
Abstract
Purpose:
Alpha blockade has been well described clinically for expulsion of distal ureteral stone. However, the in-vivo effects of α-blockade on ureteral dynamics during stone passage are not clear. We studied the effects of oral alfuzosin on ureteral pressure and peristalsis in a distally obstructed porcine ureter.
Methods:
Twenty-four female domestic swine (75–82 kg) were incorporated into the study. The study was powered to detect a 30% difference in distal ureteral pressure, with a secondary endpoint of frequency of ureteral peristalsis. The animals were divided into four equal groups: a control group without α-blockade or ureteral obstruction, a group with α-blockade and no ureteral obstruction, a cohort without α-blockade but with distal ureteral obstruction, and a group with α-blockade and distal obstruction. Peristalsis was measured by a magnetic sensor and ureteral pressure through a 5F ureteral balloon catheter. Observations were recorded for 10-minute intervals every hour for 5 consecutive hours.
Results:
There was increase in ureteral pressure and peristaltic rate with distal ureteral obstruction (p < 0.01). Alpha blockade did not produce significant changes in the above parameters with or without ureteral obstruction compared with the nonmedicated groups. We observed a 0.2 mm Hg lower increase in change of ureteral pressure during peristalsis compared with resting ureteral pressure (delta pressure) in the treated obstructed model (95% confidence interval: −0.55 −0.10; p = 0.06).
Conclusions:
In the porcine model, alfuzosin appears to decrease the delta pressure in the distal ureter during obstruction; however, statistical significance was not reached. Further investigation into the in-vivo physiology of medical expulsive therapy is warranted.
Introduction
The mechanisms for the observed clinical responses to α-blockade in obstructed or partially obstructed ureter are not well understood. Investigations to characterize the physiological effects of alpha blockade upon the distal ureter have been predominantly in-vitro studies of ureteral contractility exposed to different agents. 3 –5 Studying the in-vivo effects of an alpha blocker on ureteral dynamics such as ureteral peristalsis and intraureteral pressure may be important in understanding the mechanisms of stone passage by MET. We sought to characterize the effects of orally administered α-blockade in an in-vivo model simulating obstructive ureteral urolithiasis.
Methods
Institutional review board approval for animal studies was obtained. The study was powered with a primary endpoint of measuring a 30% difference in distal ureteral pressure. Secondary endpoints were number of observed and measured ureteral peristalsis. Twenty-four female domestic swine (73–82 kg) were divided into four equal groups: a control group without pharmacology and without distal ureteral obstruction (group I), a cohort without α-blockade but with distal ureteral obstruction (group II), a group with α-blockade and no distal ureteral obstruction (group III), and a group with both α-blockade and distal obstruction (group IV).
Pigs were acclimated to the research facility for 72 hours prior to ureteral study. Those in the pharmaceutical cohorts received 20 mg alfuzosin HCl with meals twice daily for the 2 days preceding surgery (total dose: 80 mg). This dosage was established after confirming the serum and urinary alfuzosin levels in two animals and from previous alfuzosin human pharmacologic dosage studies. 6
Before the pig was anesthetized, serum and urine specimens were taken and frozen in liquid nitrogen for later quantitative measurement of alfuzosin. Each animal was intubated and anesthesia maintained using isoflurane (2.5%–4%) and fentanyl. Ketamine and atropine were not used because of their known effects on ureteral peristalsis. Pulse oximeter and blood pressure monitor for mean arterial pressure were utilized during the procedure to ensure adequate renal blood flow. The subject was placed in the lateral decubitus position with the right side up. Cystoscopy was performed and a 5F Occluder® (Boston Scientific) ureteral occlusion balloon was placed over a 0.025″ Glide wire into the distal ureter and a Foley catheter was inserted into the urinary bladder. A lumbotomy incision was made on the right side, and the kidney and ureter were exposed. Care was taken to perform very minimal dissection of the ureter, and small windows were developed posterior to the ureter for placement of a previously described giant magneto resistive sensor and an electromyography (EMG) electrode to measure ureteral peristalsis by extraluminal method 7 (Fig. 1). The position of the distal ureteral catheter was palpably and visually confirmed and connected to a calibrated pressure transducer. The ureter was then allowed to rest free of manipulation for 45–60 minutes to establish a baseline activity. In the obstructed groups, the occlusion balloon was positioned and inflated to mimic a distal ureteral stone. Also, occlusion was confirmed visually following inflation. The inputs from the EMG electrode, magnetic sensor, and pressure transducer were recorded on a computer using WinDAQ Version 2.46 (©1992–2006 Data-Q Instrument). All the tracings could be viewed simultaneously in real time using this software. In addition, the peristaltic activity was visually confirmed and recorded.
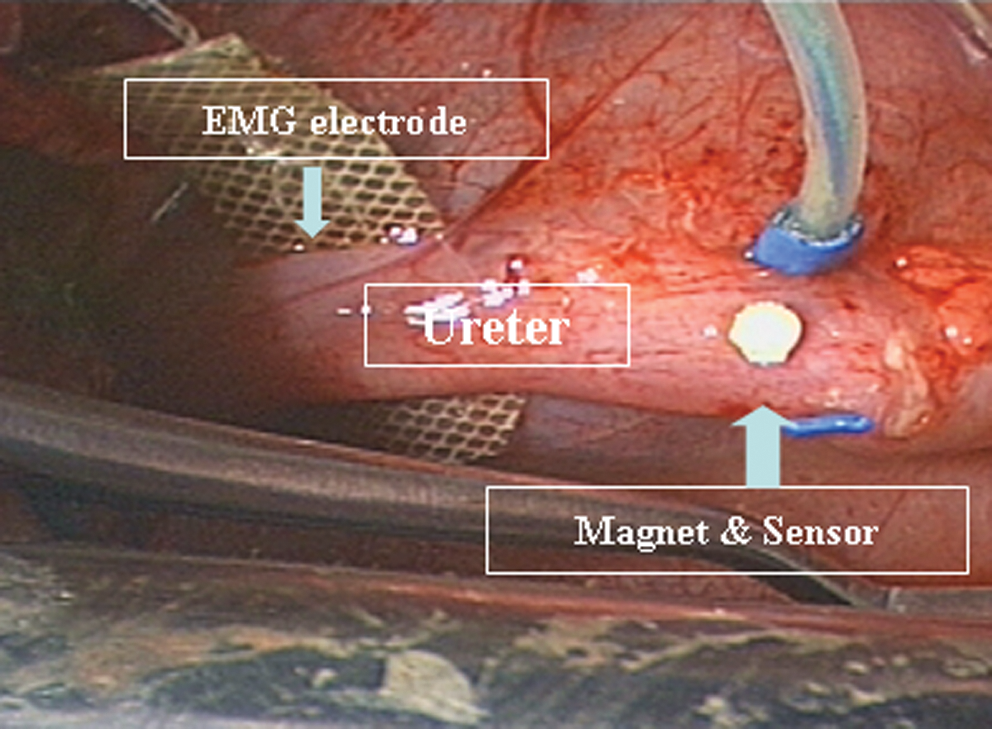
Electromyography (EMG) and giant magnetoresistive (GMR) magnetic sensor configuration.
Baseline distal ureteral pressures both at rest and during peristalsis as well as number of peristalsis during a 10-minute interval were measured every hour for 5 consecutive hours. We also measured the changes in the ureteral pressure during peristalsis compared with that during interperistaltic phase (delta pressure). The means and medians of the above parameters were calculated for each hour of observation. Intravenous hydration was maintained at 5 mL lactated Ringer's solution per kilogram per hour for the duration of the surgery. Urine output and mean arterial pressure were recorded at hourly intervals. One-way repeated measures analysis of variance was utilized to evaluate the differences in pressure changes and peristalsis across temporal points. Comparisons were made between the average changes per subject, and not the difference between the averages, to reflect true changes at each peristaltic activity in that particular animal, which acts as its own internal control.
Two swine were excluded and replaced with two other subjects, as monitoring of peristalsis was lost during the middle of the observational portion of the procedure. One subject's pressure data in the obstructed without pharmacology group was excluded, as the pressure sensor was found to be ruptured following the surgery.
Urine and serum samples were extracted for alfuzosin measurement. Five hundred microliters each of the above samples was extracted before the above procedure with 3 mL diethyl ether. Samples and standard alfuzosin were introduced into a high-performance liquid chromatography (HPLC) system. Samples were analyzed in triplicate to allow for calibration of means and standard deviations. Standard curves were established for 500 fmol to 500 nmol of injected alfuzosin. Linearity of the standard curve was r 2 = 0.985.
Results
The mean and median ureteral pressures and rate of peristalsis are tabulated in Table 1. The average baseline ureteral pressure during resting phase across all four groups was 2.52 mm Hg (2.1–3) and it was 2.95 mm Hg (2.7–3.1) during peristalsis. The mean baseline peristaltic rate among all 4 groups was 18 per 10 minutes (17.6–21.6). There was no significant difference in the mean arterial pressure and urine output among different animal groups (mean: 62.4 mm Hg, p = 0.97, 95% confidence interval [CI]: −14.1–14.7; and mean: 76.2 mL/hour, p = 0.38, 95% CI: −18.5–46.8, respectively).
occ. = ureteral occlusion.
There was an increase in the distal ureteral pressure and rate of peristalsis in the animal groups with distal ureteral obstruction (groups II and IV) compared with the nonobstructed groups (groups I and IV) (p < 0.01 for both comparisons; Fig. 2). Immediately following occlusion, the number of peristalsis elevated acutely in groups II and IV and then decreased more rapidly in the alpha blockade group (Table 1). In the animals with α-blockade but without ureteral obstruction (group III), there was no significant change in the mean and median peristaltic rate and distal ureteral pressures compared with the control animals with no drug therapy and no ureteral obstruction (group I). In those animals with ureteral obstruction, the alpha blockade group (group IV) showed a trend in decrease in peristaltic rate compared with the animal group on α-blockade (group II). However, α-blockade did not show any statistically significant difference in the ureteral pressure or peristalsis with ureteral obstruction compared with the nonmedicated obstructed group (p > 0.10 for both).
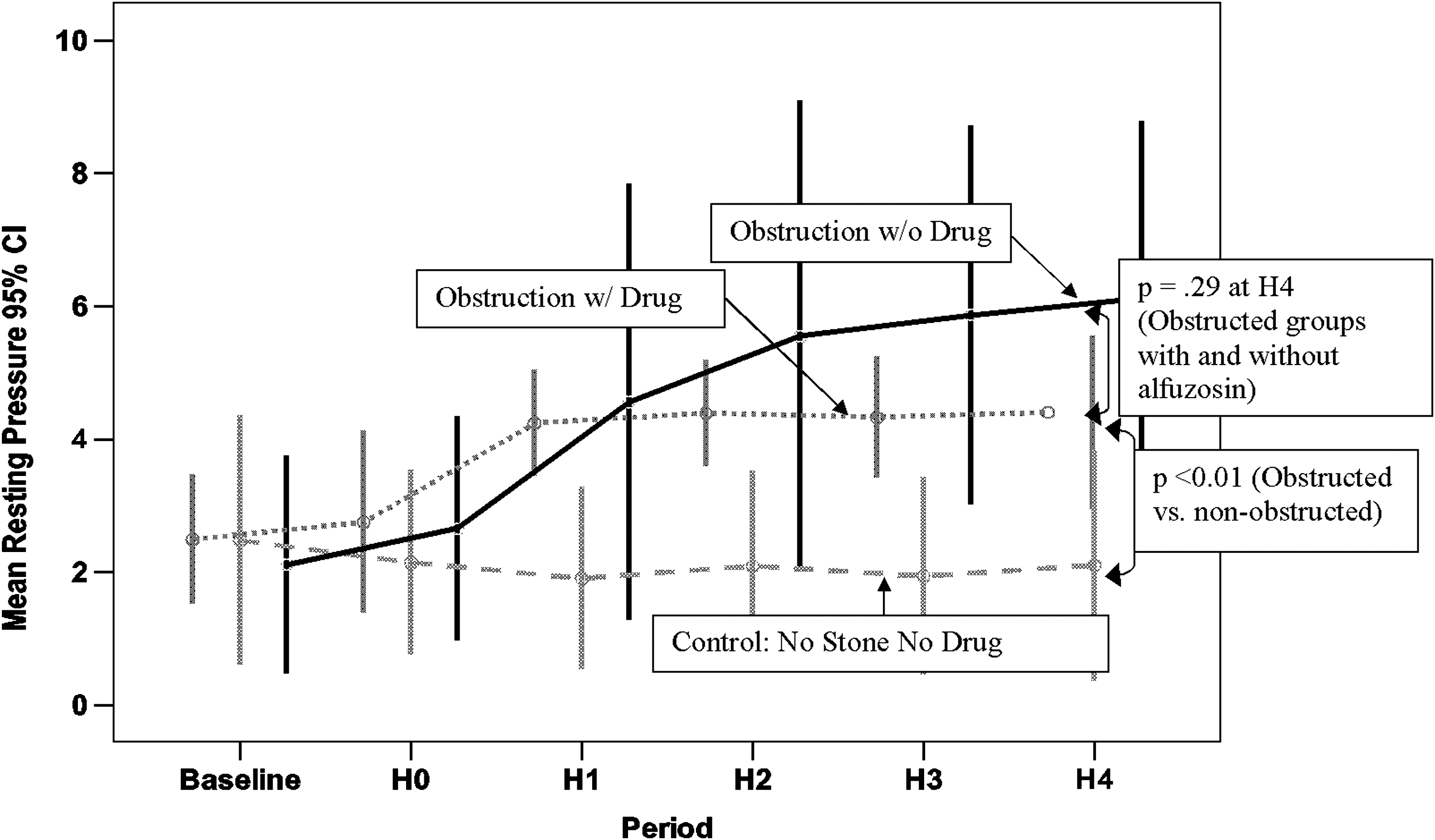
Resting ureteral pressure changes with and without alfuzosin in the obstructed groups compared to the control group. CI = confidence interval; H = hour.
The delta pressure (change in ureteral pressure from baseline to that during peristalsis) was calculated for all animal groups. The delta pressure with peristalsis was 0.225 mm Hg lower in the alpha blockade and obstructed group (group IV) compared with the untreated and obstructed group (group II) (Fig. 3). By one-way repeated measures analysis of variance, the resultant p-value was 0.066 (95% CI: −0.55–0.10) for the change between resting and peristaltic pressure over time. In the α-blockade group with ureteral obstruction, the delta pressure showed very minimal variation compared with the obstructed group with no α-blockade. Alpha blockade appeared to have much less effect upon the number of peristalsis in the unobstructed group. Also, over time, the number of peristalsis decreased in all cohorts. Comparing the obstructed cohorts, there were an average of 37% fewer visualized peristalsis and 35% fewer magnetically detected peristalsis over time (95% CI: −17.5–4.9, p = 0.253; and 95% CI: −17.5–5.5, p = 0.292, respectively).

Delta distal ureteral pressure in obstructed groups.
Serum specimens showed consistent drug levels in 6 of 12 (50%) animals. Other samples were compromised during shipping for HPLC; this combined with precipitation of some specimens precluded complete reporting of accurate quantitative values.
Discussion
Two recently reported meta-analyses of MET have shown improved stone passage rates and increased patient comfort. 1,2 Although clinical evidence for MET accumulates, the physiological mechanisms remain elusive. Most hypotheses derive from reported in-vitro data of varying agents, concentrations, and buffers. 3 –5 A decade ago, Nakada et al 8 reported that Cox-2 inhibition significantly decreased ureteral contractility in both porcine and human ureteral segments in vitro. However, a recently reported randomized controlled clinical trial of Cox-2 inhibition in obstructing ureteral stones <10 mm failed to show increased stone passage rates or improved patient pain scores. 9 Extrapolating hypotheses from in-vitro data becomes difficult when well-performed in-vitro studies demonstrate that both Cox-2 inhibition and alpha blockade decrease ureteral contractility, yet alpha blockade appears more clinically effective. 3,8,9 Clearly, an in-vivo model to evaluate ureteral dynamics during treatment would help elucidate mechanisms.
Davenport et al 10 described a human in-vivo model with indwelling ureteral catheter in normal contralateral ureter in patients undergoing ureteroscopy, for 24 hours during oral tamsulosin therapy, and found a decrease in ureteral pressure but no change in peristalsis frequency. As they noted, however, ureteral catheter placement itself has shown effects on frequency of peristalsis. 11 Another in-vivo report of pharmacological effects on ureteral peristalsis utilized a topical intraluminal ureteral delivery that would be difficult to implement in MET. 7
Without an in-vivo model we are left to either surmise which agents may be effective based upon in-vitro studies or take demonstrated clinically effective drugs from the bedside into the lab to investigate mechanisms. Either approach leaves the underlying physiology during obstruction and treatment a matter of conjecture. We sought to design an in-vivo animal model that would closely reproduce the clinical features of obstructing urolithiasis during alpha blockade administration.
When designing the study we sought to detect a 30% difference in ureteral pressure change during peristalsis. This allowed controlling for baseline ureteral pressure differences influenced by preoperative hydration status or insertion of the distal ureteral catheter into varying diameter lumens. Also, each subject then acted as its own pseudo-control by focusing on pressure alterations over time within the same subject and using repeated measure tests to evaluate the statistical significance. Obviously, the primary limitation of the study was failure to reach significance for the primary endpoint. Unfortunately, the variance encountered between subjects exceeded anticipation and left us desiring to carry out more controlled environments of in-vitro investigations. Although a decrease in ureteral pressure alterations was observed between the treated and untreated obstructed groups, it failed to reach significance (p = 0.066). Delta ureteral pressure (change in ureteral pressure during rest to that during peristalsis) may be one of the important factors in stone passage. In the α-blockade group, there was very minimal variation in delta pressure compared with the nonmedicated group, which could facilitate effective peristalsis along with the decrease in delta pressure. However, this is speculative as the above study is observational rather than mechanistic. Nevertheless, our study is an in-vivo study showing the effects of alpha blocker on ureteral dynamics in a distal ureteral obstruction model compared with control groups.
Another limitation arose regarding the ability to quantitatively characterize serum and urine alfuzosin levels for all specimens. Despite performing HPLC on two animals with and without oral alfuzosin, some confounding issues arose. Some samples were compromised in transit, which led to rupturing of the specimen containers and contamination, and also there was an issue related to an unknown precipitate that fell out of solution. We sought to reanalyze the samples using mass spectrometry but have to date been unable to obtain sufficiently pure commercially available alfuzosin.
It is difficult if not impossible to define a magnitude or cutoff of observed ureteral dynamic parameters considered as statistically significant that translate to clinical outcomes. We believe that the observed differences in pressure changes and peristalsis may relate to reported decreases in pain and improved stone passage rates with MET. We anticipate larger numbers will result in statistical power sufficient to overcome the variability intrinsic to in-vivo investigations of individual subjects and allow for better characterization of MET mechanisms and investigations of new therapeutic agents.
Conclusions
In the above in-vivo observational porcine study, there was an increase in ureteral pressure and peristaltic rate after distal ureteral obstruction with or without alpha blockade. Observed decreases in alterations of ureteral pressure with peristalsis (delta pressure) and decreased peristalsis rate during alpha blockade in an obstructed porcine model failed to reach statistical significance. Decrease in the rate of peristalsis and delta ureteral pressure may provide effective ureteral dynamics for stone passage. Further investigation and trials are warranted to elucidate the in-vivo physiology of MET.
Footnotes
Acknowledgments
The authors thank the staff of the Animal Research Experimental Surgery Division for their invaluable assistance. Source of funding: Division of Urology, University of Kentucky.
Disclosure Statement
No competing financial interests exist.