
Abstract
Background and Purpose:
Laparoscopic endoscopic single-site surgery (LESS) has recently emerged as an attempt to enhance cosmetic benefits and reduce morbidity; however, LESS for radical cystectomy is still not well established. Here we describe the technique of hybrid LESS for radical cystoprostatectomy and orthotopic ileal neobladder (RC-OIN), and evaluate its feasibility and safety.
Patients and Methods:
Between November 2008 and October 2009, 12 men with bladder cancer underwent hybrid LESS for RC-OIN. A homemade multichannel port, made from two stretchable rings and a surgical glove with trocars and valves attached to its fingers, was placed into a 4- to 5-cm midline incision in the lower abdomen and was used for laparoscopic instruments. Another subumbilical port was placed for the laparoscope. Extended bilateral pelvic lymphadenectomy was performed by the lateral view; radical cystoprostatectomy was completed laparoscopically; construction of the ileal neobladder was performed extracorporeally; and the neobladder was anastomosed to the urethral stump laparoscopically, with a slipknot running suture technique. Perioperative, functional, oncologic data and complications were collected and analyzed.
Results:
All operations were performed successfully without conversion to conventional laparoscopic radical cystectomy or open surgery. There was no perioperative mortality or port-related complications. The median operative time was 383 minutes. Median blood loss was 150 mL. A median of 25 lymph nodes were removed. Surgical margins were tumor free in all cases.
Conclusions:
Hybrid LESS for RC-OIN is technically feasible with effects similar to those of conventional laparoscopic procedures. Further instrument and technique improvement are necessary to shorten operative time and reduce intraoperative difficulties.
Introduction
Patients and Methods
Patients
Between November 2008 and October 2009, 12 men with a median age of 65 years (range 54–76 years) with bladder cancer underwent hybrid LESS for RC-OIN. Patient data are presented in Table 1. All patients were evaluated preoperatively to preclude distant metastasis. Of the 12 patients, 2 had previous abdominal surgery: 1 patient had a herniorrhaphy, and another had an appendectomy. This study was approved by the Institutional Review Board of our hospital, and written informed consent was obtained from all patients. Patient preparation has been described previously. 7 General anesthesia with endotracheal intubation was used for all patients.
BMI = body mass index; Cis = carcinoma in situ.
Equipment
A homemade multichannel port, a 10-mm, 30-degree video laparoscope (Olympus Surgical, Orangeburg, NY), and conventional laparoscopic instruments were used. Precurved irrigation suction was used for some cases to facilitate the operation. Two stretchable rubber rings, one 6-cm and another 8-cm in diameter, and a surgical glove were used as the materials for the homemade multichannel port (Fig. 1A). The 8-cm ring was attached to the cuff of the glove to act as an outer ring. The 6-cm ring was set at 5 to 6 cm (depending on the thickness of the abdominal wall) from the cuff of the glove and was slipped through the outer ring to form an inner ring (Fig. 1B). The fingertips of the glove were cut off and fixed with trocars and valves: One 12-mm trocar, one 5-mm trocar, and two rubber valves. The 12-mm trocar provided an access path for CO2, laparoscope, and needle passing.

Technique
The patients were placed in the Trendelenburg position and a 4- to 5-cm midline incision was made in the lower abdomen (Fig. 2A). The inner ring of the multichannel port was inserted through the incision into the abdominal cavity. The outer ring was kept outside the incision. The inner and outer rings were pressed against the inner and outer abdominal wall by pulling up the glove (Fig. 2B). CO2 insufflation of the abdomen created tension between the two rings to prevent air leakage and maintained the intra-abdominal pressure (Fig. 2C). After establishing pneumoperitoneum, another port was placed at the umbilicus site under laparoscopic guidance.

The surgical procedure was similar to that of conventional laparoscopic RC. 7 The primary differences included the use of a homemade multichannel port; performing an extended pelvic lymphadenectomy in a lateral view; and cumbersome urethra-pouch anastomosis with the slipknot running suture technique.
Extended laparoscopic lymphadenectomy
The left-side extended pelvic lymph node dissection (EPLND) was performed first with the patient rotated left side up at 15 to 30 degrees, and the operator and the camera holder standing on the right side of the patient (Fig. 3). The ureter was identified and mobilized from the bifurcation of the common iliac artery to the ureterovesical junction, and transected with LigaSure™ (Valleylab, Boulder, CO). The extended boundaries of the lymph node dissection have been described previously. 8 The vessel sheath of the external iliac artery was split longitudinally from the bifurcation of the common iliac artery with J hook electrocautery and extended to the circumflex iliac vein. The external iliac vein, which ran medially and posteriorly to the external iliac artery, was identified and mobilized. After dissection along the medial aspect of the external iliac vein, the obturator nerve was identified, the fatty tissue that overlays the internal iliac vessels was dissected, and the umbilical artery was transected. The tissue of the obturator–internal iliac group was removed. The fatty tissue along with the external iliac artery medial to the genitofemoral nerve was removed, and the external iliac artery and vein were skeletonized circumferentially. The adipolymphatic tissue that surrounded the common iliac arteries and the aortic bifurcation was cephalad dissected. Finally, the presacral node between the bilateral common iliac arteries was dissected (Figs. 4A and B). The resected adipolymphatic tissue in each location was placed separately in a specimen bag and extracted through the rubber valve of the multichannel port.

The hybrid port with instruments in place and the surgical team on the left side performing extended pelvic lymphadenectomy.
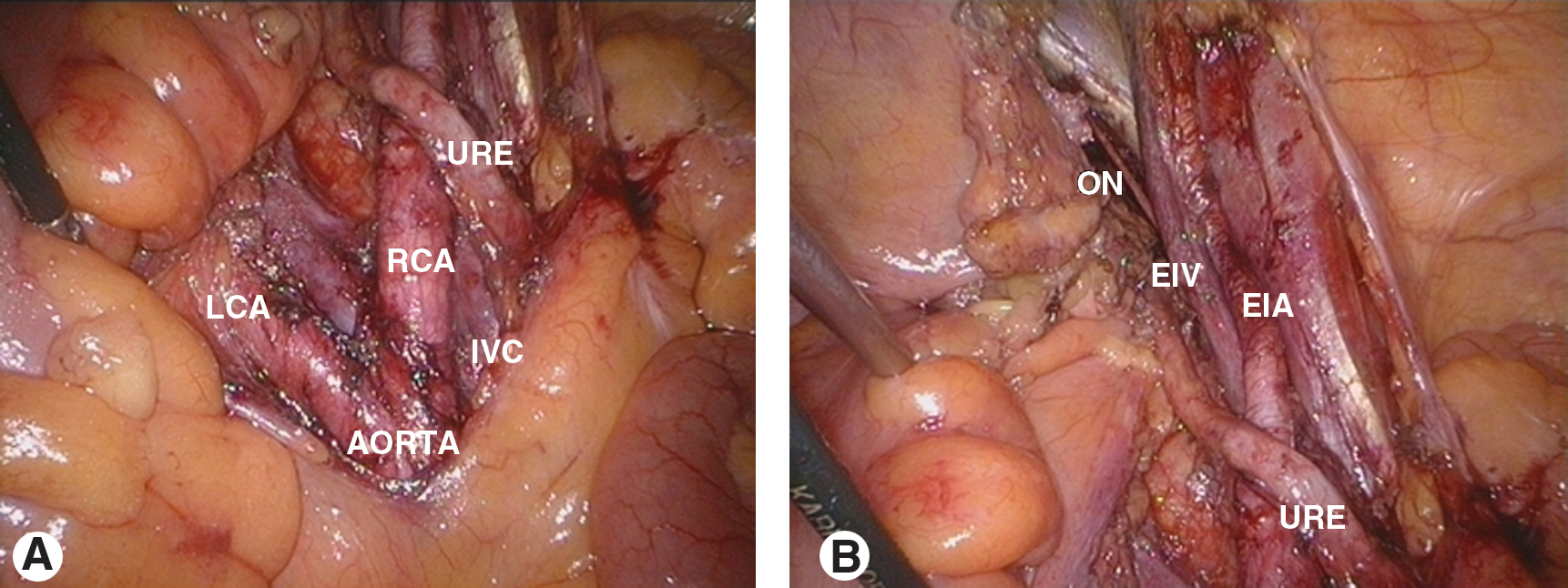
Right-side EPLND was performed similarly with the patient positioned right side up and the operator and camera holder on the left side of the patient.
Laparoscopic radical cystoprostatectomy
A traction stitch was used to pull the bladder forward for exposure of the cul-de-sac, and the peritoneum of the anterior wall of the cul-de-sac was opened. The ampullae of the vas deferens and seminal vesicles were then divided. Dissection was advanced toward the Denonvilliers fascia, which was incised horizontally to enter the Denonvillier space. The lateral pedicles of the bladder were dissected with LigaSure. An inverted U-shaped peritoneotomy was made to expose the anterior bladder wall and the Retzius space. The endopelvic fascia was incised bilaterally to expose the lateral surface of the prostate; a slipknot with PBS II stitch (Ethicon Endo-Surgery, Inc, Cincinnati, OH) (Fig. 5) was formed extracorporeally and delivered into the abdominal cavity; and the dorsal vein complex was sutured and ligated to guarantee good hemostasis. The bilateral pedicles of the prostate were divided with LigaSure.

A nerve-sparing procedure was performed in four patients, in whom the lateral pedicles of the prostate were divided as close as possible to the prostate, with the Hem-o-lok ligation system (Teleflex Medical, Limerick, PA) and scissors. The dorsal vein complex was transected to expose the apex of the prostate and urethra. The anterior urethral wall was incised; the Foley catheter was pulled out and clamped with a Hem-o-lok clip to maintain balloon inflation in the bladder, to avoid spillage of urine and carcinoma cells, and then transected with a harmonic scalpel. The Foley catheter was retracted cephalad to expose and divide the posterior wall of the urethra and rectourethralis muscle, which completely released the specimen.
Extracorporeal construction of the orthotopic ileal pouch
The outer part of the multichannel port was cut off and everted to the outer ring, which maintained the glove covering over the incision. The specimen was immediately removed through the port, and the terminal ileum and both ureters were brought out. Bilateral ureteral stents were placed. Construction of an M-shaped ileal neobladder and ureteral reimplantation were performed extracorporeally by means of a ureteral split-nipple (Fig. 6). 7 A 0.8-cm opening was made at the bottom of the pouch. A traction stitch was sutured between the lower margin of the opening of the pouch and tip of the Foley catheter before placing it into the abdomen.

Formation of the extracorporeal orthotopic ileal pouch while keeping the incision covered with the glove.
Laparoscopic urethra-pouch anastomosis
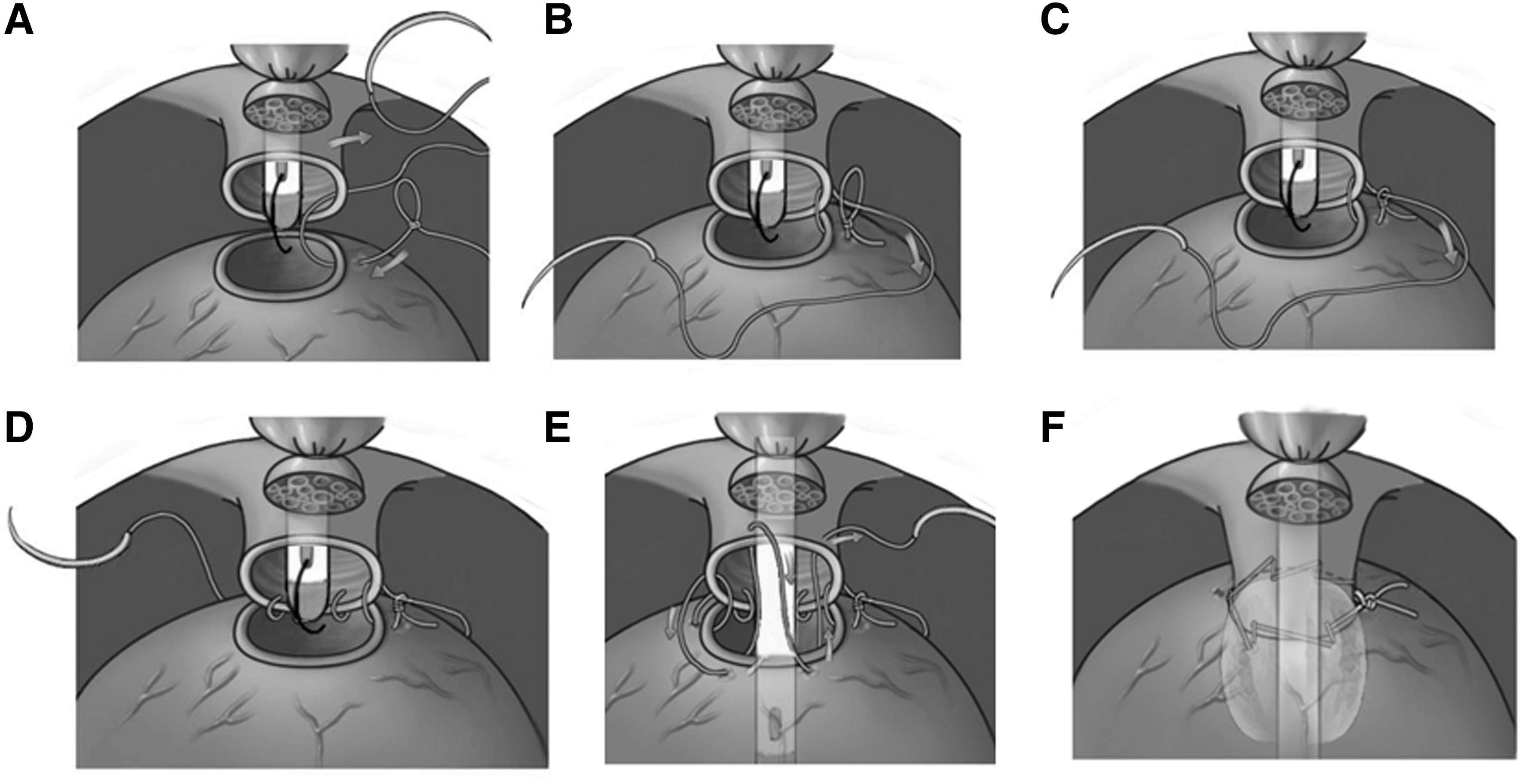
The opened port was removed and replaced by a new multichannel port. The urethra-pouch anastomosis was performed by pulling the traction stitch through the Foley catheter. 7 A slipknot was prepared extracorporeally and delivered into the abdominal cavity. A slipknot running suture was performed to facilitate the anastomosis (Fig. 7). The first stitch was placed at the 3 o'clock position; the needle was passed through the hitch of the slipknot, and the hitch was tightened; the knot was slipped and tightened; and the free-hand knot was formed intracorporeally. Running sutures were placed at the 5, 7, and 9 o'clock positions; the traction stitch was removed; the catheter was inserted into the pouch; the balloon was inflated with 20 mL physiologic saline; by pulling the catheter, the pouch was closed to the urethral stump. Another two stitches were placed at the 11 and 1 o'clock positions to anastomose the anterior walls of the urethral stump and the pouch. Both sides of the suture were tied with two knots with a right-angle forceps (Fig. 7). Finally, 100 mL of physiologic saline was injected to detect any leakage; two suction drains were placed in the pelvis; and the incisions were closed. The bilateral ureteral stents and pelvic drains were exited through the subumbilical incision.
The patients were followed up at 1, 3, 6, and 12 months postoperatively. At each follow-up time, urine cytology, routine laboratory blood testing, and CT of the thorax, abdomen, and pelvis were performed.
Results
Operative data
The results are summarized in Table 1. All procedures were completed successfully without conversion to conventional laparoscopy or laparotomy. The median operative time was 383 minutes (range 355–455 min). Median estimated blood loss was 150 mL (range 50–210 mL), and no patient needed a blood transfusion during or after surgery. Postoperative pain management consisted of an epidural catheter with morphine and intramuscular meperidine during the first postoperative day, and then minor analgesics for the next 2 to 5 days. All patients recovered bowel activity at 2 to 4 days postoperatively, and began food intake 1 to 2 days later.
Intra-abdominal drains were removed on postoperative days 4 to 6. The bilateral ureteral stents were removed on postoperative day 10, and the Foley catheter was removed on postoperative day 13. The median hospitalization time after operation was 15.3 days (range 14–18 d). Patients could ambulate at 1 to 3 days postoperatively and return to normal activity within 2 weeks. All patients were satisfied with the cosmetic results (Fig. 8).

Postoperative image of the incision.
Complications
There were no intraoperative complications and perioperative mortality. There were no port-related complications, such as wound infection, skin maceration, ventral hernia, or port-site seeding. The first patient experienced delirium 2 days after surgery and was treated successfully with conservative mangement. There were two patients with prolonged lymphatic leakage that was managed by extending the drainage time. No ureteral reflux was observed by cystography of the neobladder in any of the patients.
Neobladder and sexual function
We evaluated neobladder function at 6 and 12 months after surgery. According to the definition of Kulkarni and colleagues, 9 the daytime and nighttime continence rates were 83.3% (10/12) and 41.7% (5/12), respectively, at 6 months after the operation, and 90% (9/10) and 80% (8/10), respectively, for 10 patients at the 12-month follow-up. The mean maximal pouch capacity, residual volume, and peak flow rate were 281 mL (120–410 mL), 21 mL (0–100 mL), and 9.5 mL/s (5.9–25 mL/s) after 6 months of follow-up, and 369 mL (230–640 mL), 42 mL (0–180 mL), and 12.1 mL/s (7.1–28 mL/s) after 12 months of follow-up. No patient had urinary retention.
For four patients who underwent a bilateral nerve-sparing procedure, three completed 1 year of follow-up; one had spontaneous erection that was sufficient for intercourse; and one had erection after treatment with 100 mg sildenafil.
Histopathologic findings
Histopathologic examination revealed two pT1N0 G3, one pT1N0 G3 plus carcinoma in situ, one pT1N1 G3, two pT2aN0 G3, two pT2bN0 G2–3, one pT2bN1 G3, one pT3aN0 G2, one pT3aN0 G3, and one pT3bN0 G3 disease. The surgical margins were tumor free in all the patients; however, in one case, occult prostate adenocarcinoma was found. A median 25 lymph nodes were removed (range 12–46). Two patients with T3b disease or positive lymph nodes were given adjuvant chemotherapy after recovery.
Follow-up
The average follow-up time was 16.1 months (range 9–20 mos). All patients were alive and tumor free at the last follow-up in July 2010.
Discussion
In the past 3 years, with the evolution of commercial single-port access devices, LESS has advanced rapidly in the urologic field. 10 Using an R-port™ (Advanced Surgical Concepts, Wicklow, Ireland), Rané and coworkers 11 have reported the first single-port simple retroperitoneal nephrectomy and laparoscopic transperitoneal ureterolithotomy. Kaouk and colleagues 2 have reported seven patients who underwent single-port transumbilical urologic laparoscopic procedures with the Uni-X™ system (Pnavel Systems, Morganville, NJ). Other urologic LESS procedures using these two access devices have included nephrectomy, 3 pyeloplasty, ileal ureter, and psoas hitch ureteroneocystostomy, 4 live-donor nephrectomy, partial nephrectomy, 5 radical prostatectomy, and radical cystectomy. 12 Recently, Desai and associates 13 have reported their initial experience with LESS surgery in 100 urologic patients using the R-port.
The major barriers to the use of commercial single-port access devices include internal and external cumbersome instrument clashing and unreliable tissue handling, and unavailability of these specialized ports in China. In this study, we developed a device and successfully performed hybrid LESS RC-OIN in 12 patients. The improvements in technique of this hybrid LESS RC-OIN technique included the following: (1) A small incision was used for surgical access, specimen removal, and neobladder construction. (2) EPLND was performed from a side view with the surgeon and camera holder standing at the opposite side of the operative site. (3) A sling stitch through the abdomen was used to pull the bladder forward to expose the posterior aspect of the bladder. (4) A slipknot was used to facilitate ligation of the dorsal vein complex and urethra-pouch anastomosis. (5) The incision was sealed with a glove throughout the operation, which prevented contamination and tumor-cell seeding.
Although the procedure seemed to take longer than conventional laparoscopic RC, each intraoperative step was accomplished with confidence, and no major complications occurred. The negative surgical margins of the bladder specimen in all patients and a similar number of harvested lymph nodes as in conventional laparoscopic RC 14 support the hypothesis that the hybrid LESS RC-OIN procedure does not have an increased risk of poor tumor control.
Laparoscopic RC using two ports instead of one can decrease the difficulty of EPLND and ensure the extent of lymphadenectomy without compromising the cosmetic effect. A single transumbilical incision makes EPLND and urethra-pouch anastomosis difficult, and usually extension of the incision is necessary for extraction of the sample in patients with a large prostate or bladder tumor, and to return the neobladder to the abdomen.
Our homemade single-port access has several merits. First, it offers a simple, convenient, and flexible approach to perform LESS. The fingers of the glove provide channels for valves or different-sized trocars. Both 10-mm and 5-mm instruments can be used. Clashing of instruments and the laparoscope was minimized because the range of motion of the instruments was larger with our design than with commercial products. In addition, needles can be delivered into the abdominal cavity easily using a 12-mm trocar. Second, the homemade single-port access is more cost-effective than current commercial systems, and conventional surgical equipment can be used. Third, it can prevent subcutaneous emphysema, port-site infection, and bleeding, as well as contamination of the field with tumor cells while performing oncologic procedures. Lastly, it provides a good operative field without significant gas leakage, thus decreasing related intraoperative complications.
Our hybrid LESS RC-OIN has a unique learning curve, including navigating the instruments within a limited range of motion, coordination between the surgeon and the camera holder, and adaption of counterintuitive movements because of frequent crossing of the instrument shafts. With development of surgical equipment and novel innovations, hybrid LESS RC-OIN is likely to have an expanded role in the future and become more easily incorporated into standard practice.
Conclusion
Hybrid LESS RC-OIN is technically feasible with a low complication rate. It provides an easy, flexible, and cost-effective surgical method for the treatment of patients with muscle-invasive bladder cancer. Our initial experience is encouraging, but additional study and comparison of oncologic outcomes with conventional surgery are necessary.
Footnotes
Disclosure Statement
No competing financial interests exist.