
Abstract
Purpose:
To evaluate the feasibility and safety of two or three concomitant laparoscopic procedures in the same patient in one anesthesia session.
Patients and Methods:
Data were reviewed for 32 patients for whom two or three concomitant laparoscopic surgeries at our institution were considered. Preoperative details, port position, surgical time, blood loss, complications, hospital stay, and postoperative recovery were analyzed.
Results:
Thirty-two patients underwent two concomitant laparoscopic procedures and one patient three procedures. Surgical time was increased by 6 minutes because of the repositioning time of the patients. There were no complications during all procedures, and hospital stay was not increased, being limited only by the first procedure.
Conclusion:
Planned laparoscopic surgery for two or three urologic malignancies is feasible in one anesthesia session, thereby reducing cost and overall hospital stay for the patient without any increased risk of perioperative morbidity. The decision to continue with the second or the third procedures depends on the successful conclusion of the former procedures in a reasonable time and without any complications.
Introduction
Large series of laparoscopic radical prostatectomies (LRPs), radical nephrectomies, partial nephrectomies (LPNs), and adrenalectomies, have been reported with excellent results as a single procedure. 2 –4.
Traditionally, single-setting surgical treatment of synchronous pathologic conditions has been condemned because of the increased risks for the patient. Excessive morbidity and mortality and an extended recovery period were reported for patients who underwent open surgery for bilateral renal pathologic features. 5 –8
We review our experience with a single-setting transperitoneal laparoscopic approach to urologic synchronous tumors in one anesthesia session.
Patients and Methods
We performed a retrospective chart review of all patients who had undergone laparoscopic single-setting surgery for synchronous tumors and collected preoperative, operative, and follow-up data.
Between May 2004 and May 2009, 32 patients with synchronous urologic tumors underwent laparoscopic surgery in a single operative session. All cases were performed using a transperitoneal approach. Age, body mass index and preoperative American Society of Anesthesiologists score were not considered absolute contraindication to single-setting procedures. All patients with adrenal masses underwent endocrinology evaluation and complete serum and urine hormonal screening before surgery. Preoperative data are summarized in Table 1.
PSA = prostate specific antigen; GS = Gleason score; RP = radical prostatectomy; PN = partial nephrectomy; SEA = superselective transarterial embolization; VHL = von Hippel-Lindau; RCC = renal-cell carcinoma; BMI = body mass index; ASA = American Society of Anesthesiologists.
Surgical technique
Laparoscopic approach to prostate cancer and coexistent renal or adrenal tumors
The first step was laparoscopic radical nephrectomy (LRN)/LPN or laparoscopic adrenalectomy (LA). We performed a four-trocar transperitoneal access with patients in the extended flank position. First, a 12-mm trocar for the camera is placed at the level of the umbilicus using the open Hasson technique; a 10-mm trocar is placed at the iliac fossa, midway between the umbilicus and the anterior superior iliac spine; and two 5-mm trocars are inserted along the midclavicular line in the upper abdominal quadrant and along the anterior axillary line just below the last rib.
Laparoscopic PN after superselective transarterial embolization was performed for tumor diameter >4 cm or intraparenchymal depth >1.5 cm. Details of this technique are described in a previous report. 9
For small exophytic renal tumors, we used a no-clamp, no-suture technique. Hilum vessels were not clamped and were not isolated. The renal parenchyma was incised with a monopolar scissor just a few millimeters below the renal tumor, and the dissection plane was found using the 10-mm LigaSure. After having identified the cleavage plane, the LigaSure allowed us to minimize the intraoperative bleeding and to reduce the time for PN. The hemostasis of the surgical bed was completed with the LigaSure or with monopolar coagulation and then using a bolster of Surgicel, TachoSil, or Tabotamp alternatively. In most cases, the Gerota fascia was closed with a running suture, and a drain was placed into the perinephric tissue close to the renal bed.
We performed LA using the 10-mm LigaSure sealing system. No clip or ligature was applied to adrenal vessels, and tumor dissection and vessels sealing was performed using only a 10-mm LigaSure.
Once the first procedure was completed, the specimen was placed into an endobag, and the endobag was secured to a port. At the conclusion of the operation, it was removed together with the other specimen through the same port.
For LRP, we moved the patient into a supine position, and we used the same trocar for the camera.
If the previous procedure on the renal or adrenal gland was performed on the left side, other 10-mm and 5-mm trocars were positioned in the left iliac fossa, and another 5-mm trocar was inserted into the right iliac fossa.
If the previous procedure on the renal or adrenal gland was performed on the right side, we used the same 5-mm trocar, and we added two trocars along the midclavicular line: One 10-mm trocar at the level of the camera port and another one in the iliac fossa.
Then LRP was performed in an antegrade manner in all cases.
Laparoscopic approach to bilateral renal and/or adrenal tumors
We performed a four- trocar transperitoneal access with patients in the extended flank position. The first step was always to perform LRN when indicated. In the case of bilateral LPN or LA, priority was given to the most challenging procedure. In the case of concomitant renal and adrenal malignancies, we always began performing LRN or LPN. Once the first procedure was completed, the patient was repositioned, and we used the same trocar for the camera. Also in this case, the specimen was placed into an endobag, and the endobag was secured to a port (Fig. 1). At the conclusion, it was removed together with the other specimen through the same port (Fig. 2).
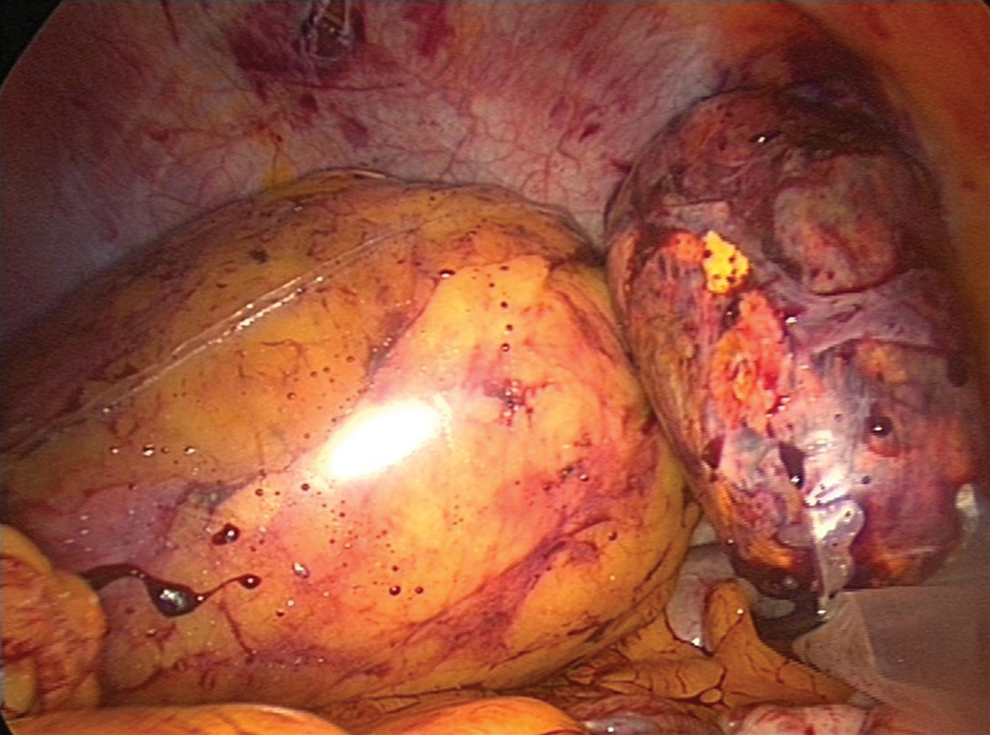
Kidney and adrenal gland placed into endobags that are secured to a port.
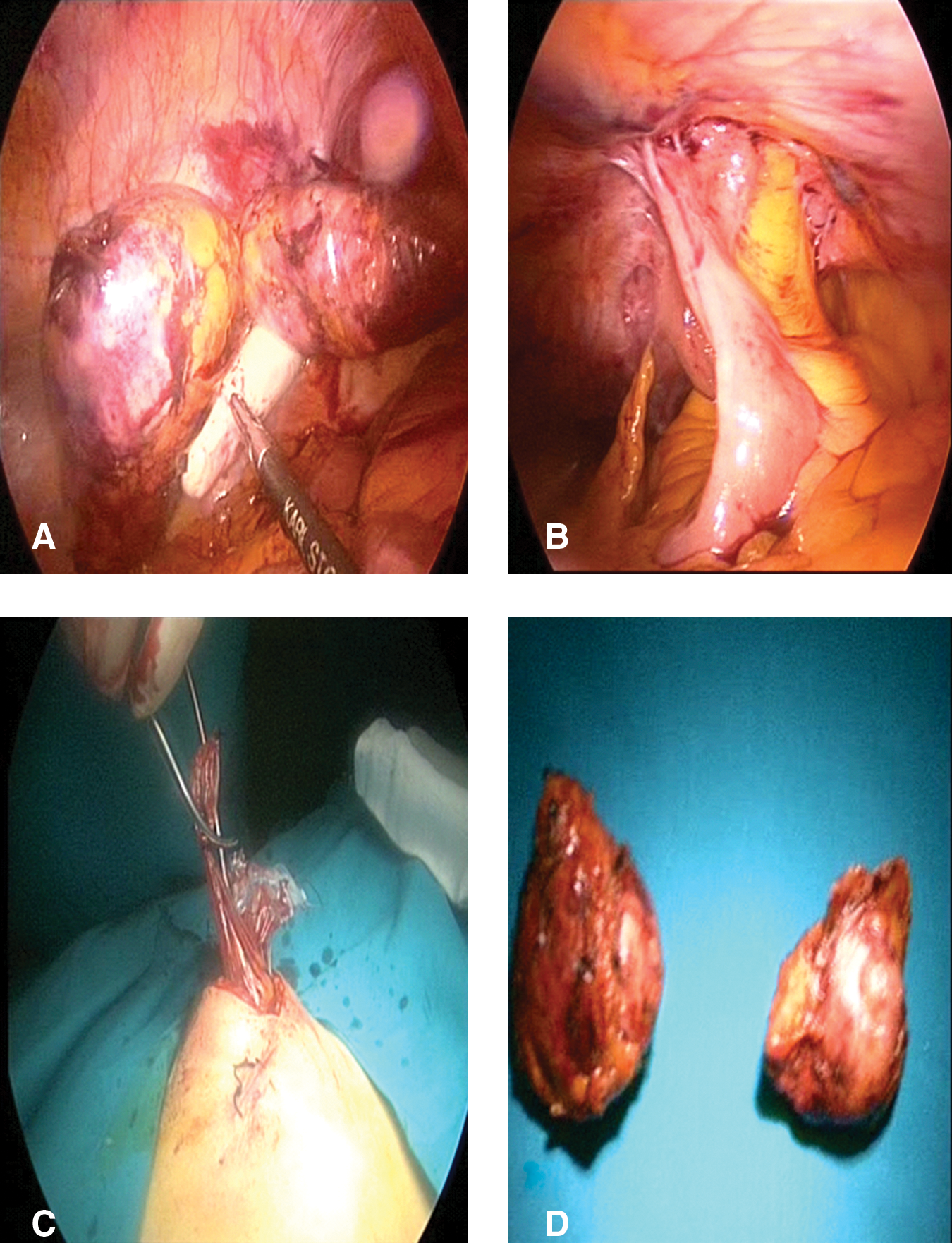
Bilateral removal of adrenal metastases in a patient who had previously undergone radical cystectomy and ileal conduit.
Laparoscopic approach to ipsilateral renal and adrenal tumors
We performed a four-trocar transperitoneal access with patients in the extended flank position Also in these cases, the first step was to perform LPN. Special care was taken to place trocars to avoid placing any further ports. Specimens were removed through the same port in a separate endobag.
Results
Thirty-two patients successfully underwent simultaneous laparoscopic procedures. Operative data, pathologic stage, and follow-up are summarized in Table 2. The mean repositioning time was 6 minutes (5–10 min). No conversion to an open approach was needed. No specific major surgical complication or hampered recovery of the patients because of the second or third procedures occurred. Moreover, no late complication from the combined procedure was observed during the follow-up (range 10–58 months).
ccRCC = clear-cell renal-cell carcinoma; DF = disease free.
The median postoperative hemoglobin decrease was 2.5 mg/dL (range 0.4–7.4 mg/dL). Patients returned to oral intake at a mean of 2 days and were ambulating 24 hours postoperatively. Patients had a median postoperative analgesic requirement of 40.5 mg morphine equivalents (range 2–278). Patients returned to full activity at a mean of 18.5 days (9–25).
Discussion
Most patients with more than one urologic disease undergo surgery depending on which pathology is estimated to have priority of treatment. The advantages of the laparoscopic approach in the management of multiple urologic diseases have been reported by several authors. Reisiger and associates 10 have shown that single-setting bilateral laparoscopic renal procedures are safe and do not increase morbidity; the authors advocate this approach and argue that with one anesthetic insult, both risks for the patients and costs of another procedure are reduced. Gill and colleagues 11 reported that laparoscopic bilateral synchronous nephrectomy in selected patients with symptomatic autosomal dominant polycystic kidney disease and renal failure is feasible, safe, and efficacious. Mikhail and coworkers 12 compared open vs laparoscopic simultaneous bilateral adrenalectomy and showed how the laparoscopic approach resulted in decreased blood loss, lower transfusion rate, and a trend toward a short hospital stay, although the operative time was longer. 12–13
The main problems related to a combined laparoscopic procedures are oncologic effectiveness, patient safety, operative time, technical difficulties, and the effect of one procedure on the outcome of the other if performed consecutively. This is particularly relevant when laparoscopic surgery involves kidneys, and it could, for example, put the patient at risk of acute renal failure. Therefore, a risk-benefit assessment concerning continuation with the second procedure should always be performed in consultation with the anesthesia members at the end of each single procedure.
The rationale for performing two or three procedures in the same session include: Single anesthetic insult, fewer ports, a single recovery period, shorter overall hospital stay, and early return to full activity, with time and cost saving for patients and hospitals.
Despite a variety of advantages, several reservations are present. The anesthesia and the surgical time could result in being excessively long, complications of each procedure may be added, and blood loss increased by performing more than one procedure. Therefore, it is important to select suitable cases according to personal surgical skills.
In our experience, all procedures were successfully completed. No patients needed conversion to an open procedure. No major complications or rehospitalization occurred, and mean hospital stay was not increased because of the second or third in tandem performed procedure. The retroperitoneal or transperitoneal approach depends on the preference of the surgeon. All our laparoscopic procedures are usually performed by transperitoneal access, and we believe that it is particularly advantageous when you have to treat more than one disease; it allowed us to create a single working space and to monitor the operating field of the previously performed procedures.
Although we did not report any complications, the single-setting laparoscopic approach to synchronous urologic tumors should be performed by surgeons with experience in laparoscopy and in selected centers. A long operative time could not allow surgeons to conclude all procedures laparoscopically, and it may result in a higher conversion rate to open surgery.
Conclusion
The laparoscopic approach to synchronous urologic malignancies in one anesthesia session is feasible. Furthermore, patients need only a single procedure and avoiding two or three visits to the operating theater and repeated anesthesia exposure. The intervention should only be performed if the primary portion of the procedure is completed expeditiously and without complications. A surgeon with extensive experience in laparoscopic surgery should be mandatory.
Footnotes
Acknowledgment
Emanuela Altobelli contributed to data collection.
Disclosure Statement
No competing financial interests exist.