
Abstract
Introduction:
The da Vinci® surgical platform is becoming increasingly available and utilized. Due to the lack of haptic feedback, visual cues are necessary to estimate grip forces and tissue tensions during surgery. We directly measured the grip forces of robotic EndoWrist ® instruments using the three available da Vinci robotic surgical platforms.
Methods:
Robotic instruments were tested in the da Vinci S, Si, and Standard systems. A load cell was placed in a housing unit that allowed for measurement of the grip forces applied by the tip of each robotic instrument. Each instrument was tested six times, and all data were analyzed using Student's t-tests or analysis of variance when appropriate.
Results:
Slight differences in grip force were seen when the instrument was tested through 2 degrees of freedom at the tip (p = 0.02, analysis of variance) and when comparing a new instrument to an older instrument (p = 0.001 at the neutral position). There was no statistical difference in grip force between the left and right robotic arms. There was a broad range of grip forces between the various robotic instruments. The lowest grip force was registered in the double fenestrated grasper (2.26 ± 0.15 N), whereas the highest was seen in the Hem-o-lok® clip applier (39.92 ± 0.89 N). In comparison to the S and Si, the Standard platform appeared to have significantly higher grip forces.
Conclusion:
Different grip forces were observed among the various robotic instruments commonly used during urologic surgery and between the Standard and the S and Si platforms.
Introduction
Although there are numerous studies examining robotic surgical outcomes and novel uses for the robot, very little is known about the inner workings of the robot. Few surgeons question the capabilities or limitations of the machine. We sought to help elucidate one of the most basic elements of the robot: the grip force of the robotic instruments. Using a load cell testing device, we investigated the specific grip forces (closing pressures) exerted by the tips of various EndoWrist ® robotic instruments across the three commercially available da Vinci Surgical platforms.
Methods
A Standard da Vinci Robotic platform in an accredited robotic training center was used for the initial experiments. A 2.2-mm button style compression load cell transducer (Interface Advanced Force Measurement, Scottsdale, AZ) was placed in a specially designed aluminum housing unit that allowed for the measurement of grip force for fine tipped instruments (Fig. 1). All instrument tips were placed in the middle of the housing unit with the tip extending to the shoulder of the shelved out platform (Fig. 2). Bulldog clamps were used to determine the force conversion factor inherent in the load cell housing unit by measuring the forces directly on the load cell and with the load cell within the housing unit.
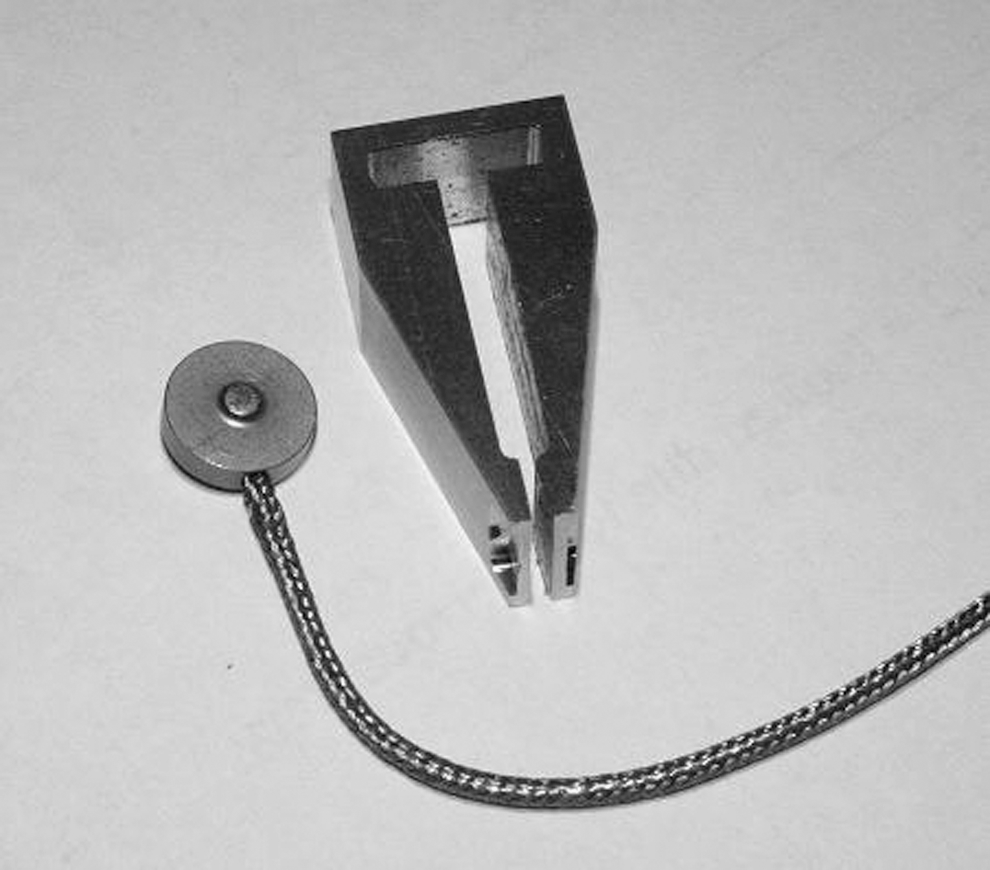
Load cell and housing unit. The load cell (left) consists of a small circular disc connected by a wire to the interface® 9820 strain gage transducer (not pictured). The housing unit (right) holds the load cell in its long interior chamber for the testing of all robotic instruments.
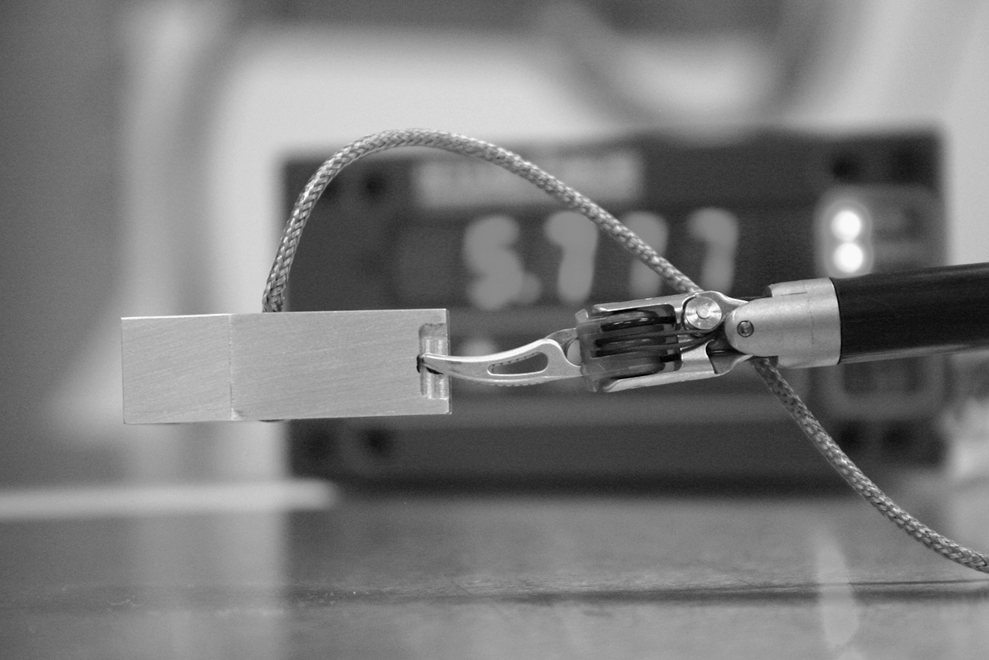
Experimental apparatus. A da Vinci® Maryland Bipolar Forceps grasps the housing unit, which holds the load cell in place. All instruments were tested by gripping the middle of the housing unit with the tips fit tightly against the shoulder of the shelved out platform as seen above. The interface 9820 strain gage transducer can be seen in the background.
Initially, the differences in grip force at various wrist positions, including the neutral position, positive and negative major deflection (deflection at the proximal wrist joint) (Fig. 3), and left and right minor deflection (deflection at the distal wrist joint) (Fig. 4) were measured in a new (previously unopened) Maryland bipolar extended training instrument (8 mm) and an ∼3-year-old large needle driver (8 mm, extended use training instrument). Once the wrist position was achieved, the housing unit was firmly grasped and movements of the instruments were deactivated by removing the head from the console visor. The new 8-mm Maryland bipolar grasper was also used to evaluated the left versus the right robotic arm, and was compared with an older (∼2 years old) training instrument. All instrument trials were repeated six times at each EndoWrist position. Open surgical instruments were also tested in a similar manner. The Aesculap Instruments (Long Kelly Curved, Product #: BH165R, Kelly Curved (Hemostat) Product #: BH135R, Baby-Mosquito Product #: BH115R, and Long Allis Product #: EA097R) were placed on the load cell housing and locked at one click. All instrument trials were repeated six times.
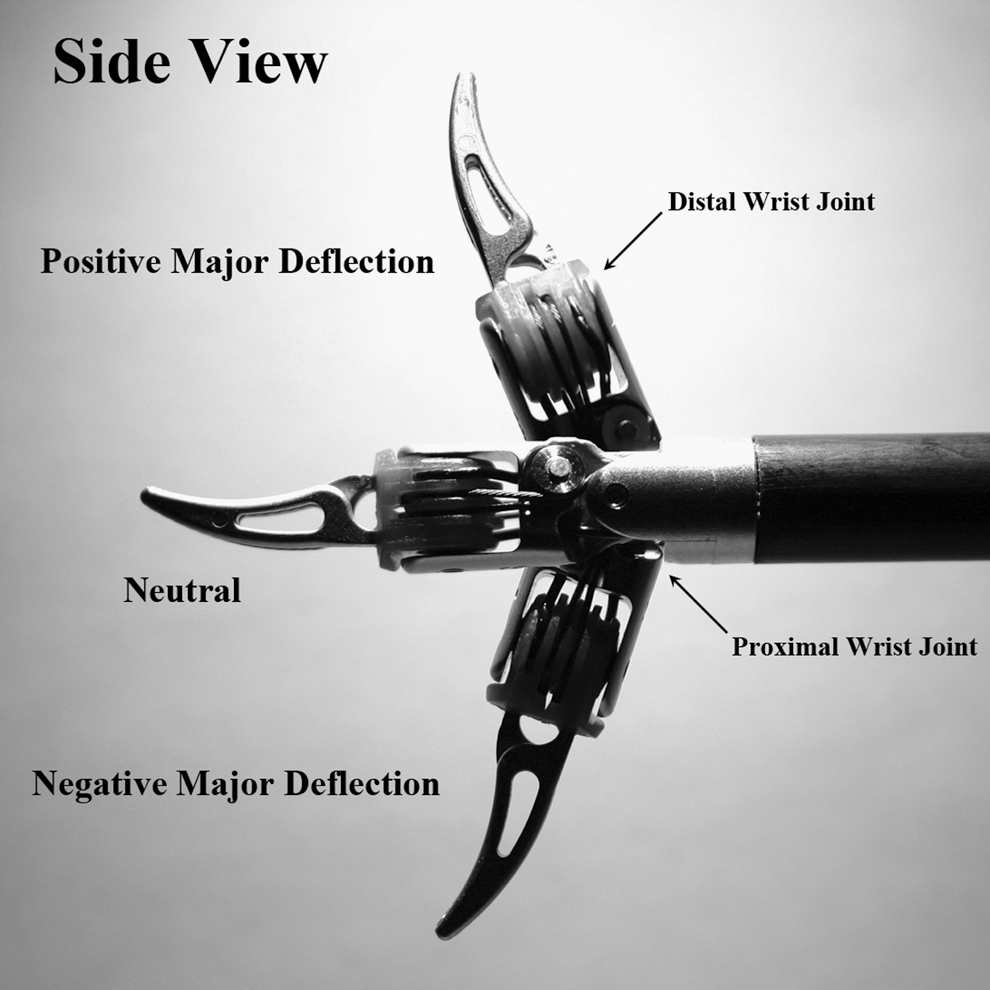
Side view of a da Vinci Maryland bipolar forceps. The neutral position is defined as being parallel to the instrument arm, with no net displacement of the proximal or distal wrist joint. The positive major deflection is defined as a maximum upward or positive displacement from the neutral position via movement of the proximal wrist joint only. The negative major deflection is defined as a maximum downward or negative displacement from the neutral position via movement of the proximal wrist joint only.
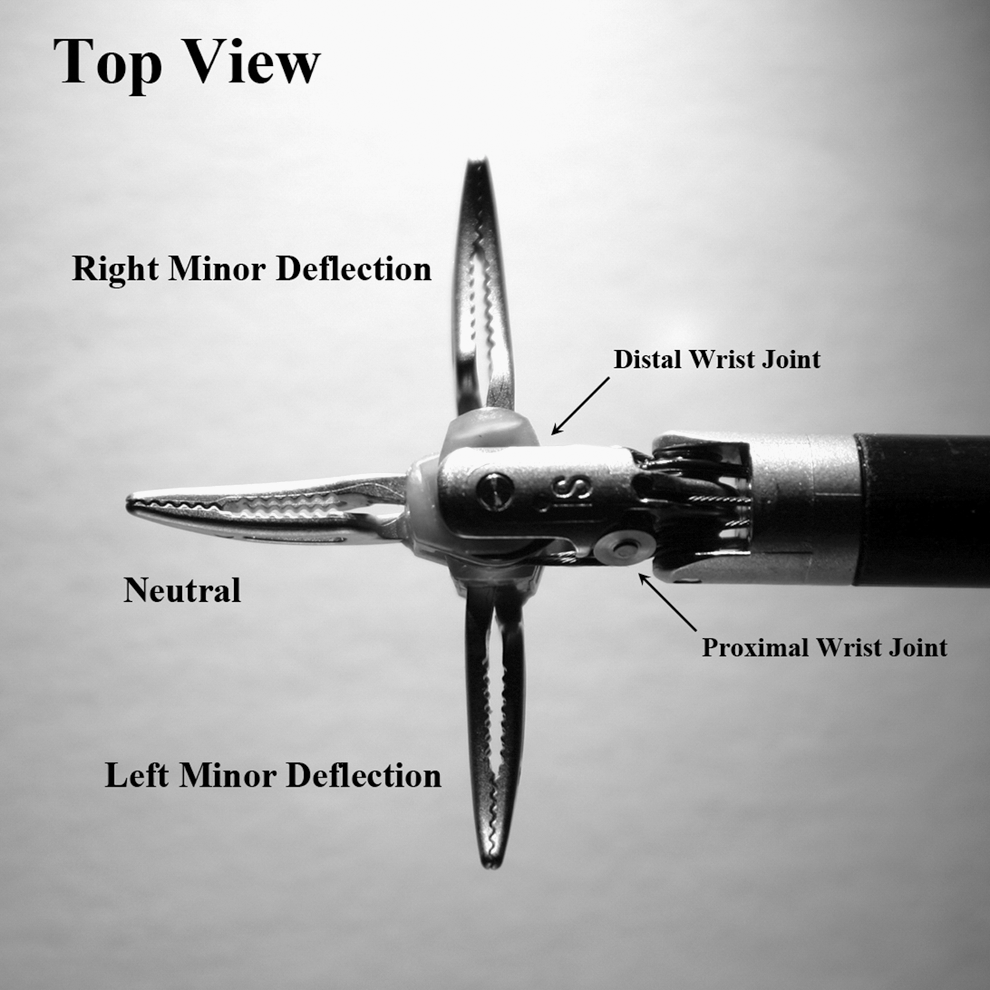
Top view of a da Vinci Maryland bipolar forceps. The neutral position is defined as being parallel to the instrument arm, with no net displacement via the proximal or distal wrist joint. The right minor deflection is defined as a maximum rightward—in this view upward—displacement from the neutral position via movement of the distal wrist joint only. The negative major deflection is defined as a maximum leftward—in this view downward—displacement from the neutral position via movement of the distal wrist joint only.
Leak point pressure was determined using a similar setup described by Lee et al. 5 A freshly harvested porcine renal artery was occluded by the tips of an ∼2-year-old 8-mm Bowel grasper using the Standard robotic platform. Methylene blue dye mixed with saline was then infused through the artery at a constant rate of 30 mL/minute using an infusion pump. The maximum pressure in mm Hg required for leakage distal to the Bowel grasper was recorded using a Cole-Parmer (Vernon Hills, IL) digital pressure measuring device.
A Standard, S, and Si da Vinci surgical systems were all available for testing at the same time and place during an American Urologic Association (AUA) robotic educational course at the University of California, Irvine. At this time, instruments commonly used during urologic surgery were tested across all platforms. All instruments were tested in the neutral position and each test was taken in triplicate. When comparing the S and the Si, the same instrument was used for each patient side cart and compared with the same type of instrument in the Standard system.
Statistical analysis was performed using one-way analysis of variance and unpaired Student's t-tests where appropriate. A p-value of <0.05 was considered significant. All statistical analysis was performed using STATA software, version 9.0 (Stata Corp, College Station, TX).
Results
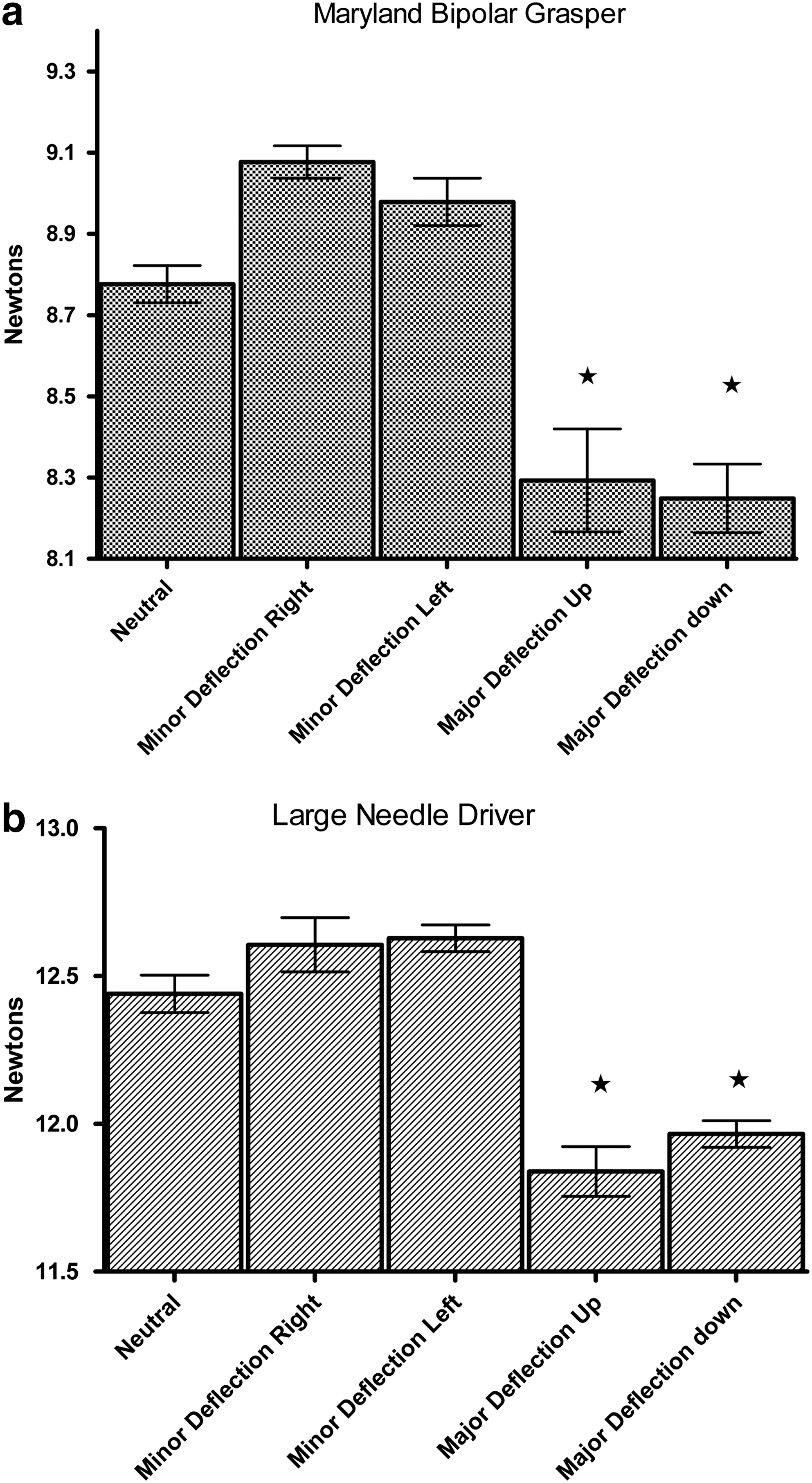
A new Maryland bipolar grasper and large needle driver were found to have significant differences in grip forces at the neutral, major defection (positive and negative), and minor deflection (left or right) positions (Maryland p = 0.02, large needle driver p < 0.001, analysis of variance). Grip forces at the neutral position and minor deflections were not significantly different in both the Maryland grasper (neutral vs. left [p = 0.507] neutral vs. right [p = 0.147] right vs. left [p = 0.937]) and needle driver (neutral vs. left [p = 0.357] neutral vs. right [p = 0.484] right vs. left [p = 0.999]). A significant difference did exist between the major deflections compared with the neutral and minor deflections in both the Maryland grasper and large needle driver (Fig. 5a, b). The total difference between the neutral position and average major deflections was 6.72% of the neutral position in the Maryland grasper and 4.3% in the large needle driver. These results were also confirmed with the Maryland grasper on the left arm (data not shown).
The right and the left robotic arms were compared using the same instrument and found to be equivalent at each position (Table 1). When compared with an older training instrument, the newer instrument had a significantly higher grip force at each position (Table 1).
A new Maryland grasper was tested on the left or right robotic arms for grip forces at each position. A new Maryland grasper was tested versus an ∼2-year-old Maryland grasper. (Since earlier tests revealed no differences between neutral and minor deflection, these results were omitted.) All p-values were determined using unpaired Student's t-tests.
N = newtons; SD = standard deviation.
Table 2 is a summary of all of the available training instruments tested on the Standard, S, and Si platform. Grip forces ranged from lowest (Double Fenestrated grasper 2.26 ± 0.15 N) to highest (Hem-o-lok® clip applier 39.92 ± 0.89 N). There were no significant differences seen when the same instrument was tested on the S and the Si surgical platforms; however, the Standard platform had a statistically significant higher grip force in most instruments when compared with the S and the Si. (Fig. 6).
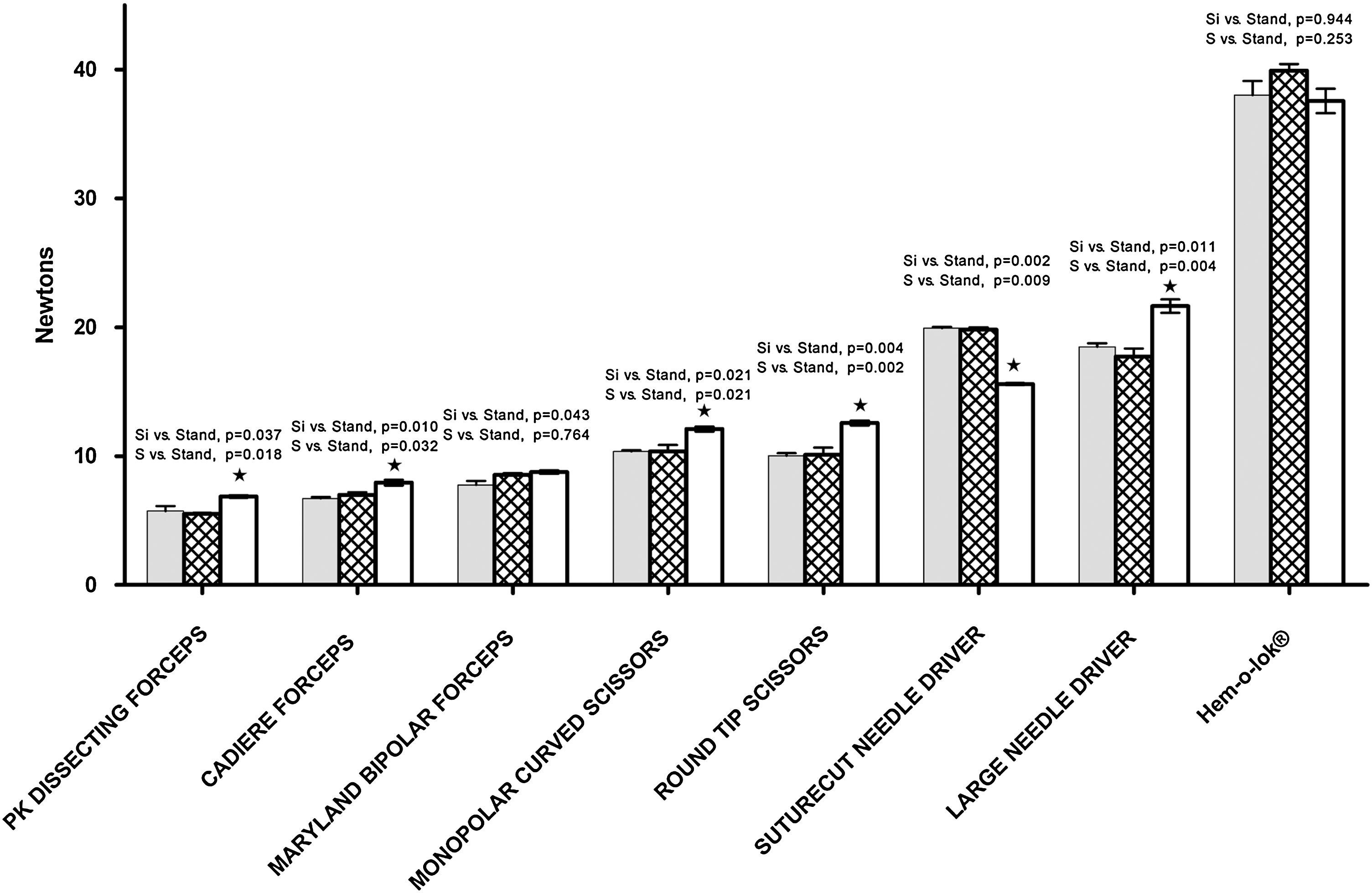
Comparison of grip forces in various instruments among different da Vinci robotic platforms. White bar = da Vinci Standard; striped bar = da Vinci S; gray bars = da Vinci Si; * = Standard platforms significantly different from the Si and S platforms on post hoc analysis of variance test.
All instruments were 8 mm unless otherwise stated.
p-Value determined by unpaired Student's t-test.
p-Value determined by analysis of variance.
Standard, da Vinci Standard Platform; S, da Vinci S Platform; Si, da Vinci Si Platform.
Leak point pressure was calculated using a bowel grasper and freshly harvested porcine renal artery. Leak point pressure was observed to be ∼830 mm Hg while using the 8 mm Bowel Grasper. Finally, commonly used open instruments were tested on the load cell as a reference point for comparison to the robotic instruments. These findings are summarized in Table 3.
Discussion
Robotic surgery has quickly gained in popularity and acceptance as an alternative to some open and laparoscopic procedures. As the only commercially available robotic surgical platform, over 150,000 urologic procedures are expected to be performed with the da Vinci surgical system in the upcoming year. 1
The current robotic platforms do not employ the use of haptic feedback. Surgeons must use visual cues to estimate the force and tension placed on tissues and sutures during the operation. Although the lack of haptic feedback does not appear to increase tissue injury or result in poorer oncologic outcomes, 6,7 the specific amount of force applied by the robotic instruments has never been examined. To our knowledge, this is the first study directly measuring the grip forces exerted by the robot instruments on the three different platforms.
We first examined the grip force at various angles afforded by the seven degrees of freedom. Minor deflections (movements along the distal wrist joint) and the neutral position exhibit the same amount of grip force, whereas major deflections (movements at the proximal wrist joint) result in a significantly lower grip force. This was confirmed in the right and left hand as well as between two different instruments. Although these differences were significant, the actual grip force difference was only ∼5% of the neutral position in the Maryland grasper and Large Needle driver. As a result, this difference is unlikely to be of any major clinical significance.
Differences also existed between new instruments and old instruments. It is not surprising that a previously unused instrument had a significantly higher grip force at all grasping angles compared with the same older instrument. In our trials we tested an extended use training instrument that had been used for over 2 years and compared it to an unused instrument. The actual differences were statistically significant, but by <10% in the neutral position for the new instrument. In a clinical setting where most EndoWrist instruments are limited to 10 uses, it is unlikely that these differences would be noted.
More importantly, grip force between the left and right arms of the robot did not differ when using the same instrument. Significant differences were observed among the various EndoWrist instruments and varied widely among the different types of instruments. Grasping or tissue handling instruments, such as the PK Maryland dissector and bipolar Maryland, had less grip force compared with needle drivers and Hem-o-lok clip appliers. This suggests that they will produce less tissue trauma or injury during surgery.
The Standard da Vinci surgical system displayed a significantly higher grip force for nearly all of the instruments tested when compared with the S and Si platforms. It was not surprising that the S and Si surgical platforms displayed similar grip forces among instruments, as much of the advancement between the two systems is at the surgeon console and not the patient side cart; however, there were differences between the Si/S and Standard systems. Much of these differences in grip force (which again were small) could be the result of using instruments of differing ages. Alternatively, the differences may be a result of the construction of the Standard instruments or patient side cart.
Using an 8-mm bowel grasper (which some surgeons may utilize on the fourth arm as a vascular clamp during a robotic partial nephrectomy), we occluded a freshly harvested porcine renal artery and tested for leak pressures. When compared with the leak pressures reported by Lee et al. 5 (who compared leak pressures in handheld Satinsky clamps and various bulldog clamps), the robotic leak pressures were greater than the bulldog clamps but less than the handheld Satinsky clamps. This suggests that using a robotic bowel grasper as a vascular clamp may be safe and effective; however, further testing, including histologic analysis, should be performed.
Finally, we compared the obtained grip forces in common open instruments. Each open instrument set at one click, with the exception of the long 255-mm Allis, was much higher than the commonly used robotic instruments. This finding offers some reassurance that the robot is exerting less force when grasping tissue compared with commonly used open instruments.
This study had some limitations, including the use of extended use training instruments for most of the measurements, as well as the use of the Standard platform patient side cart that is over 5 years old. Extended use training instruments are not validated to maintain the programmed closing forces that are standard for clinically used instruments. Second, because of the small tips of the robotic instruments, a housing unit was manufactured to measure closing force, introducing another degree of uncertainty into the measurements. Finally, histological analysis of direct tissue damage was not performed. Despite these limitations, we feel that this article highlights the differences found in grip force among various robotic instruments, various robotic platforms, and at the various degrees of freedom. Future studies are needed with limited use patient instruments.
The da Vinci robot is a major advancement in minimally invasive surgery, and urologists have been at the forefront in pursuing and utilizing this new technology. Although the current technology may be limited by the lack of direct haptic feedback, this study is the first to establish direct forces exerted by the robotic instruments. It provides an initial step in creating data that may eventually lead to the utilization of computer-generated haptics for the surgeon and may be important for instrument selection during the delicate portions of an operation.
Conclusion
Different grip forces were observed among the various robotic training instruments commonly used during urologic surgery and between the Standard and the S and Si platforms. The grip force of the robotic instruments tends to be less than that observed in comparable open surgery instruments, suggesting the general safety of robotic instruments in handling delicate urologic tissues. Further evaluation of the grip force of clinical, limited-use robotic instruments is needed.
Footnotes
Disclosure Statement
No competing financial interests exist.