
Abstract
Introduction and Objectives:
Retroperitonoscopic nephrectomy in children was considered by some authors to be the final gold standard in children. Hence, we reviewed our data focusing on the safety and efficacy of the procedure.
Materials and Methods:
In the period from November 2005 till February 2010, 35 patients were operated by a single surgeon (the first author); patients comprised 18 boys and 17 girls, with a mean age of 7.5 years (range: 1–19 years). In all patients, the retroperitonoscopic approach was used with the use of only three trocars, one 10-mm optic trocar and two 5-mm trocars. The retroperitoneal space was established either by direct insufflation into the Gerota fascia, which is grasped and opened under vision, or using a balloon dilator to widen the space and then incising the Gerota fascia under control of the optic trocar, then control of the pedicle is performed, and the specimen is extracted from the same optic trocar.
Results:
The mean operative time is 75 minutes (range: 45–120 minutes). Nineteen nephrectomies and 16 nephrouretrectomies were performed. Blood loss was minimal, blood transfusion was not given, and conversion to open surgery was not needed. There were no intraoperative complications, and only one postoperative hematoma resolved spontaneously. The mean hospital stay was 2 days (1–3 days).
Conclusion:
Retroperitonoscopic nephrectomy in children is safe and feasible. Blood loss is minimal, hospital stay is very short, and complications are minimal. It has excellent cosmetic outcome.
Introduction
Laparoscopic nephrectomy through the transperitoneal approach is a settled, minimally invasive technique for nephrectomy in children. Retroperitonoscopic approach is not gaining the same popularity as the transperitoneal approach and its use was described by limited centers. Those in favor of transperitoneal approach are concerned by the working space in the retroperitonoscopic approach, which in their opinion is rather limited.
On the other hand, those in favor of retroperitonoscopic approach consider it as the natural approach to the kidney and ureter simulating the open surgical approach to the kidney, and they report no difficulty related to a limited working space and consider this approach as the gold standard approach for laparoscopic nephrectomy and a forward way in the progress of laparoscopic renal surgery in children. 3,4
Herein, we report our single-center experience with retroperitonoscopic nephrectomy and nephrouretrectomy in children, emphasizing the role of the learning curve and highlighting the safety and feasibility of the technique in the different indications beside giving tips and tricks of the trade that help to establish a rapid and safe learning curve.
Patients and Methods
In the period from November 2005 to February 2010, we operated on 35 children and adolescent, 18 boys and 17 girls, with a mean age of 7.5 years (1–19 years).
For all patients, the lateral retroperitonoscopic approach was used as follows: general anesthesia was used in all patients. Nasogastric tube was inserted for all patients, together with a urethral catheter. All patients were positioned in the lateral jackknife kidney position. Access to the retroperitoneal space was achieved by a 1-cm incision below the last rib in the midaxillary line, and through this incision, a blunt scissor was used to pierce the lumbar fascia and then, using long slim retractors, we could observe the Gerota fascia, which is grasped by a forceps and opened by a scissor. In the opened Gerota fascia, we introduce the first optic trocar, which is always a 10-mm trocar, and insufflation is started inside the Gerota fascia. In small hypoplastic kidneys, we access the retroperitoneal space in the same manner, but we do not search for the Gerota fascia, instead we use a balloon dilator to develop the retroperitoneal space and then we insert the first trocar and identify the Gerota fascia under vision.
We usually work through three trocars: the optic trocar and two 5-mm trocars. The second trocar is inserted in the costovertebral angle and followed by the third trocar in the anterior axillary line above the iliac crest by one finger breadth.
After all trocars were in place, we always start by attacking the renal pedicle first. One hand usually acting as a lever just elevating the kidney upward, while the other hand dissecting the fascia over the renal pedicle, we first face the renal artery, which is controlled and severed, and then the renal vein, which is also controlled and severed. In case of small hypoplastic kidneys, we first identify the ureter at the border of the psoas muscle and dissect it upward toward the renal pedicle, which is ultimately identified easily and then controlled and severed in the same manner.
Control of the renal pedicle was done routinely using 5-mm clip applier in 29 cases. Other ways of pedicle control were ligasure vessel sealing device in two cases, harmonic scalpel in one case, and not tying in three cases.
After complete pedicel control, dissection of the upper renal pole is followed by dissection of the anterior surface of the kidney from the peritoneum, and finally, the kidney remains attached only to the ureter, which is dissected and controlled.
Control of the ureter depends on the original pathology; in case of vesicoureteral reflux, we control the ureter as low as we could by clips and then severe it. In the absence of reflux, we control the ureter at the lower pole of the kidney by either using clips, ligasure, or harmonic scalpel or, rarely, tying a ligature and then the ureter is severed.
Extraction of the kidney is performed through the 10-mm optic trocar (Figs. 1 and 2). The kidney is grasped by a grasper through the optic trocar after putting another 5-mm camera in the costovertebral angle trocar to ensure adequate view of the kidney. Usually, we grasp the kidney from one pole to facilitate its extraction along its longitudinal access. A drain is left in all patients in the retroperitoneal space through the costovertebral angle trocar for 24 hours only (Fig. 3). All trocars sites are infiltrated with local anesthetic before closure is completed.

Retroperitonoscopic nephrectomy of a hypoplastic kidney.
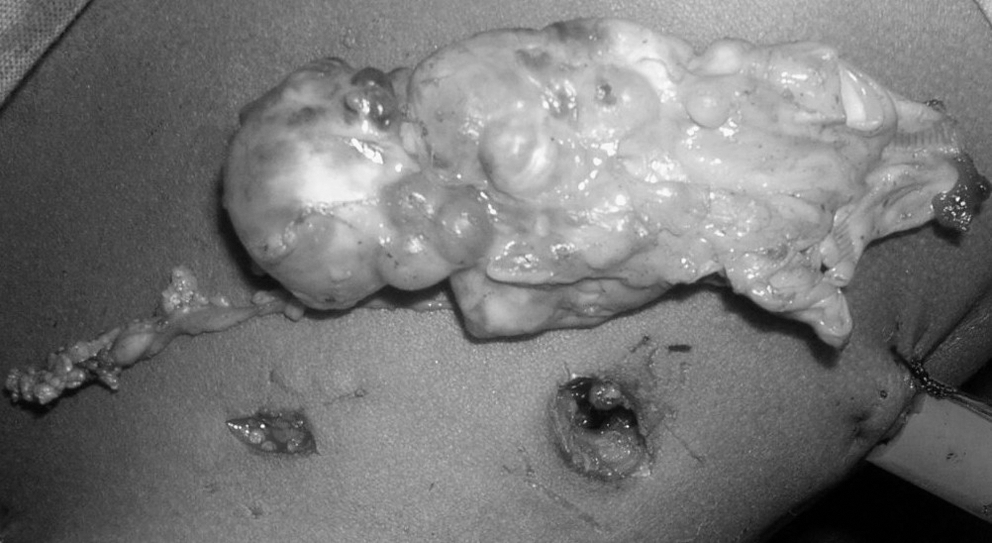
Retroperitonoscopic nephrectomy of a multicystic dysplastic kidney.

Postoperative closure of trocar sites with the drain in place.
Results
As shown in Table 1, we operated on 35 patients. In all patients, the lateral retroperitoneal approach was used successfully. Nineteen nephrectomies and 16 nephrouretrectomies were performed, 19 right side and 16 left side. Nephrectomy and nephrouretrectomy were indicated for nonfunctioning kidneys with vesicoureteral reflux in 15 patients, neglected hydronephrosis in 9 patients, multicystic dysplastic kidney in 7 patients, and miscellaneous indications in only 4 cases, including 2 hypoplastic kidneys associated with hypertension and 2 renal stone diseases, of which one was a xanthogranulomatous kidney. The average operative time was 75 minutes; 28 children had an operative time of 80 minutes and less, whereas only 7 children had >80 minutes. The evolution of operative time with increasing experience is demonstrated in Figure 4. Blood loss was <50 mL in 32 patients and never exceeded 100 mL in the remaining 3 patients; no single patient needed any blood transfusion. Hospital stay ranged from 1 to 3 days, with a mean hospital stay of 2 days; analgesic requirement was only during the first postoperative day in all patients, with no need for opiate analgesics. Conversion to open surgery was not needed. Intraoperative complications were not encountered. Postoperative hematoma was encountered in one adolescent, which was caused by bleeding from the trocar site that was inappropriately closed; conservative treatment with antibiotics and follow-up were successful.
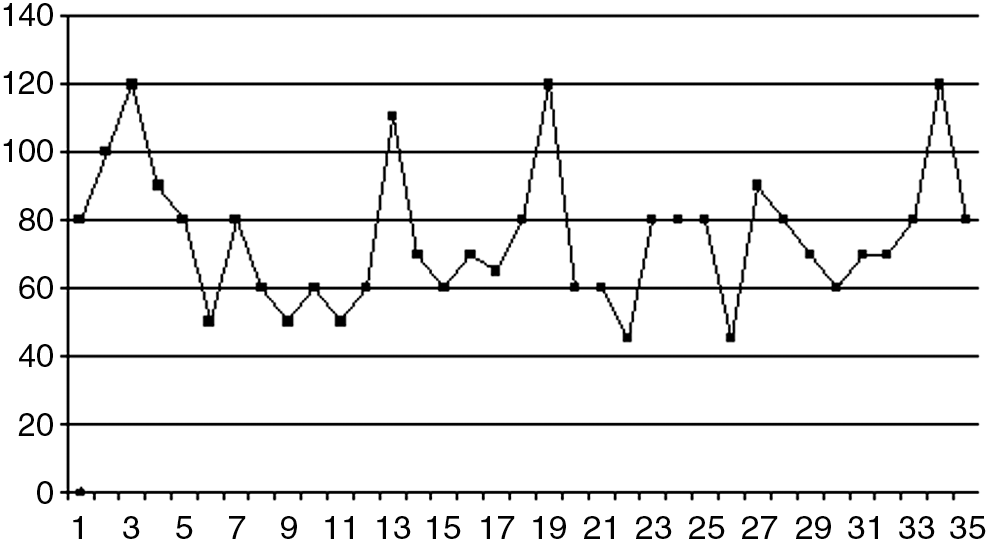
Evolution of the operative time with increasing experience.
RT = right; LT = left.
Discussion
Retroperitonoscopic approach receives a lot of criticism. Limited working space is the main disadvantage described by opponents of the approach, especially in children. Opponents of the approach are in favor of the transperitoneal approach, which in their opinion is rather a wide working space making laparoscopic surgery easy and rapid.
Herein, we presented our experience with the use of the lateral retroperitonoscopic approach for nephrectomy and nephrouretrectomy in children and adolescents. All cases are operated by a single surgeon who is the first author in the present study. Camera men were the second and third authors of the present study.
According to our experience, the retroperitonoscopic approach was feasible even in very young children aged 1 year, which is the lowest age in our series with no difficulty related to the working space; also, the working space was very adequate for completing the nephrectomy in a reasonable time with no limitation. Our experience coincides with other authors who reported neither difficulty nor increased incidence of complications in doing retroperitonoscopic nephrectomy and partial nephrectomy in children weighing <10 kg. 3,5 This reflects the importance of concentrating on a single approach—either the retroperitonoscopic or transperitonoscopic approach during the learning curve.
The retroperitonoscopic approach is considered a duplication of open surgical approach to which all pediatric urologists and urologists are familiar. It avoids violation of the peritoneum and dissection of the colon and obviates unnecessary intraperitoneal manipulations, which might be associated with increased incidence of complications and postoperative ileus. This is reflected in the operative time. In our series, the mean operative time was only 75 minutes, which is very close to our mean operative time during open nephrectomy and coincides with the operative time of most of the studies addressing retroperitonoscopic nephrectomy. Moreover, this mean operative time is shorter than the operative time of transperitoneal laparoscopic nephrectomy. 4 It has to be emphasized that the operative time during retroperitonoscopic nephrectomy decreases with experience. As shown in Figure 4, we can clearly find that only seven patients had operative times of >80 minutes; three of them were in the start of the learning curve and the other four were difficult cases including one case of xanthogranulomatous kidney, one associated with longstanding perinephritis due to a longstanding renal stone disease, and the remaining two cases were hypoplastic kidneys.
Retroperitonoscopic approach gives direct access to the kidney, making the renal pedicle easy to identify and control with no difficulty. Access of the renal artery is achieved first by this approach, which is a major advantage of the technique during nephrectomy. Control of the renal pedicle in our series was conducted using clip appliers in most of the cases or using harmonic scalpel, ligasure, and not tying in the remaining cases. Actually, based on our experience, clip application is the easiest and fastest way of control of the renal pedicle being also very safe; however, use of harmonic scalpel and ligasure is also effective, simple, and rapid but sometimes dangerous in larger vessels and more costly. Not tying is time consuming; however, it is effective but requires special laparoscopic skills.
Retroperitonoscopic approach is suitable to all indications of nephrectomy and nephrouretrectomy in children, including neglected hydronephrosis due to pelviureteral junction obstruction and obstructed megaureter. Huge hydronephrotic kidneys are not a contraindication to retroperitonoscopic nephrectomy, wherein puncture of the hydronephrotic kidney leads to shrinkage in the size of the kidney, making it very amenable to extraction through the optic trocar with no need to increase the size of the port. Hemal et al 6 presented their experience in laparoscopic nephrectomy for giant hydronephrosis using both transperitoneal approach and retroperitoneal approach, concluding that the retroperitoneal approach is a feasible alternative even with the narrow retroperitoneal space due to huge kidney. Multicystic dysplastic kidneys pose no surgical difficulty during retroperitonoscopic approach. Hypoplastic kidney in our series was managed cautiously during retroperitonoscopic approach. First, during the access we do not grasp the Gerota fascia; instead, we insert a balloon dilator and dissect the retroperitoneal space and then insufflation is started followed by identification of the ureter, which guides us to the kidney. This way helps us not to open the peritoneum inadvertently by mistake between it and the Gerota fascia, which is more difficult to identify in small hypoplastic kidneys. Second, we do not try to approach the vessels first in the hypoplastic kidneys instead; we approach the ureter first, which makes identification of the pedicle more safe and easy. Xanthogranulomatous kidneys were treated by laparoscopic approach safely. 7,8 In our series, we operated on only one xanthogranulomatous kidney; as it was very difficult to dissect the fat overlying the renal pedicle and to identify the pedicle safely, it was performed with the aid of the ligasure vessel sealing device, which helped us to safely control the renal pedicle with the fat around. Dissection of the kidney from the peritoneum was rather difficult and subcapsular dissection was used in some parts to prevent inadvertent injury to peritoneum and peritoneal structures. 7
In our series, the lateral retroperitonoscopic approach was adopted in whole cases. The advantage of the lateral retroperitoneal approach over the prone retroperitoneal approach is that it gives an access to the ureter at a lower level than in the prone position, making nephrouretrectomy more efficient and leaving a shorter ureteral stump. Moreover, the lateral approach is quite similar to the open approach in surgical landmarks rather than in the prone position, which is more similar to the relatively less frequently used lumbotomy approach. Comparative study between the lateral and prone approaches in partial nephrectomy proved no difference except for the accessibility of the lower ureter as previously explained. 9
The fate of the stump left following nephrectomy and partial uretrectomy is a matter of concern and debate. Cain et al 10 presented their retrospective review of a cohort of patients who underwent nephrectomy and partial ureterectomy and thereby had a refluxing stump. They found that only 5% of their patients developed recurrent symptomatic urinary tract infection necessitating secondary uretrectomy; these patients had risk factors contributing to the infection, namely posterior urethral valve, uretrocele, neurogenic bladder, and female sex. They concluded that complete uretrectomy with nephrectomy is not routinely indicated and can be spared to symptomatic children. On the other hand, Casale et al 11 presented a retrospective review of a cohort of children who underwent nephrectomy and partial uretrectomy and thereby a refluxing stump; they found that 19% had recurrent urinary tract infection necessitating secondary uretrectomy. All of them were girls. They advised complete uretrectomy with nephrectomy. With regard to leaving a ureteral stump, we found that the transperitoneal laparoscopic nephrectomy would be the best option if complete uretrectomy has to be contemplated followed by lateral retroperitonoscopic approach and finally the prone approach, which gives no downward space to remove a large ureteral segment, and so we preferred the lateral over the prone approach in our series.
Comparative studies between laparoscopic nephrectomy and open nephrectomy in children are scarce and almost all of them are retrospectives ones; however, superiority of retroperitonoscopy over open surgery in terms of the need for analgesics, shorter hospital stay, blood loss, and cosmoses was proved in a recent retrospective study published in 2010 that compared retroperitonoscopic prone nephrectomy and open nephrectomy. This study proved that retroperitonoscopic prone nephrectomy is superior in terms of analgesic need and reduction of hospital stay significantly. 12
Our study proves a reduction in the mean hospital stay to only 2 days, reflecting the rapid recovery and decrease in the need for postoperative analgesia, with rapid recovery of bowel movement associated with the use of the retroperitoneal approach. El-Ghoneimi et al 3 and Tadini et al 5 reported the same mean hospital stay of about 2 days for retroperitonoscopic nephrectomy in children. Absence of any intraoperative complications, minimal blood loss, and absence of any conversion to open surgery prove the fact that the technique is easy, safe, effective, and feasible to learn, with no complications. The only complication in our series was very mild, which occurred in an obese adolescent in the form of postoperative hematoma from bleeding in the wall of one of the trocar sites and disappeared spontaneously with no need for intervention.
Conclusion
Retroperitonoscopic approach is the direct approach to the kidney for nephrectomy. It is a safe, feasible, easy-to-learn approach characterized by short hospital stay, minimal blood loss, absence of intraoperative complications, and excellent cosmoses.
Footnotes
Disclosure Statement
The authors certify that there was no financial support to this work from any organization and no conflict of interest of any kind.