
Abstract
Objective:
Enterocystoplasty is an established treatment for patients with refractory neurogenic bladder symptoms. We assessed the feasibility, safety, and efficacy of a robot-assisted enterocystoplasty in this population.
Materials and Methods:
Five neurogenic bladder patients, median age of 43.8 years, underwent the procedure. Using a five-port technique, intraperitoneal robotic enterocystoplasty was performed through the following steps: (1) creation of a U-shaped full-thickness detrusor cystotomy, (2) intracorporeal harvesting of 30 cm of ileum, (3) intracorporeal construction of a detubularized ileal patch, and (4) anastomosis of the ileal patch to the cystotomy. An extracorporeal side-to-side bowel anastomosis re-established bowel continuity. After surgery, urinary continence, bladder capacity, upper tract protection, and complications were assessed.
Results:
Mean operative time was 6.4 hours, estimated blood loss was 180 mL, and length of stay was 7 days. Postoperatively, all patients had a functioning enterocystoplasty, urethral continence, and normal upper tract imaging. One patient was rehospitalized for an ileus/urinoma, which resolved with conservative treatment.
Conclusions:
Robot-assisted enterocystoplasty can be effectively and safely performed with minimal morbidity.
Introduction
Robot-assisted minimally invasive surgery, with its greater degree of instrument freedom, may offer suturing advantages during the enterocystoplasty procedure. Recently, a case report on robot-assisted enterocystoplasty was published, 7 but this modality has not been explored in a larger patient series. Our goal was to describe a robot-assisted enterocystoplasty technique in a consecutive patient cohort and report on the initial safety and efficacy outcomes.
Materials and Methods
Patients/outcome measures
Patients were identified through an Institutional Review Board–approved retrospective review of surgical logs. Chart review was performed to extract demographic, urodynamic, operative, and postoperative data. All patients treated with robotic enterocystoplasty had an established neurogenic bladder diagnosis and had failed conservative therapies for urinary incontinence and low bladder compliance. All patients treated with robotic enterocystoplasty underwent full informed consent and were initially offered an open enterocystoplasty as an alternative.
Robotic enterocystoplasty procedural safety was assessed through review of intraoperative blood loss and intraoperative/postoperative complications. Efficacy was assessed through review of length of hospital stay, postoperative bladder capacity, urinary continence, and upper tract status. The total inpatient direct costs for procedure and the postoperative hospital stay were also calculated for each patient.
Surgical technique
The robotic enterocystoplasty surgical technique was modeled after the open technique popularized by Leng et al. 8 All patients received broad-spectrum antibiotics prior to general anesthesia and were placed in the supine position with the legs abducted and the arms tucked. An 18F catheter was placed per urethra. After pneumoperitoneum was established, five trocars were placed for access, including a supraumbilical 12-mm camera trocar. Figure 1 summarizes the trocar schematic used for the procedure.

Trocar placement for robot-assisted enterocystoplasty.
After the bladder was filled to capacity with sterile water via the urethral catheter, the dome of the bladder was sutured to the anterior abdominal wall. The peritoneum was sharply dissected off the posterior bladder wall using endowrist hot shears (Intuitive Surgical, Sunnyvale, CA) and a 15 × 10 cm full-thickness U-shaped detrusor cystotomy was developed. The cystotomy was opened to its maximal aperture by grasping the U-shaped detrusor flap with endowrist prograsp forceps (Intuitive Surgical) and elevating toward the abdominal wall (Fig. 2). The cystotomy was made as large as possible, depending on bladder capacity. During cystotomy development, the urethral catheter remained clamped to ensure good pneumoperitoneum.
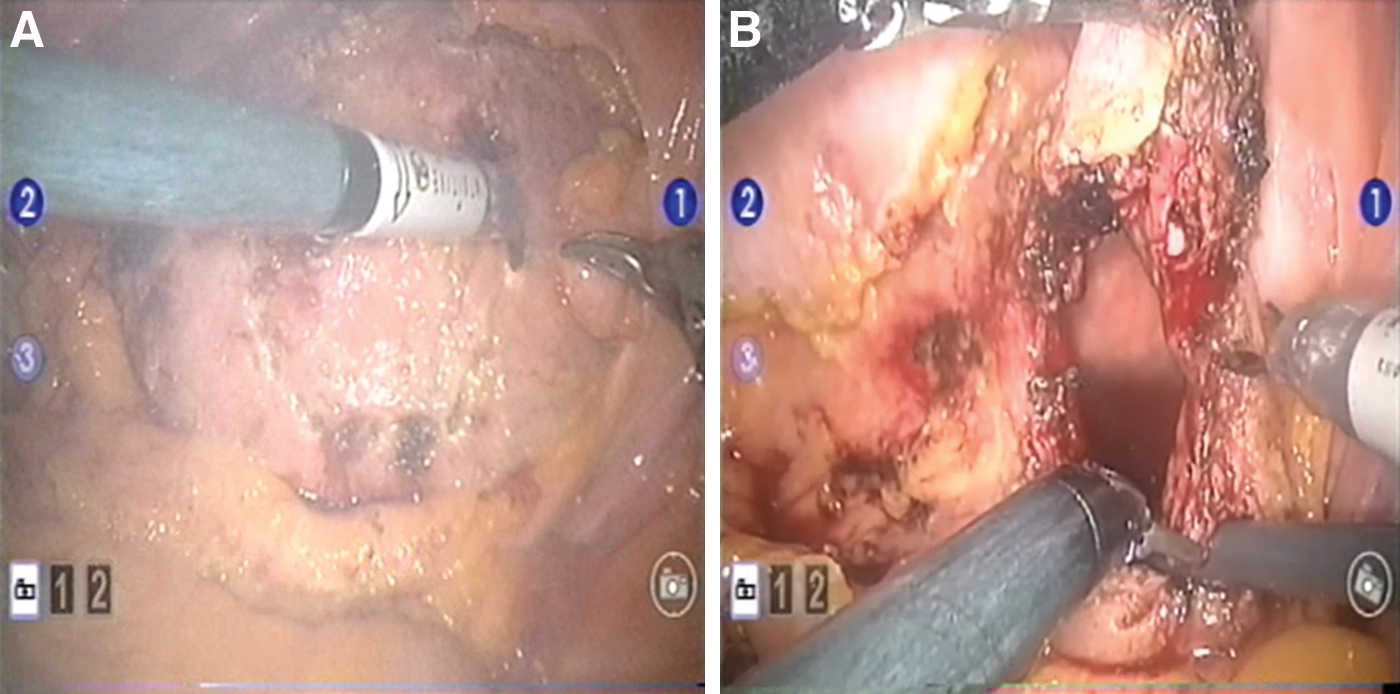
Creation of posterior bladder flap.
A 30–40-cm segment of ileum, located 15–20 cm proximal to the ileocecal junction, was then identified. The surgeon used blunt dissection with endowrist hot shears and Maryland bipolar forceps (Intuitive Surgical) to create mesenteric windows and the isolated segment was then harvested with an endo GIA stapler (Covidien, Mansfield, MA). The surgeon then resected or isolated the staple lines from the harvested bowel segment, incised the antimesenteric border of the bowel to completely detubularize the segment, and sewed the medial edges together with 2-0 absorbable polyglactin 910 suture (18 cm in length) to create an intracorporeal U-shaped ileal augment patch. The abdomen was copiously irrigated during this process to prevent contamination. If a continent stoma was planned, detubularization began 5 cm from the bowel end and an intracorporeal stoma was created by tapering this 5 cm native bowel segment over a 14F catheter with 3-0 polyglactin 910 suture (10 cm in length). Alternatively, a Yang-Monti reconstruction and reimplantation technique was used to create the continent stoma limb.
After the ileal patch was created, the patch base was then oriented with the base of the U-shaped cystotomy with an interrupted absorbable suture. The vesicoenteric anastomosis began at this orienting suture and ran, full thickness, up both sides of the U-shaped cystotomy (Fig. 3). The augment was closed along the top wall by laying the elevated U-shaped detrusor flap over the remaining open patch segment and suturing the edge together to complete the top wall closure. The anastomosis was then tested by irrigating the bladder with 200 mL of sterile water.

Development of vesicoenteric anastomosis.
After completing the augment anastomosis, the trocars were removed, and a 4-cm fasciotomy was made at either a previously marked stoma site or two fingerbreadths above the pubic symphysis. The native bowel segments were then retrieved from the abdomen and an extracorporeal side-to-side stapled anastomosis was performed. The reconnected bowel was then returned to the abdominal cavity. If indicated, the previously constructed continent stoma was then delivered through this counterincision and matured.
Postoperative care
The urethral catheter was kept open to drainage for 3 weeks. Patients were evaluated by a neurourologist and continence center nurse at 3 weeks postoperative, 3 months, 9 months, and then annually. Cystograms were performed at 3 weeks, immediately prior to catheter removal (Fig. 4). Continence status was assessed at each visit by asking the patient and caregiver if he/she experienced urethral incontinence in the preceding week prior to visit. Bladder capacity was measured through catheterization and/or assessing time intervals between catheterization. Renal ultrasonographs were obtained after the second postoperative visit and then annually. Urodynamics were obtained when convenient for the patient and/or to address a specific urinary symptom.
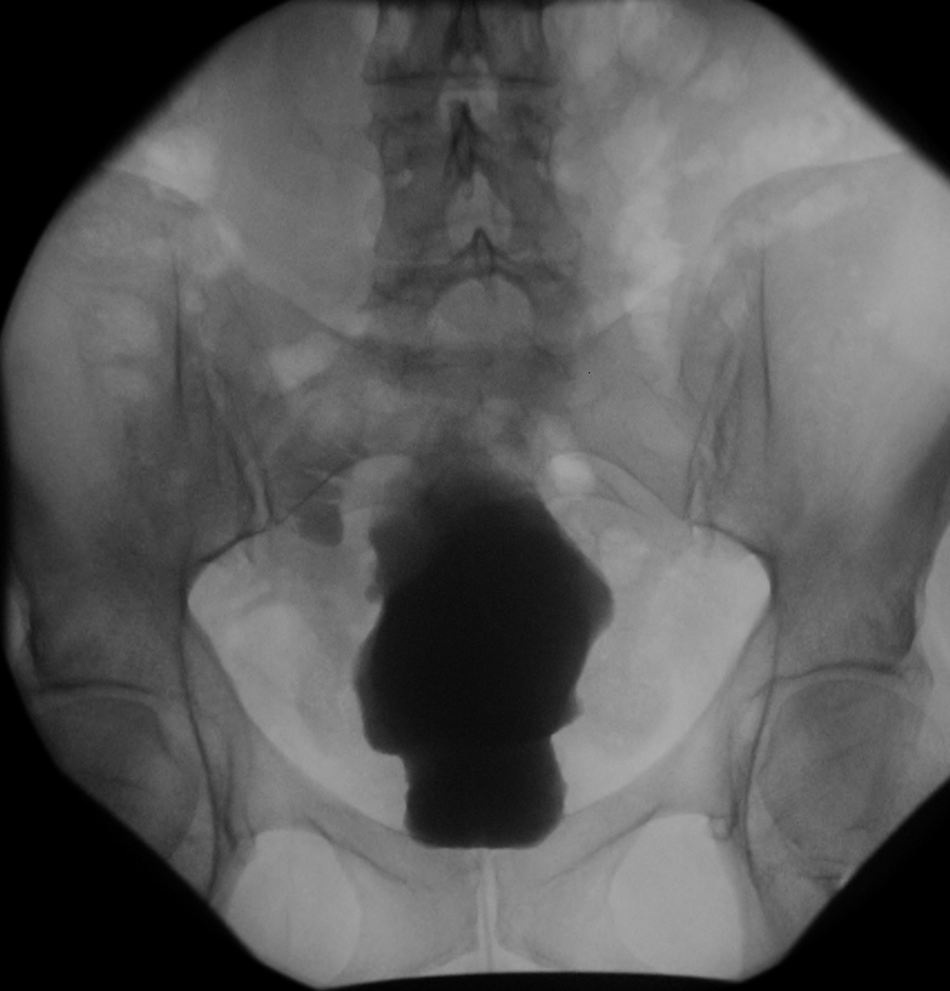
Postoperative cystogram at 3 weeks. Opacified bowel at superior aspect of augment is incompletely filled augment cavity.
Results
Between March 2007 and April 2009, five robotic enterocystoplasties (four women) were performed. Three patients had concomitant continent stomas created during the enterocystoplasty. Four of the robotic procedures were completed successfully and one procedure (patient 2 in the series) was converted to open (using the 5-cm planned stoma incision) because of a robotic electrical malfunction after >75% of the vesico-enteric anastomosis was completed. If this technical complication had not occurred, the procedure would have been completed without conversion.
Mean patient age was 43 years (range: 24–55). Etiology for a neurogenic bladder included cervical spinal cord injury in three and multiple sclerosis in two patients. On preoperative urodynamics, mean maximum bladder capacity was 110 cc (range: 70–220) and mean bladder compliance was H2O 9.6 mL/cm (range: 2.5–30.0). Four patients also demonstrated significant detrusor overactivity during urodynamics. No patient has stress incontinence. One patient also had bilateral grade 5 vesicoureteral reflux on preoperative cystogram.
Mean operative time, from induction to extubation, was 6.4 hours (range: 5.9–7.3). Over the five-patient cohort, the operative time sequentially decreased. Mean estimated blood loss was 180 mL (range: 100–250) and no patients required blood transfusion. Bowel function, defined as passing of flatus, resumed at a mean number of 5 days (range: 3–7) postoperative and mean hospital stay was 7 days (range: 5–9). The mean total inpatient direct cost for patients in this series was $34,137 (range: 28,610–40,865). The mean operating room (OR) supply costs per case were $3907 (range: 3644–4105). Over a median follow-up of 192 days (range: 75–369), all patients exhibited stable renal function after robotic enterocystoplasty (median creatinine preoperative 0.76 vs. postoperative 0.72, p = 0.74). Although two patients demonstrated moderate bilateral hydronephrosis on preoperative imaging, all five patients had normal-appearing upper tracts on most recent postoperative imaging. At last follow-up, all patients were able to store urine for at least 3 to 4 hours and/or catheterize for volumes >300 cc (Fig. 5). Postoperative urodynamics for two patients demonstrated high bladder compliances of H2O 50 and 150 mL/cm. All patients reported being dry per urethra at his/her last follow-up appointment.
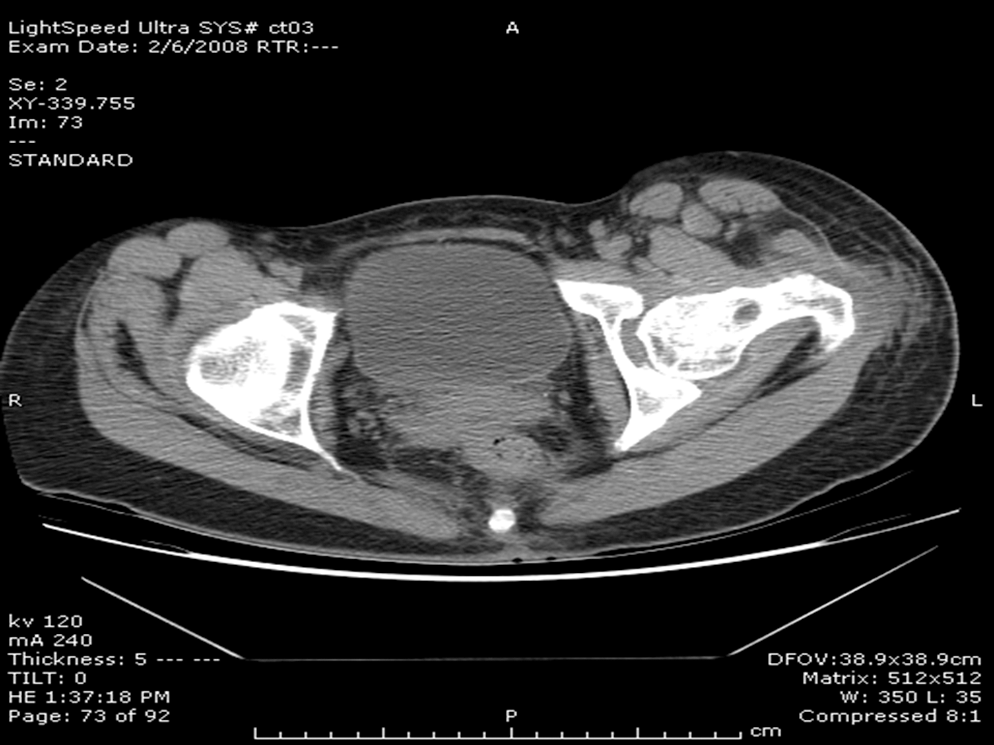
Computed tomography demonstrating intact and functional bladder augment at 6 months after the procedure.
No perioperative complications occurred. Three Clavian-grade postoperative complication occurred, including a postoperative ileus related to a small postoperative urinoma (Clavian grade 1), chronic urinary tract infections related to persistant vesicoureteral reflux (Clavian grade 2), and incontinence per stoma (Clavian grade 3). No patients experienced postoperative wound infections. The patient with persistent vesicoureteral reflux was treated with transurethral periureteral collagen injections and the patient with stoma incontinence underwent stoma revision surgery.
Discussion
Enterocystoplasty is a viable treatment option for patients with refractory neurogenic bladder symptoms. With the advent of minimally invasive surgery, several investigators have proven the safety and efficacy of a laparoscopic enterocystoplasty procedure. 1 –5 However, these series also describe a long learning curve that required advanced laparoscopic suturing skills. In theory, robot-assisted enterocystoplasty can yield minimally invasive advantages similar to pure laparoscopy, but without the same suturing demands. Al-Othman et al 7 demonstrated the feasibility of a robotic enterocystoplasty in an initial case report, but there are no additional case series on this technique. Our data on five consecutive patients who underwent robot-assisted enterocystoplasty confirms initial observations that the procedure can be performed safely and with good patient outcomes.
All five patients in our series demonstrated improved bladder capacity, improved urethral continence, and upper tract protection after the procedure. These outcomes mirror data from laparoscopic enterocystoplasty techniques. In El-Feel's 23 patient series, laparoscopic ileocystoplasty improved bladder capacity from a mean value of 111 to 778 cc after the procedure. 9 Likewise, Gill et al 3 reported improvement in a smaller laparoscopic series. Mean operative time in our series was considerable (6.4 hours), but also similar to other laparoscopic case times, which ranged from a mean value of 3.4 to 7.0 hours. 3,9,10 Further, our initial efficacy and safety data are comparable to open enterocystoplasty outcomes. 11 A longer follow-up and more patients will be needed to draw a better comparison between enterocystoplasty technique outcomes.
With the exception of a brief ileus in one patient, the robotic procedure did not incur any significant intraoperative or perioperative complication. We attribute the low incidence of bowel complications to our use of an extracorporeal bowel anastomosis to re-establish bowel continuity, instead of an intracorporeal anastomosis technique. Elliott et al 4 commented on the technical difficulty associated with performing an intracorporeal bowel anastomosis and Passerotti et al 12 reported an intraperitoneal bowel leak after using an intracorporeal stapling technique in their procine model. Other authors have also reported few bowel complications when an extracorporeal bowel anastomosis was utilized, although the intracorporeal technique has been utilized in the general surgery literature. 3,6,13,14 A larger patient series is needed to determine if the robotic technique reduces other complications commonly associated with enterocystoplasty, such as bladder stones, urinary tract infections, and wound infections.
In contrast to other laparoscopic enterocystoplasty series, we created an ileal augment patch via an intracorporeal technique. It is likely that authors using pure laparoscopy utilized an extracorporeal technique to minimize the amount of intracorporeal suturing, which is known to require a high laparoscopic technical skill level. 6,15 In our experience, robot-assisted laparoscopy greatly facilitated creation of the detubularized ileal patch and operative times sequentially decreased from 7.3 to 5.9 hours for the five patients. We found that when the assistant applied counter-traction to “flatten out” the medial edges, suturing speed increased because of better visibility of tissue edges. However, we see no technical reasons as to why an extracorporeal ileal patch could not be used with robotic enterocystoplasty.
At this juncture, the advantages of robotic enterocystoplasty can only be considered theoretical, which must be compared against a high cost per procedure. Benefits traditionally associated with robotic surgery, such as decreased pain requirements and more rapid return to health, 16,17 are difficult to assess in a small neurologically compromised patient population. Further, as pain requirements differ across patients with different neurological diagnosis, it is challenging to assess how robotics affects the postoperative analgesia need. Finally, bowel function in our series returned on mean postoperative day 5 and patients left the hospital on postoperative day 7. These numbers compare favorably against contemporary open enterocystoplasty data. 18 If a length of stay difference is proven in a randomized study with an open cohort, robotic enterocystoplasty could prove advantageous for patient care.
We realize that our study has several limitations. Most importantly, this study is a retrospective review of patients seeking the robotic enterocystoplasty procedure and thus may be influenced by selection bias. As mentioned previously, a randomized study comparing open versus robotic enterocystoplasty with identical pre- and postoperative plans would provide a more valid comparison. Further, as quality-of-life questionnaires were not used in the study, it is difficult to measure patient satisfaction. Although all patients reported being dry per urethra, a validated quality-of-life questionnaire would better measure patient-perceived improvement and satisfaction with the recovery. When comparing this with a similar open cohort, differences in patients' perception of quality of life may be found.
Despite these limitations, robotic enterocystoplasty appears to be a viable surgical technique in this consecutive patient series. This information is important to understand prior to committing resources to comparative randomized outcome analyzes with the open procedure. We suggest that investigating potential benefits of the robotic technique, compared with the open standard, may yield improvements in patient care. However, any potential benefit needs to be weighed against the contemporary cost associated with robotic instrument usage in the operating room. Further, experience and longer follow-up are needed to validate patient outcomes and utility of this newly evolving technology.
Conclusions
Robotic enterocystoplasty can be performed safely and effectively. All patients reported improvement in urethral continence and bladder storage, with minimal morbidity.
Footnotes
Disclosure Statement
No competing financial interests exist.