
Abstract
Introduction:
Upper tract urothelial carcinoma (UT-UC) is an uncommon disease with pronounced difference in 5-year survival for noninvasive (96%) versus invasive (17%) disease. High survival rate of early disease questioned the accepted norm of using radical nephroureterectomy (RNU) for all stages. This review assesses effectiveness of endoscopic management for UT-UC.
Methods:
A review of 131 UT-UC patients seen between January 1999 and October 2009 was performed. Demographic, clinicopathologic, and outcomes data were collected and compared between patients initially managed with RNU versus those initially managed with nephron-sparing surgery (NSS). The chi-square or Fisher's exact tests for categorical variables and the Wilcoxon–Mann–Whitney test for continuous variables were used. Clinical and pathologic stages of RNU patients were evaluated with chi-square testing, whereas difference in length of stay was detected using linear regression. Recurrence rates were compared using multivariate Cox regression.
Results:
The two arms had similar distributions of age, sex, frequency of medical comorbidities, American Society of Anesthesiologists (ASA), and Charlson scores. Mean-adjusted length of stay was 2.1 (95% confidence interval [1.6, 2.5]) and 5.5 days (95% confidence interval [5.3, 6.4]) for the NSS and RNU groups, respectively (p < 0.001). Comparison of clinical and pathologic stages of RNU patients showed a difference (p < 0.001), with under-staging noted in 32%. Men (Hazards Ratio = 2.9 [1.5–5.5], p = 0.001) and NSS patients (hazards ratio [HR] = 3.5 [1.7–7.3], p < 0.001) had threefold increased recurrence risk.
Conclusion:
NSS offered shorter hospital stay but had increased risk of recurrence. Therefore, extreme care should be made to rule out occult invasive tumors preoperatively. Patients being managed endoscopically must be informed of the necessity for close follow-up.
Introduction
Materials and Methods
After obtaining Institutional Review Board (IRB) approval, data were abstracted for UT-UC patients managed at our institution from January 1999 to October 2009. Candidates were identified using International Classification of Diseases (ICD) codes corresponding to neoplasms of the renal pelvis, calices, and ureter corroborated by an imaging study demonstrating the lesions, and urine cytology or tissue diagnosis confirming urothelial origin. Patients found to have neoplasms that were nonurothelial in origin were excluded (n = 5), resulting in a final cohort of 131 patients. Of these, 11 did not undergo either RNU or NSS because of personal choice (n = 2), extensive comorbidities (n = 5), or metastatic disease (n = 4). NSS was defined as percutaneous and/or ureteroscopic resection and/or fulguration, or basketing of UT-UC. Clinico-pathologic characteristics were compared between patients initially managed with RNU versus those initially managed with NSS using chi-square or Fisher's exact tests for categorical variables and Wilcoxon–Mann–Whitney test for continuous variables. The chi-square test was also employed to detect if a difference between the clinical and pathologic stages of patients under the RNU cohort existed. Length of stay (LOS) was compared using linear regression, adjusting for age, sex, race, stage, American Society of Anesthesiologists (ASA) score, Charlson comorbidity index score, and Clavien complication severity score. Because of non-normal distribution, LOS was log-transformed before analysis and mean-adjusted values were calculated for each subgroup; back-transformation was then done for ease of interpretation. Follow-up was calculated using reverse Kaplan–Meier method, and cumulative incidence functions were used to assess survival outcomes. Cox modeling of recurrence began by univariate analysis of candidate predictors using logrank test. Predictors, with a p-value < 0.2 were included in multivariate proportional hazards model. Analyses were performed using STATA v.11 with an alpha of 0.05.
Results
The baseline characteristics for the entire population and the two subgroups were summarized in Table 1. The most common presenting symptoms were gross hematuria (56%) and flank pain (23%). Synchronous bilateral presentation was seen in 5% of cases, whereas only a single patient (0.8%) had bilateral metachronous presentation. Eleven patients presented with a solitary kidney. Of the unilateral cases, 48% were on the left and 52% were on the right. Tumors were identified on imaging in all patients: 76% with computed tomography scan and retrograde pyelography in 57%. Ureteroscopy assisted in the work-up of 55%. Preoperatively, diagnosis was confirmed with cytology in 65%, biopsy in 30%, and visual assessment in 29%. A mean number of 2.6 ± 1.1 biopsy cores were needed for a preoperative diagnosis and grading to be made. The majority of cases were managed with RNU (74%): open approach in 54% and laparoscopic in 46%. NSS was used to manage 16% of cases (see Table 2). Patients initially managed with NSS who experienced recurrence underwent further surgery, ranging in number from 1 to 10 with a mean of three procedures. The rest were diagnosed as stage IV or synchronous bilateral disease and either underwent systemic chemotherapy alone or opted for palliative care only. Eight percent were subjected to local adjuvant therapy for their UT-UC, with a single patient receiving prophylactic treatment 3 weeks postoperatively. The agents were administered through a nephrostomy tube (3%), or intravesically with an internal ureteral (4%), or open-ended ureteral stent (1%) in place.
ASA = American Society of Anesthesiologists; BMI = body mass index; CAD = coronary artery disease; DM = diabetes mellitus; HTN = hypertension; NSS = nephron-sparing surgery; RNU = radical nephroureterectomy; SD = standard deviation; UT-UC = upper tract urothelial carcinoma; UT = upper tract; TC = transitional cell.
BCG = Bacillus Calmette-Guerin.
The overall mean postoperative LOS was 5.8 ± 4.4 days. Mean length of follow-up was 17.9 months (13.2, 24.6). The mean-adjusted LOS was 2.1 (95% confidence interval [1.6, 2.5]) and 5.5 days (95% confidence interval [5.3, 6.4]) for the NSS and RNU arms, respectively (p < 0.001) (see Table 3). Only 28% of the population (n = 37) remained disease-free, whereas the overall recurrence rate was 63% on the latest date of follow-up. Recurrence was defined as any recurrent disease in the bladder, ipsilateral UT, bladder and UT simultaneously, or distant metastases. The cumulative incidences for recurrence in the RNU versus the NSS arms were plotted in Figure 1. Comparison of clinical and pathologic stages of RNU patients showed a significant difference (p < 0.001), with under-staging noted in 32% (Table 4). After univariate analysis, predictors included in the multivariate Cox regression were sex, type of initial intervention, pathologic stage, and tumor size, wherein sex (hazards ratio [HR] = 2.9 [1.5–5.5], p = 0.001) and initial surgical intervention (HR = 3.5 [1.7–7.3], p-value < 0.001) proved to be positive predictors of recurrence (Tables 5 and 6). Kaplan–Meier recurrence-free survival curves were plotted in Figure 2.
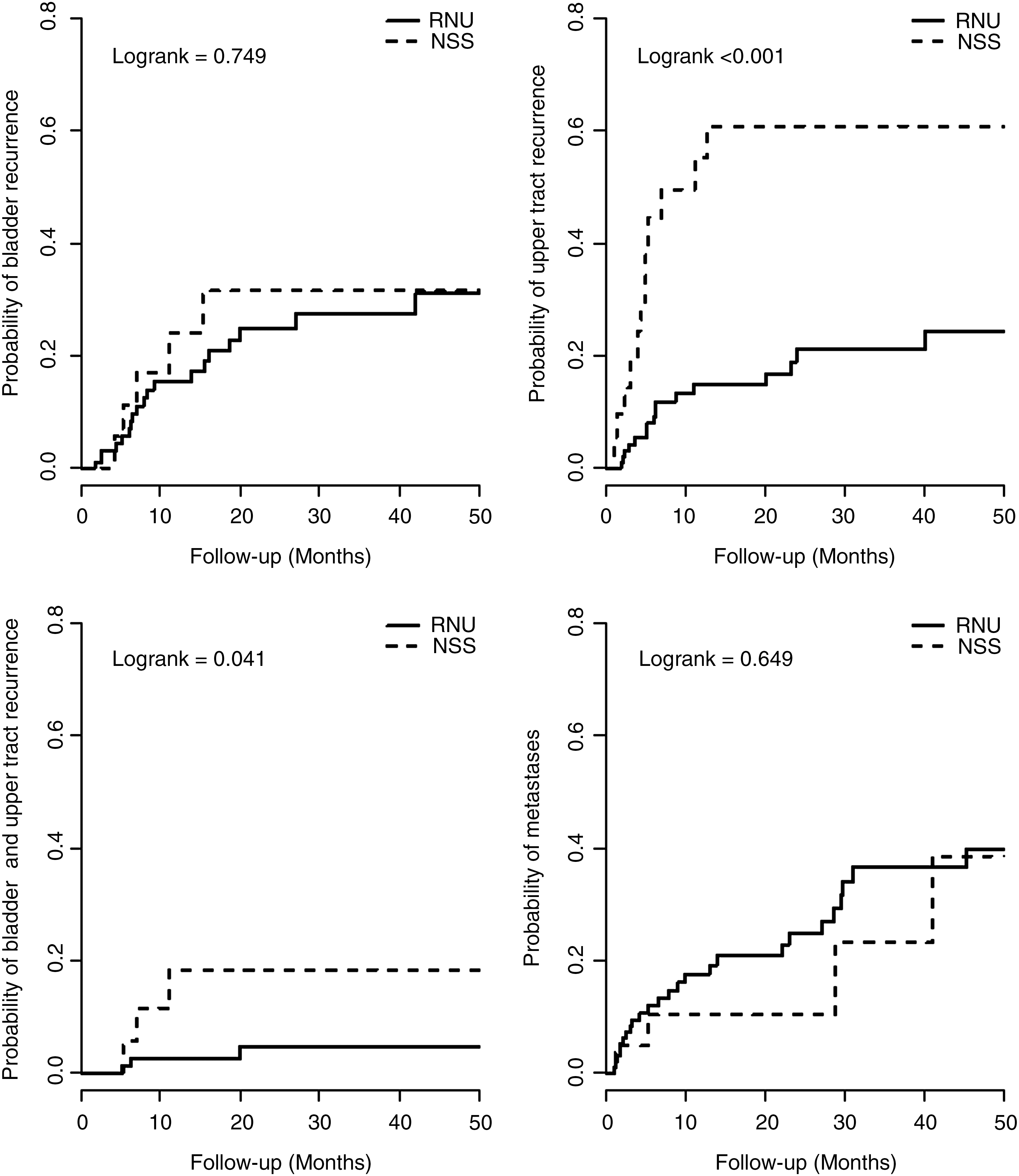
Cumulative incidence of recurrence in the RNU versus NSS cohorts, broken down into (top left) bladder recurrence, (top right) UT recurrence, (bottom left) simultaneous bladder and UT recurrence, and (bottom right) distant metastases. NSS = nephron-sparing surgery; RNU = radical nephroureterectomy; UT = upper tract.
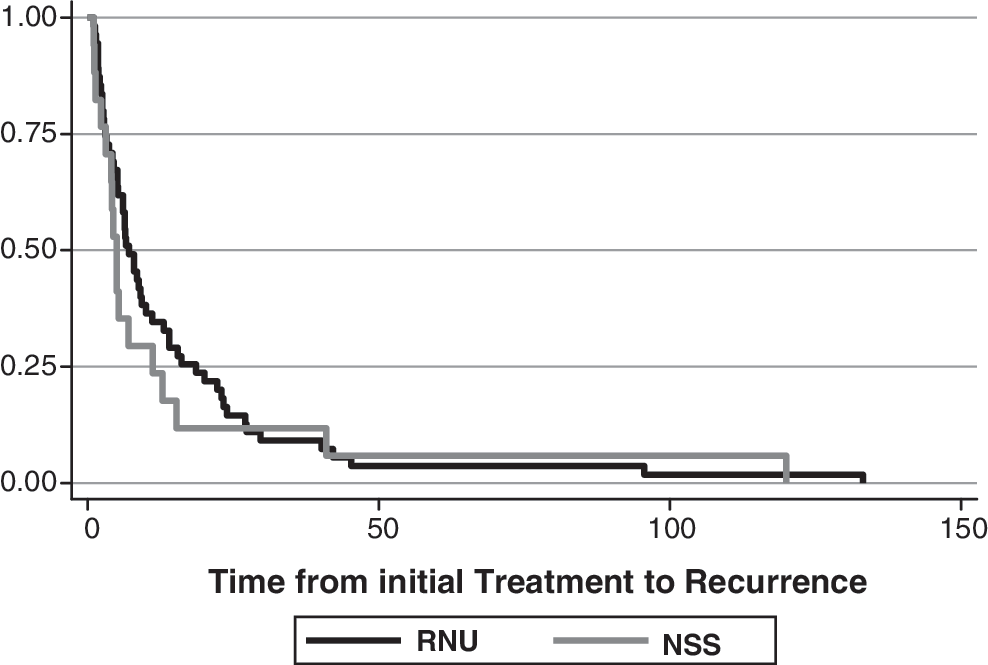
Recurrence-free survival rate: NSS versus RNU.
RR = risk ratio.
CI = confidence interval; HR = hazards ratio.
Discussion
Although UT-UC is relatively uncommon, interest in the disease has remained because of increasing incidence 1,17 and the pronounced difference in 5-year survival for noninvasive (96%) versus invasive (17%) disease. Other issues associated with UT-UC, such as its preponderance to occur in older patients or for synchronous presentation, resulted in exploring endoscopy to replace RNU.
Demographic parameters of our UT-UC patients mirrored characteristics noted in earlier publications. A mean age of 70 years confirmed that this disease is commonly diagnosed in elderly patients. 1,2 The preponderance of UT-UC for men 2,3 was confirmed by this study's 2:1 male-to-female ratio. More importantly, sex's role as a predictor of recurrence has not been previously noted to our knowledge. Aside from more men being found to have UT-UC, men were also almost thrice as likely to develop recurrence. Racial distribution and presenting symptomatology that we noted were similar to earlier findings. 2,3,13,18 Previous studies have estimated that 52% of UT-UC occurred in the renal pelvis and 25% in the lower ureter. 2,19 We found approximately the same distribution, with 60% of the tumors in our cohort located in the renal pelvis and 22% located in the distal ureter.
Part of the impetus for performing NSS in patients with UT-UC is the tendency for these patients to present with synchronous or metachronous bilateral lesions. This has been reported to occur in up to 72%. 3 In our population, we found synchronous bilateral lesions in <5%. Other indications for NSS in the current study included concomitant renal disease in 15% and a solitary kidney in 8% of patients. In addition, significant medical comorbidities are often cited as a reason for performing NSS. High survival rate in early stage disease led investigators to consider percutaneous and ureteroscopic approaches for patients with early stage tumors and significant comorbidities precluding RNU. Confounding medical problems can prevent many patients from undergoing taxing surgical procedures, such as open RNU. There were no differences in the incidence of medical comorbidities, ASA level, and Charlson index in patients of either arm of our series. However, there were increased complications in patients who underwent RNU compared with NSS (30% vs. 14%, p = 0.137). Although this finding did not reach statistical significance, it is clinically relevant. Patients with significant comorbidities may in fact benefit from less invasive approaches. With the increasing use of laparoscopy to perform RNU, this difference in complications may change.
Tumor diameter and histologic grade distribution between the two arms varied significantly, with more grade 1 disease and smaller tumors receiving NSS. This finding is expected as the larger a tumor becomes, the more difficult it is to treat endoscopically. In addition, histologic grade has been shown to affect cancer-specific survival rate by multiple studies, with chances of survival in well-differentiated UT-UC almost double that of poorly differentiated cancers. 4,5,20,21 Grade is felt to be a surrogate for tumor stage as it is often difficult to obtain muscle in biopsy specimens of the UT. Therefore, patients with higher grade tumors are often felt to have clinically higher stage disease. One limitation of our study was the relatively high incidence of visual diagnosis of the initial tumor. Previous studies suggest that visual assessment alone was inaccurate in 30% of the cases. 22
There was a trend toward increased clinical stage in the RNU cohort in our study. Traditionally, it was assumed that these patients benefit from RNU compared with NSS. Tumor diameter was found to affect metastasis-free and disease-free survival, 23 whereas tumor architecture was noted to be an independent predictor of recurrence and disease-specific survival rate. 24 Tumors with sessile architecture were found to be of higher grade, more advance stage, and more likely to have lymphovascular invasion. 23,24 In this series, neither tumor grade nor size were significant predictors of recurrence. Most of the previous studies that compared NSS to RNU had demonstrated similar recurrence rates, with ureteroscopy at 30% to 71%, and 11% to 33% for percutaneous approach 14 –16 ; rates for RNU were 23% to 62%. 25 –28 Our overall recurrence rate was comparable at 31%. However, we found significantly greater recurrence in patients who underwent NSS. In particular, patients undergoing NSS were at significantly greater risk of recurring in their UT. The risk of bladder recurrence was similar between the two. When bladder and UT recurrences were combined for overall recurrence rate, patients who were treated with NSS were still at a disadvantage and having three times the risk of experiencing recurrence (HR = 3.5 [1.7–7.3], p-value < 0.001). This was likely because of elimination of more anatomic sites of possible recurrence by RNU, since majority (48%) of the recurrent tumors managed with NSS returned to their original sites of growth. 29 Incomplete eradication of primary tumor or intraoperative seeding may also contribute to higher recurrence rates. The significance of this is that patients who undergo NSS must be made aware of the need for lifelong surveillance and repeat procedures when counseled about their treatment options. It is unclear if the cumulative perioperative risk of these procedures is greater than that for RNU. In our study, 16 of the 22 patients treated with NSS underwent multiple procedures because of recurrent disease and 9 went on to undergo RNU. Five of the 10 NSS patients who experienced UT recurrence progressed to metastatic disease, 1 of whom died because of surgical complications. At most recent follow-up, only 8% of the patients treated ureteroscopically and 44% of patients treated with percutaneous approach were disease-free. The ideal surveillance regimen for these patients is not known at this time, but it is clear from our data that they require regular surveillance likely for an indefinite period of time.
Metastasis rate has been reported to be 17% among patients managed with percutaneous resection, 30 which was slightly higher than the 8% to 13% rate in a series of patients who underwent RNU. 28 In our series, there was no significant difference in the risk for metastasis, despite the previously mentioned increased risk of recurrence in patients who underwent NSS; the RNU and NSS arms had 36% and 23% rates at 3 years postintervention (logrank, p = 0.65). For our entire study population, the overall survival rate was noted to be 95%, likely a consequence of most cases (55%) being diagnosed in the early stages. Moreover, most of the NSS patients who experienced recurrence eventually underwent RNU, which could explain the improved figures compared with earlier publications. 31,32 No percutaneous tract recurrence was noted in our study, as was previously suggested by others. 21 Disease-specific survival for locally confined UT-UC has been reported to be 95% compared with 16% for metastatic disease. 1 Disease-free survival rates ranged from 35% to 86% for tumors treated endoscopically. 30 –33 RNU approach had so far offered disease-free survival rates between 62% and 95%. 26,28,31,32,34,35
As expected, one of the advantages of NSS over RNU was the shorter postoperative hospital stay. This had been noted in almost all surgical treatments that veer toward a less invasive treatment modality. 26,28,30,36 This advantage may become less significant as more RNU are performed laparoscopically.
Most publications on adjunctive therapy for UT-UC have not demonstrated a clinical benefit from treatment with Bacillus Calmette-Guerin (BCG), 10,16 immunotherapy, 10,16 or other chemotherapeutic 11,36 –39 agents. 11,35 –38 However, several publications claimed recurrence-free rates between 43% 40 and 83% 25 with the use of BCG, 25,41 –44 but the complication of systemic BCG infection has remained a major concern. Although the use of adjuvant radiotherapy has been found to have recurrence rate of 50% and overall disease-free 5-year survival of 30%, 45 its use at our institution for recurrent and end-stage UT-UC comprised only a handful of cases and remained mostly experimental. Adjuvant local and systemic chemotherapy given to our patients did not significantly affect the risk for recurrence (logrank p = 0.4). It was, however, noteworthy that a higher percentage of RNU patients were given adjuvant systemic chemotherapy (p = 0.008).
Under-staging was observed in 32% of stage I-II UT-UC after RNU. This could indicate that a significant number of stage I-II patients in the NSS cohort were under-staged as well, and may explain the higher UT recurrence in the NSS arm (Fig. 2). Because there would be no way to determine pathologic and thus under-staging in patients managed with NSS, it may be prudent to consider UT irrigation with a chemotherapeutic agent 24 hours postoperatively to address possible seeding; this adjunctive treatment has been shown to decrease recurrence in bladder UC managed with transurethral resection. 46 Re-staging transurethral resection had likewise been shown to improve recurrence-free survival 47 by minimizing chances of residual tumors. Conducting second-look endoscopy 2 to 6 weeks after initial NSS should be contemplated. Other methods that have been used to improve detection of residual and/or recurrent bladder tumors could also be applied to NSS for the UT, such as narrow band imaging 48 –51 or photodynamic endoscopy. 52,53
With increasing incidence of UT-UC 1 and other diseases that cause chronic renal insufficiency, use of NSS for this disease is here to stay. Although this approach offers undeniable benefits, there is an increased risk for recurrence related to its use. Thus, NSS should be undertaken with caution and great care must be made to rule out occult invasive tumors. Moreover, uniform protocols for administration of adjunctive treatment should be developed to help decrease the risk of recurrence after NSS.
Conclusions
Given that UT-UC is rare, this study was limited by a relatively small sample size. Limited number of events (i.e., recurrence, metastases, and death) precluded adequate comparison of outcomes parameters (recurrence, metastases, and survival rate) between the cohorts. Collaborative, multicenter research would be of great benefit in producing an adequately powered study that is necessary to meaningfully determine if one treatment arm would be better than the other and offer improved prognosis for UT-UC. Variabilities in histologic grading nomenclature, surgeons' skills, and treatment preferences likewise hampered this study, as would be expected from most retrospective research. A randomized design would greatly contribute in producing robust results and recommendations.
Footnotes
Disclosure Statement
Dr. Eliza M. Raymundo is a recipient of the Industry-sponsored (Gyrus ACMI Corp/Olympus) Endourology fellowship.