
Abstract
Background and Purpose:
Bosniak III and IV renal cysts have low mortality potential, and little is reported regarding the feasibility and safety of managing such tumors by laparoscopy and its comparison with open surgery. We report on the experience with 37 complex renal cysts managed in the era of laparoscopy.
Patients and Methods:
A retrospective analysis of a prospective database from all patients with renal tumors who were operated on at our institution was evaluated after Institutional Review Board approval. The database comprises information for demographic, clinical, imaging, preoperative, intraoperative, histologic, and follow-up data. A comparison among all performed approaches was done for demographic, American Society of Anesthesiologists classification, operative time, estimated blood loss, ischemia time, hospital stay, oncologic and survival rate. The cysts removed by laparoscopic partial nephrectomy were compared with the solid tumors removed by the same approach at the same period.
Results:
The database included 407 patients with renal tumors who were operated on from 2000 to 2009 at our institution. In 36 patients of the total cohort, there were 37 complex renal cysts. No patients with preoperative Bosniak type I or II underwent surgery. Of the cysts, 60% were Bosniak IV, and 86% were confirmed as malignant; 40% were Bosniak III, and 44% were confirmed as malignant. Laparoscopic partial nephrectomy was performed in 67.5%. The tumor size and hospital stay were significantly different in the laparoscopic group. No cyst spillage occurred either by laparoscopy or by the open approach, and no tumor recurrence was found in a mean follow-up of 43.7 months with overall survival of 100%.
Conclusion:
Laparoscopic surgery for complex cysts is safe, feasible, and effective. Nevertheless, regardless of surgical approach, patients with complex renal cysts have excellent overall survival with short-term follow-up.
Introduction
There is no previously reported data evaluating the laparoscopic approach and conventional open surgery for complex renal cysts in a contemporary series when laparoscopy is used more often. 6 We report on the evaluation of 37 complex renal cysts that were managed in the era of laparoscopy.
Patients and Methods
A prospective database that collects data from all patients with renal tumors operated on at our institution since 2000 was retrospectively evaluated, and data from patients operated on because of complex renal cysts was retrieved. The database comprises information with demographic, clinical, imaging, preoperative, intraoperative, histologic, and follow-up data, and it was previously approved by the Institutional Review Board.
Imaging
All patients undergoing the surgery had either a CT scan or MRI or both. The radiologist who works in the division of urology at our institution reviewed the imaging data, and if necessary, the test was repeated at our institution for a more accurate evaluation; then, the image data were used for Bosniak renal cyst classification. 1
Indications of surgical approach
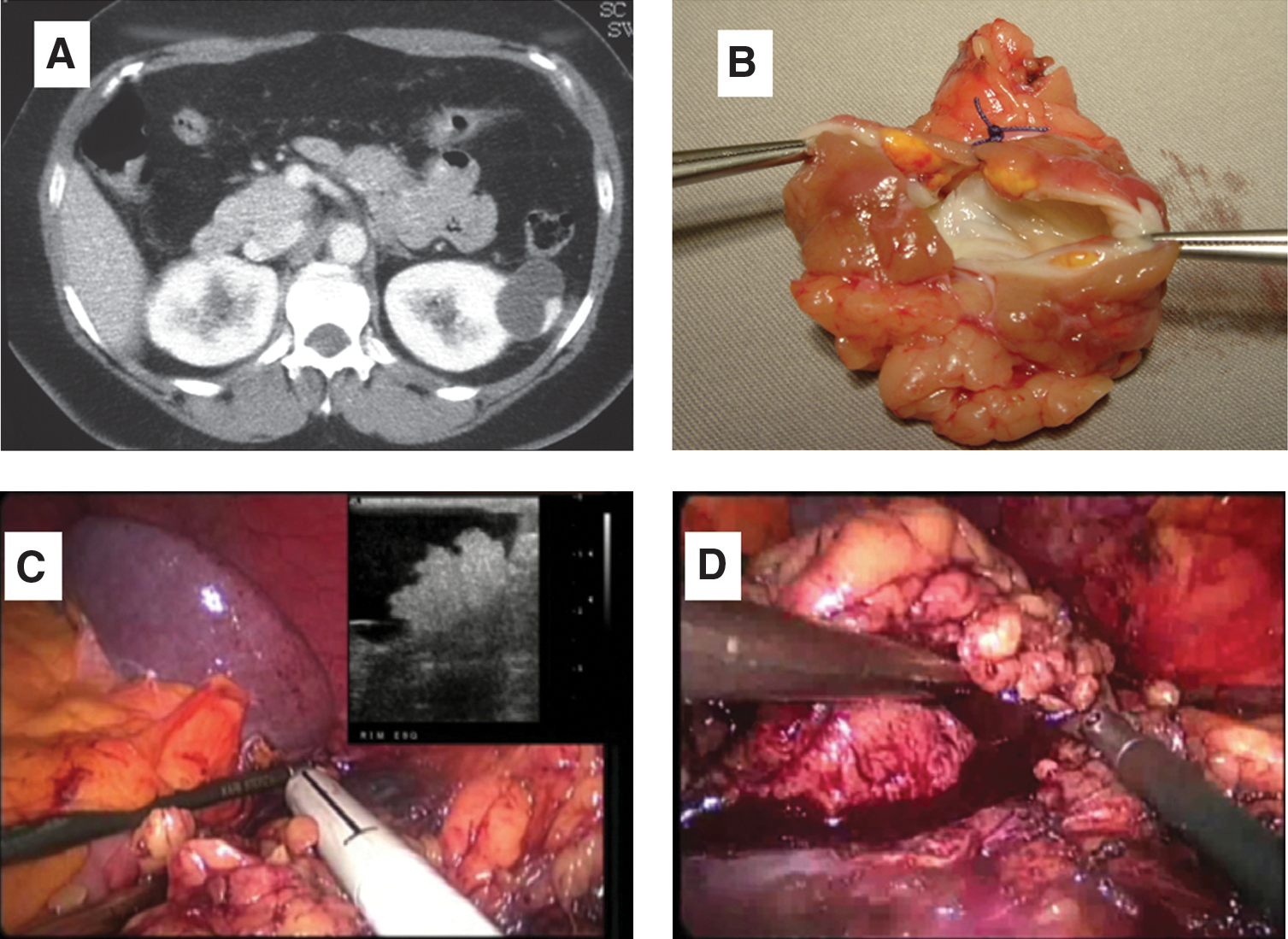
The patients with complex renal cysts were evaluated by the same urologic team in the period, and only patients with Bosniak types III and IV classified after radiologic review were considered candidates for surgical removal. Patients with neither Bosniak type I nor type II/IIF underwent surgery. NSS was favored for most patients, regardless of tumor size or absolute indications, such as solitary kidney, renal insufficiency, and bilateral tumor. Radical nephrectomy was recommended when the renal cyst was invading the renal hilum such that it would not be possible to perform NSS; one patient with von Hippel Lindau disease had a complex lesion, and surgery was performed partial nephrectomy after laparoscopic radical nephrectomy with donor technique (Fig. 1). Open surgery was only considered in patients with absolute contraindications, such as cardiac and lung diseases. Open partial nephrectomy (OPN) was also considered for patients with complex hilar tumors when ischemia time was expected to be longer than 30 minutes.

Surgical techniques
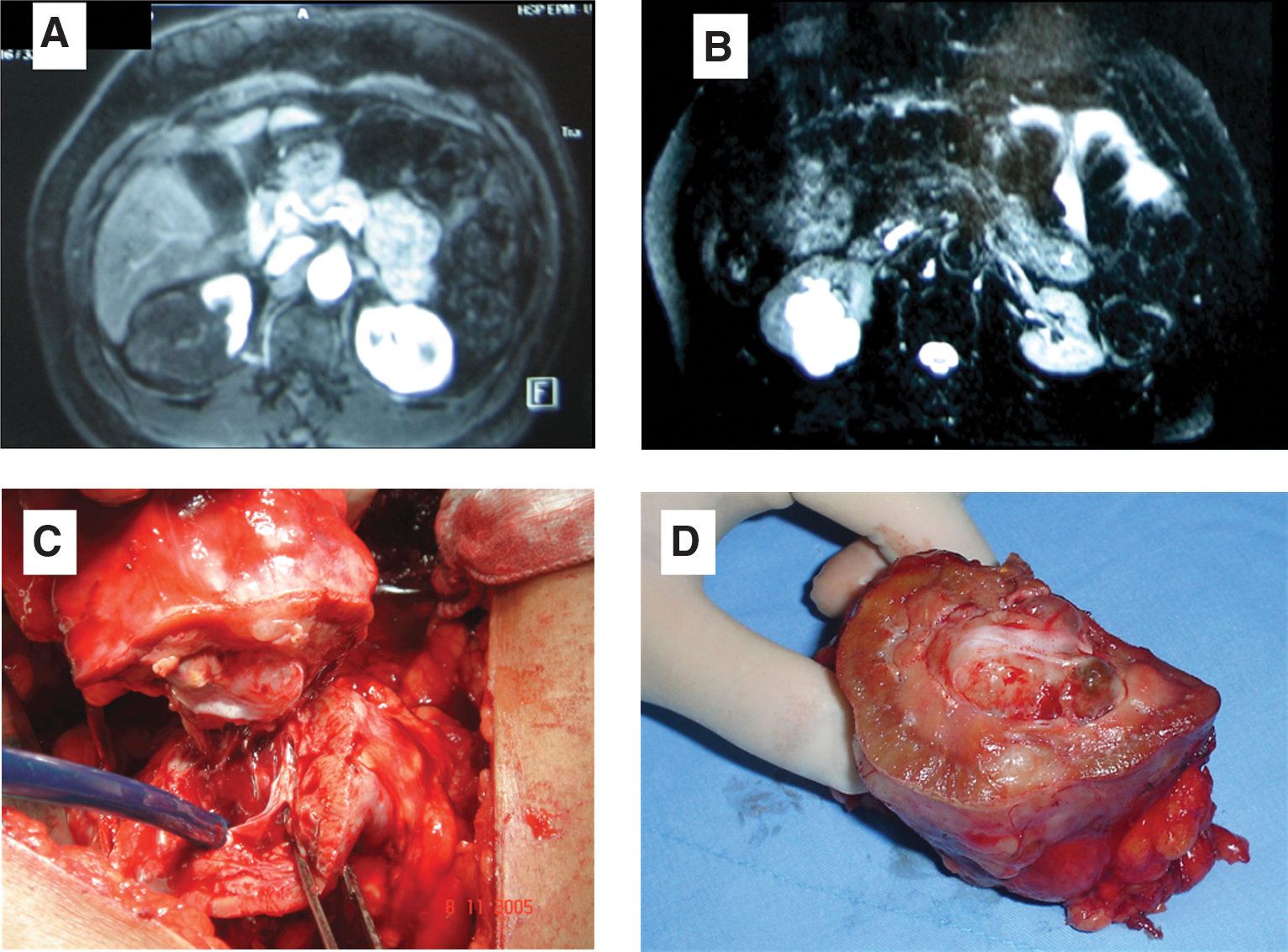
LPN was offered as a first option when possible; four trocars were placed transperitoneally; intraoperative ultrasonography was performed only for precise localization; a bulldog clamp was placed in both artery and vein (warm ischemia); and the tumor was removed with endoshears and intracorporeal suturing performed for hemostasis (Fig. 2). Laparoscopic radical nephrectomy was performed trasnsperitoneally with four trocars in a standard fashion and the specimen removed through a suprapubic incision. OPN was performed retroperitoneally, and cold ischemia was perfomed in all cases (Fig. 3). Open radical nephrectomy was performed retroperitoneally in a standard fashion.
Findings of patients with Bosniak III and IV renal cysts who underwent surgical cyst removal were evaluated. A comparison among all the approaches was performed for demographic, American Society of Anesthesiologists classification, operative time, estimated blood loss, ischemia time, hospital stay, oncologic and survival rate. The cysts removed by LPN were compared with the solid tumors removed by the same approach at the same period.
Statistical analysis was performed for numerical measures using the Student t test, and significance was considered when P < 0.5.
Results
From 2000 to 2009, 407 renal tumors were removed in the division of urology at our institution, and 37 tumors were classified as Bosniak type III and IV in 36 patients; one patient had complex cysts bilaterally. The radiologic analysis of 37 complex cystic lesions according to the Bosniak classification revealed that 15 were type III and 22 were type IV. Twenty-two tumors were on the right side and 15 on the left in 24 men and 12 women. Demographic data are shown in Table 1.
BMI = body mass index; ASA = American Society of Anesthesiologists.
LPN, OPN, laparoscopic radical nephrectomy, and open radical nephrectomy were performed in 67.5%, 10.8%, 10.8%, and 8.1%, respectively. Table 2 shows the perioperative data for all the surgeries performed for complex renal cysts. The tumor size and hospital stay were significantly different in the laparoscopic group. There were no conversions. There was no involvement of surgical margins or violation of the cysts during the procedures. No cyst spillage occurred either by laparoscopy or by the open approach, and no tumor recurrence was found in the mean follow-up of 43.7 months with overall survival of 100% (Table 3).
RCC = renal cell carcinoma; TNM = tumor node metastasis.
Major complications occurred in two cases after LPN and one case after OPN. Two patients after LPN with persistent hematuria after 7 and 10 days underwent selective renal embolization because of arteriovenous fistula. Acute tubular nechrosis with renal insufficiency developed in one patient after OPN, and the patient underwent temporary dialysis. Four patients underwent OPN; one had a 14-cm complex cyst in the lower pole of one kidney, and two patients presented hilar cysts leaning and touching the renal vessels. Another case was discovered incidentally during an episode of acute diverticulitis and operated on at the time of colostomy closure.
Radical nephrectomy was performed in seven (18.9%) cases. The laparoscopic approach was recommended in four cases; one patient, in spite of having a 4-cm cyst, had end-stage renal disease; the other patients had renal cysts with an unfavorable location for NSS. Open radical nephrectomy was performed in only three patients with hilar tumors with average size of 6.2 cm and with clinical contraindication to pneumoperitoneum because of cardiac diseases.
Table 3 shows the histopathologic data. The size of the cysts surgery ranged from 1.5 to 14 cm. Histologic analysis of this group of lesions showed that 64.8% of all complex cysts were malignant lesions; the multicystic renal-cell carcinoma accounted for 91.6% of the tumors, and only two (8.3%) tumors were papillary. Bosniak IV cysts were malignant in 86.2% of the time; the three benign lesions were one oncocytoma with cystic component and two multicystic nephromas. The Bosniak III cysts were benign in 66% of cases, comprising six benign cysts and four multicystic nephromas. We did not observe involvement of surgical margins or rupture of the cysts in our series independent of surgical technique. The malignant lesions were staged clinically and pathologically according to the tumor-node-metastasis system 2002; 50% were pT1a, seven (29%) tumors were pT1b, and five pT2. More than half of the tumors were Fuhrman grade 1, 40% Fuhrman grade 2, and only one (4.1%) tumor had Fuhrman grade 3. No specimen showed vascular embolization. At mean follow-up of 43.7 months (range 2–104 mos), there were no recurrences of the disease regardless of histologic type, staging, and surgical modality used.
The comparison of LPN for complex cysts with solid tumors (Table 4) revealed no significant difference regarding the variables evaluated; the operative time, warm ischemia time, and intraoperative bleeding were slightly higher in the group of complex cysts, but there was no statistical significance.
EBL = estimated blood loss.
Discussion
Despite the limitations from a retrospective study, in the present series, a similar histologic profile was observed as has been reported in other series of complex cysts, but with a higher rate of benign lesions in the group of Bosniak type III cysts. 5,7 Historically, several studies have shown that the complex cysts have low mortality potential, represented mainly by multicystic renal-cell carcinoma, small size, early stage, low-grade malignancy, and papillary tumors 2 –5,7 with characteristics similar to those of incidental renal tumors less than 4 cm. 8 Based on this fact, if one extrapolates the knowledge gained with tumors smaller than 4 cm, cystic tumors have a similar biologic behavior, and patients may have disease-free survival at 5 years of 90% to 100% when treated with NSS. 9 –11
Little is known about the natural history of complex cysts and Corica and colleagues 3 suggested NSS as the ideal therapeutic modality in the management of complex renal cysts. There was no tumor recurrence independent of tumor size, stage, and number of cysts or disease-related mortality survival and tumor recurrence in 24 cases of cystic renal-cell carcinoma that was surgically removed in a mean follow-up of 77.6 months, suggesting that preserving as much functioning renal tissue offers benefits to the patient without jeopardizing the cancer treatment. Sharing the same opinion, the present series elected partial nephrectomy as the modality of choice in the management of complex renal cysts, and only seven cases of complex renal cysts were candidates for radical surgery because of their large size, anatomic complexity, and lack of need for renal preservation.
The approach of choice for renal tumors in our institution is the laparoscopic approach; 30 laparoscopic procedures (25 partial nephrectomies and 5 radical nephrectomies) were performed. The open approach was selected for complex cases; the selection criteria are based on size and location of lesions, and candidates for open surgery were only those who had large lesions, very close to the renal vessels, that would be difficult to remove by laparoscopy and patients with absolute contraindication to pneumoperitoneum.
Only 10.8% (4) of our patients underwent OPN; therefore, 25 (67.5%) patients were candidates for LPN in our series, and no conversions were observed at the time of surgery, with no significant differences when compared with other historical series of partial nephrectomy for solid tumors of the kidney.
The potential violations of the cysts during surgery did not occur in the present study regardless of surgical approach, and at a mean follow-up of 52.2 months, there were no recurrences of the disease. In the series by Spaliviero and coworkers, 5 33 patients with complex cysts (Bosniak III and IV) underwent the laparoscopic approach, and there was no violation or tumor involvement of tumor margins; only one case of tumor recurrence occurred in a 2-cm Bosniak III cyst with Fuhrman grade III. Limb and associates 12 performed a laparoscopic procedure in 57 complex cysts, called indeterminate cysts; they aspirated the fluid and biopsied the cystic wall at operating time, which revealed that 20% were malignant. No recurrences were observed in five patients who underwent partial nephrectomy and six who underwent radical nephrectomy in a mean follow-up of 40 months.
At present, renal ablation therapy, such as cryoablation and radiofrequency ablation, would be a possibility for the management of a complex cystic lesion, but the likelihood of tumor spillage during the probe placement and the unknown best target to place the probe into the cyst made this approach interesting but still not used in our institution.
Conclusion
Regardless of the low mortality potential, complex renal cysts need a precise and complete surgical removal with maximum renal parenchyma preservation, which can be offered in a less invasive approach, such as LPN, without violating oncologic principles. Laparoscopic surgery for complex cysts is safe, feasible, and effective. Nevertheless, regardless of surgical approach, patients with complex renal cysts have excellent overall survival.
Footnotes
Disclosure Statement
No competing financial interests exist.