttlingen, Germany) were used through the port. Combinations of two and three 5-mm instruments were placed to perform the dissection. These included standard laparoscopic scissors, bowel graspers, Maryland and right-angle forceps. The renal hilum was secured en bloc with the use of a 12-mm endovascular stapler. The kidney was placed in a 15-mm Endocatch specimen retrieval bag and extracted through the port site incision. The port site was then closed with a running 0-polyglactin suture, and the skin was reapproximated with staples. The animal was then repositioned to perform the contralateral nephrectomy in an analogous fashion. The animal was sacrificed at the completion of the procedure.
Results
Porcine AirSeal LESS nephrectomy model
A total of nine porcine transperitoneal LESS nephrectomies were performed in five animals. All surgeries were completed without complication and with minimal blood loss. Mean operative time was 24 ± 13 minutes with a trend toward even shorter operative times at the end of the series. Blood loss was minimal in each case. After specimen extraction, the port incision measured 4.5 ± 0.5 cm. No additional ports or needlescopic instruments were used.
Discussion
LESS
This project has several important findings. First, we found the AirSeal valveless trocar system to be suited to LESS, because it provides tremendous flexibility in the placement of multiple instruments of different sizes and shapes. LESS has evolved from the placement of multiple standard laparoscopic ports through a single umbilical skin incision 5 to the placement of specifically designed multichannel ports through a single incision. The R-port™ and TriPort™ (Advanced Surgical Concepts, Bray, Ireland) house one 12-mm and two 5-mm ports in a single casing and have been used to perform LESS nephrectomy, donor nephrectomy, ureterolithotomy, orchidopexy, and pyeloplasty procedures. 2,6,7 The Uni-X™ (Pnavel Systems, Morganville, NJ) has three 5-mm channels and has been used to perform renal cryotherapy, nephrectomy, abdominal sacrocolpopexy, and radical prostatectomy. 8,9 Other approaches have included the passing of standard laparoscopic and robotic ports through a Gelport™ (Applied Medical, Rancho Santa Margarita, CA) placed through a single incision to perform renal surgery. 10 Kaouk and colleagues 11 have reported performing LESS using the da Vinci S robot through the R-port supplemented with an additional 8-mm trocar placed through the same skin incision.
The AirSeal system has several advantages over these single-port designs. Traditional and multichannel ports limit the number and size of instruments that can be passed. These cases potentially necessitate the placement of additional ports to accommodate endovascular staplers, specimen bags, and other instruments larger than 10-mm. By having a true single-port design, any combination of instruments can be used. In this report, the 27-mm AirSeal port simultaneously accommodated a 5-mm laparoscope, two 5-mm instruments, and an endovascular stapler through a single 4-cm incision. The multichannel port designs also dictate the relative position of each instrument. The AirSeal allows for more flexibility in instrument placement, and the elliptical shape does provide for some subtle triangulation of the working instruments. As new instruments are developed to address the space constraints specific to LESS, the AirSeal system also provides the advantage of accepting instruments that are curved or irregularly shaped while maintaining the benefits of an insufflated surgical field.
The flexibility of the valveless trocar system does present some challenges in LESS. First, laparoscopic surgeons are accustomed to the laparoscopic instrument resting on the gasket within the trocar. This stabilizes the instrument and creates a fulcrum point that the surgeon can use when maneuvering the instrument. The lack of physical elements within the trocar to stabilize a laparoscopic instrument creates a new working environment and different working feel when using the valveless trocar. We found it best to rest the laparoscopic instruments against either the inner or outer edge of the trocar for stabilization. We also found it easier to operate with the surgeon sitting as an additional means of stabilizing the laparoscopic instruments.
Having a true single-port design without internal structures also affects the placement and relative positioning of the camera and working instruments. We found the bariatric length 5-mm 30-degree laparoscope allowed for the camera head to be positioned away from the working instruments. We primarily oriented the laparoscope to be looking down on the operative field. This orientation is similar to our approach in traditional multiple-port laparoscopy and created a familiar perspective. Using an angled laparoscope also dropped the camera head below the working envelope of laparoscopic instruments, further reducing interference between the instruments and camera. Flexible laparoscopes would likely provide similar benefits.
Our group also experimented with straight and curved laparoscopic instrumentation while using the valveless trocar to improve instrument triangulation and minimize “jousting” interactions between the instruments. Our group identified the most comfortable instrument combination as a straight laparoscopic instrument in the nondominant and a curved instrument in the dominant hand. The complexity of operating two curved instruments appeared to be magnified by the lack of the stabilization provided by the gasket found in traditional trocars. We did find that one curved instrument was enough to provided working space for each hand.
Over the series of nine nephrectomy procedures, the surgical team quickly adjusted to operating through a valveless trocar. Additional experience with the AirSeal platform would document surgeon comfort level with this novel trocar design and other opportunities to realize the benefits of the valveless design.
Valveless trocar design
The second important finding from this study highlights the potential benefits of the AirSeal trocar technology. A significant portion of any laparoscopic surgery is spent cleaning the laparoscope and evacuating smoke created by electrosurgical devices. In our early experience, we found that the valveless trocar system eliminated the smudging encountered when inserting the laparoscope through the gasket in a traditional laparoscopic port. This minimized the time needed to clean the camera throughout the case. Image quality was also improved by the continuous evacuation and filtering of the smoke from the operative field. Finally, the recirculating airflow system is able to maintain a consistent pneumoperitoneum even when suction is used in the field. We found that even when suction was constantly used, the pneumoperiteum remained greater than 11 mm Hg. Pressure was also maintained even when the tether of the specimen bag was placed through the trocar. Herati and associates 3 reported their early results using the Food and Drug Administration approved 12-mm round trocar in multiple-port laparoscopic renal surgery and also identified similar benefits of the AirSeal system. 3 In addition, this group suggested that the recirculating system resulted in a reduction in the volume of CO2 used, which may, in a high-volume center, result in demonstrable cost savings. 3
The AirSeal system does have limitations. First, a significant drawback of the current version of the recirculating airflow system is the noise generated by the compressor. Future generations of the system would benefit from reduction of the noise generated by the system itself. Second, there is a cost associated with adoption of a new trocar technology because it would necessitate the purchase of a new insufflator system in addition to the cost of the disposable trocars and tubing. Perhaps most importantly, the physiologic effects of a recirculating insufflation system are not fully known. Preliminary studies do not show any ill effects, such as increased tissue absorption of CO2, or differences in CO2 elimination rates. 3,4 Herati and colleagues 3 also note that the AirSeal system does maintain a more constant insufflation pressure. The summation of this pressure over time may accentuate the physiologic effects of the pneumoperitoneum, although this has not yet been formally examined.
Conclusion
The initial experience with the AirSeal valveless trocar system in LESS is encouraging. This technology may offer several potential benefits over traditional single-port platforms, including reduction in the time attending to the laparoscope, automatic smoke evacuation, stable insufflation pressures, ease of needle and specimen passage through the trocar, and the increased flexibility in accommodating multiple instruments through a single port. Further development and study of these trocars will help define the optimal size and shape of valveless trocars for various applications and may lead to advances in traditional laparoscopic and robotic approaches, as well as the urologic applications of LESS.
Footnotes
Disclosure Statement
Dr. Schulam is a member of the scientific advisory board for Surgiquest and has been compensated with stock options. No competing financial interests exist for the other authors.