
Abstract
Purpose:
To assess long-term oncologic outcomes in patients with renal pelvic cancer who are receiving nephrectomy plus endoscopy-assisted intussusception ureterectomy. There has been no large study reporting long-term oncologic outcomes of this approach in comparison with those of conventional nephroureterectomy plus bladder cuff removal.
Patients and Methods:
We reviewed 181 consecutive patients with renal pelvic cancer who underwent open nephroureterectomy with complete bladder cuff removal (cuff removal group, n = 33), nephroureterectomy with incomplete cuff removal (orifice-remaining group, n = 39), and nephrectomy with intussusception ureterectomy (intussusception group, n = 109).
Results:
Patients in the intussusception group had larger tumor size, higher histologic grade, and more advanced pathologic stage (P = 0.005, 0.021, and 0.030, respectively), while the incidence of coexistent bladder/ureteral cancer was lower in this group (P < 0.001). The mean operative time was shorter in the intussusception group than in the cuff removal and orifice-remaining groups (201.2 ± 33.1 and 221.5 ± 47.2 min, respectively, P < 0.001). The 5-year extraurinary tract recurrence-free survival rate in the intussusception and cuff removal groups was 74.8% and 71.4%, respectively (log-rank P = 0.766), and it was lower in the orifice-remaining group compared with that in the intussusception group (P = 0.031). The 5-year urinary tract recurrence-free survival rate in the intussusception, cuff removal, and orifice-remaining groups was 76.6%, 65.0%, and 65.0%, respectively (intussusception vs cuff removal: P = 0.089). With both univariate and multivariate analyses, intussusception ureterectomy had no significant impact on urinary tract recurrence (multivariate P = 0.553, hazard ratio = 0.784).
Conclusions:
Nephrectomy plus endoscopy-assisted intussusception ureterectomy is an oncologically safe alternative for renal pelvic cancer patients, which is possibly associated with less patient morbidity.
Introduction
In current practice, several surgical approaches for the distal ureter may be selected according to the disease extension or among institutions. They represent cuff removal and transvesical detachment of the distal ureter; these techniques are applied in combination with open or laparoscopic surgery, 2,6 –8 and each has practical or possible advantages and disadvantages associated both with technical and oncologic matters. Patients who are treated with open total nephroureterectomy with bladder cuff removal receive a long lumbar-abdominal incision or two/separate ones, thereby associated with considerable morbidity, whereas management of the distal ureter has been controversial in laparoscopic approaches. 2,9 Thus, the optimal procedure for management of the distal ureter and ureterovesical junction has not been determined, and the open approach remains a standard option and also as a control/reference when comparing the technical and oncologic outcomes among the mentioned modalities. 2,10
The endoscopy-assisted ureteral intussusception technique for nephroureterectomy has been reported with its safety and advantages, such as less patient morbidity, 11 and has recently been introduced in seminar articles with laparoscopic approaches. 3,8 Its principled method was established and described by Angulo and associates. 11 Its application, however, is still limited, probably because of the technical problem and the absence of studies that enrolled a statistically sufficient number of patients and reported long-term oncologic outcomes in comparison with conventional nephroureterectomy plus bladder cuff removal.
Since 1992, we have used the ureteral intussusception technique in surgery for patients with renal pelvic cancer. In the present study, we showed long-term oncologic outcomes in patients with renal pelvic cancer who underwent nephrectomy plus endoscopy-assisted intussusception ureterectomy, as well as its technical notes and limitations based on experience with more than 100 patients receiving this technique for renal pelvic cancer.
Patients and Methods
Patient characteristics
We reviewed the medical records of 185 consecutive patients with renal pelvic cancer who were treated with elective radical surgery at Niigata Cancer Center Hospital between January 1994 and December 2006. All patients gave informed consent. The procedure for this research project was approved by the Ethics Committee of our institution. Clinical and pathologic stages were determined by experienced diagnostic radiologists and surgical pathologists and were standardized according to the International Union Against Cancer classification of 2002. Clinical staging routinely included abdominal and pelvic CT, cystoscopy, intravenous urography, and chest radiography or thoracic CT. Isotope bone scanning was performed when considered necessary based on symptoms and laboratory data. Exclusion criteria for subjects were: Patients with distant metastasis at diagnosis and those having synchronous bilateral tumors in the upper urinary tract. In total, 181 patients comprised the final study groups (Table 1).
Surgical procedures and patient stratification
Patients were treated by open nephroureterectomy with bladder cuff removal (n = 72) or open nephrectomy with intussusception ureterectomy (intussusception group, n = 109). In addition, patients receiving the former were categorized into two groups: Patients cystoscopically certified with complete resection of the ipsilateral ureteral orifice (cuff removal group, n = 33) and those possibly with the remaining orifice determined by postoperative cystoscopy (orifice-remaining group, n = 39). In 21 patients in the orifice-remaining group, incomplete cuff removal was suggested because of technical limitations or patient comorbidity; in the other 18 patients, no further information was available regarding the remaining orifice. All patients were treated by experienced urologists.
Definite decision criteria for surgical options were absent, and they were determined based on informed consent in general; in patients who had undergone previous abdominal surgery, nephroureterectomy plus bladder cuff removal was selected, and for those possibly having tumors concurrent in the distal ureter, this approach was also chosen. Four patients with a previous pelvic surgery were treated with nephroureterectomy plus bladder cuff removal. In patients with locally advanced disease, nephrectomy with intussusception ureterectomy was preferred.
Standardized nephroureterectomy with bladder cuff removal were performed as follows: An elongated 15 to 25 cm thoracoabdominal incision was begun over the 11th or 12th rib or off the tip of the 11th or 12th rib with patients in the lateral position, and radical nephrectomy was performed in a retroperitoneal approach. Without ureteral disconnect, the kidney was taken out of the incision. Subsequently, total ureterectomy with complete distal ureter resection and extravesical bladder cuff removal was performed to excise the specimen en-bloc. All patients underwent renal hilar lymphadenectomy and, if necessary, para-aortic lymphadenectomy according to a defined or modified lymph node dissection protocol. Defect of the bladder was suture-closed in two layers.
Nephrectomy plus intussusception ureterectomy was performed with patients in the less intense lithotomy position. An 8 to 15 cm modified Chevron incision was made, and radical nephrectomy with lymphadenectomy similar to that in nephroureterectomy with cuff removal was performed in the transperitoneal approach. During nephrectomy, the ureter was ligated and transected; in all four patients with coexistent ureteral tumors, the ureteral lesions were localized in the proximal ureter, and the ureter was transected at the distal site of the ureteral tumors with a surgical margin. We developed the similar technique described by Angulo and colleagues. 11
Technical notes for intussusception ureterectomy are as follows: After nephrectomy, a 7F polypropylene catheter is antegradely inserted from the proximal end of the ureter to the bladder (Figs. 1A, 1B). The ureter is sutured and attached to the catheter using 2-0 polyglactin through side holes of the catheter. Minimal ureterolysis is important for successful intussusception. When extra ureterolysis is performed to facilitate the antegrade catheterization, the released ureter occasionally becomes accordion-pleated in the beginning of the ureteral intussusception, making following intussusceptions difficult. The mucosa around the ureteral orifice is deeply coagulated using transurethral resection endoscope and electrode system (resection of the orifice is not necessary; deep circumferential coagulation around the orifice is sufficient: Fig. 1C), and the distal end of the catheter is induced out of the urethral meatus (Fig. 1D). Anchoring the lateral and opposite sides of periureteral connective tissue 5 mm from the proximal end with tweezers, another surgeon plunges the attached catheter into the ureter, and simultaneously, an endoscopist pulls the catheter out of the urethral meatus. Thereby, the inverted and reversed ureter is detached with the catheter from the meatus (Fig. 1E). The bladder mucosal defect is just coagulated under cystoscopy to control bleeding (although always minor: Fig. 1F), and no additional treatment is given for the bladder defect or extravesical field where the distal ureter is removed. Transurethral resections of coexistent bladder cancer were concurrently performed with intussusception ureterectomy.
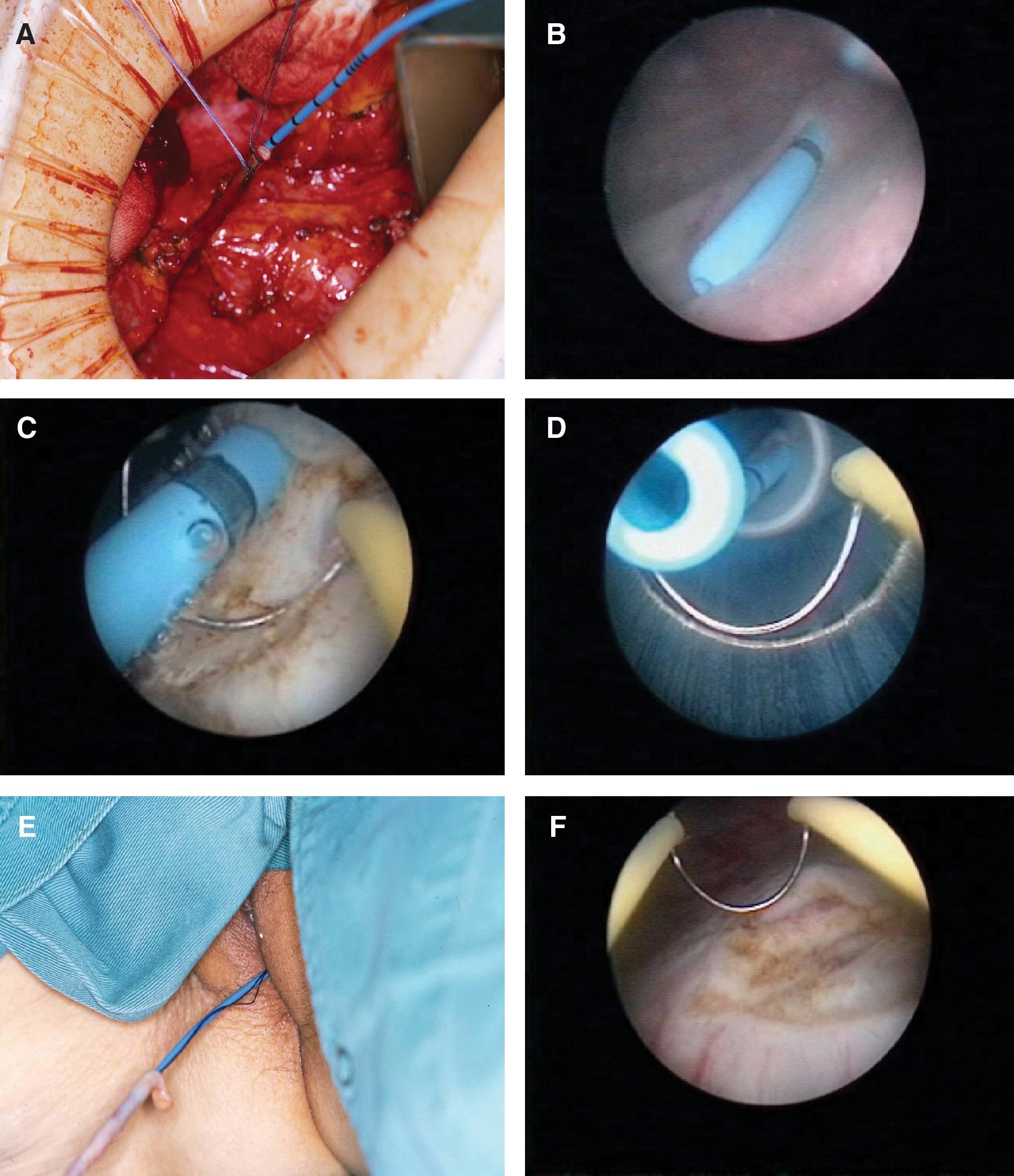
(
The patients were followed postoperatively with abdominal-pelvic CT and chest radiography or thoracic CT every 3 to 6 months, and cystoscopy with urine cytologic examinations every 3 months for the first 2 years; for the next 3 years, these examinations were performed at 6-month intervals in patients without intravesical recurrence, and thereafter at 6- to 12-month intervals. Isotope bone scanning and bone magnetic resonance imaging were performed when considered necessary based on symptoms and laboratory data. We defined metastatic, lymph node, or local recurrence as extraurinary tract recurrence, and recurrence in the bladder or possible residual distal ureter as urinary tract recurrence. The median observation period was 60, 67, and 69 months in the intussusception, cuff removal, and orifice-remaining groups, respectively (P = 0.157).
Statistical analysis
In addition to the chi-square test, the Mann-Whitney U test was used to compare unpaired parameters among subgroups. Survival curves were generated using the method of Kaplan and Meier. Univariate and multivariate analyses for survival-associated parameters were performed using Cox proportional hazard models. Statistical analyses were calculated and tested using SPSS software version 15.0 (SPSS, Inc., Chicago, IL) and Prism Version 4.02 (GraphPad Software, Inc, San Diego, CA) for Windows-based computers. The test was two-sided, and P < 0.05 was considered significant.
Results
Perioperative outcomes and complications
Patient demographics are summarized in Table 1. The three groups were comparable in age and sex fraction. The mean operative time was shorter in the intussusception group than in the cuff removal and orifice-remaining groups (201.2 ± 33.1 and 221.5 ± 47.2 min, respectively, P < 0.001). Blood loss was not different among the three groups (data not shown). There were no differences in the incidence of total surgical-site infection, remote infections such as pneumonia, or postoperative ileus among the three groups (data not shown). Delayed postoperative bleeding was found in one and one patient in the cuff removal and intussusception groups, respectively. Incisional/abdominal-wall hernia emerged in one patient in the cuff removal group.
Three patients experienced perioperative or postoperative complications specific for intussusception ureterectomy; in a 67-year-old woman with right renal pelvic cancer, detachment of bladder mucosa extending from the trigonum to the bladder neck occurred probably because of an insufficient coagulation around the ureteral orifice. In a 76-year-old man with right renal pelvic cancer, urethral injury by the ureteral catheter was observed, and a 63-year-old man with left renal pelvic cancer experienced bloody tamponade of the bladder on the first postoperative day. Mentioned complications were successfully managed with transurethral manipulations or conservative treatments in all of them. In four (3.7%) patients, intussusception failed once and was successfully performed in the repeated procedure with the ureter reattached to the 7F polypropylene catheter. No patient in the intussusception group experienced conversions to other surgical procedures.
Oncologic outcomes
Histopathologic findings and adjuvant/auxiliary treatments are also shown in Table 1. No difference was found in terms of previous treatments such as previous/neoadjuvant chemotherapy. Two patients had a positive margin in the removed bladder cuff, and one patient in the intussusception group had a positive margin in the ureterovesical junction. Patients in the intussusception group had larger tumor size, higher histologic grade, and more advanced pathologic stage (P = 0.005, 0.021, and 0.030, respectively), while the incidence of coexistent bladder/ureteral cancer was lower in this group (P < 0.001).
In the present series, six patients were lost or unable to receive follow-up examinations between 24 and 60 months after surgery, and two patients died of other causes 41 and 52 months postoperatively. Extraurinary tract recurrence-free survivals are presented in Figure 2. The 5-year extraurinary tract recurrence-free survival rate in the intussusception and cuff removal groups was 74.8% and 71.4%, respectively, and it was not different between the cuff removal and intussusception groups (log-rank P = 0.766). The 5-year extraurinary tract recurrence-free survival rate was lower in the orifice-remaining group than in the intussusception group (P = 0.031). In the intussusception group, 13 patients with pT3–4 and pN1–3, who experienced extraurinary tract recurrence, had cause-specific death 3 to 21 months postoperatively; 10 patients with pT3–4, pN0 died of systemic metastasis 4 to 24 months after surgery.
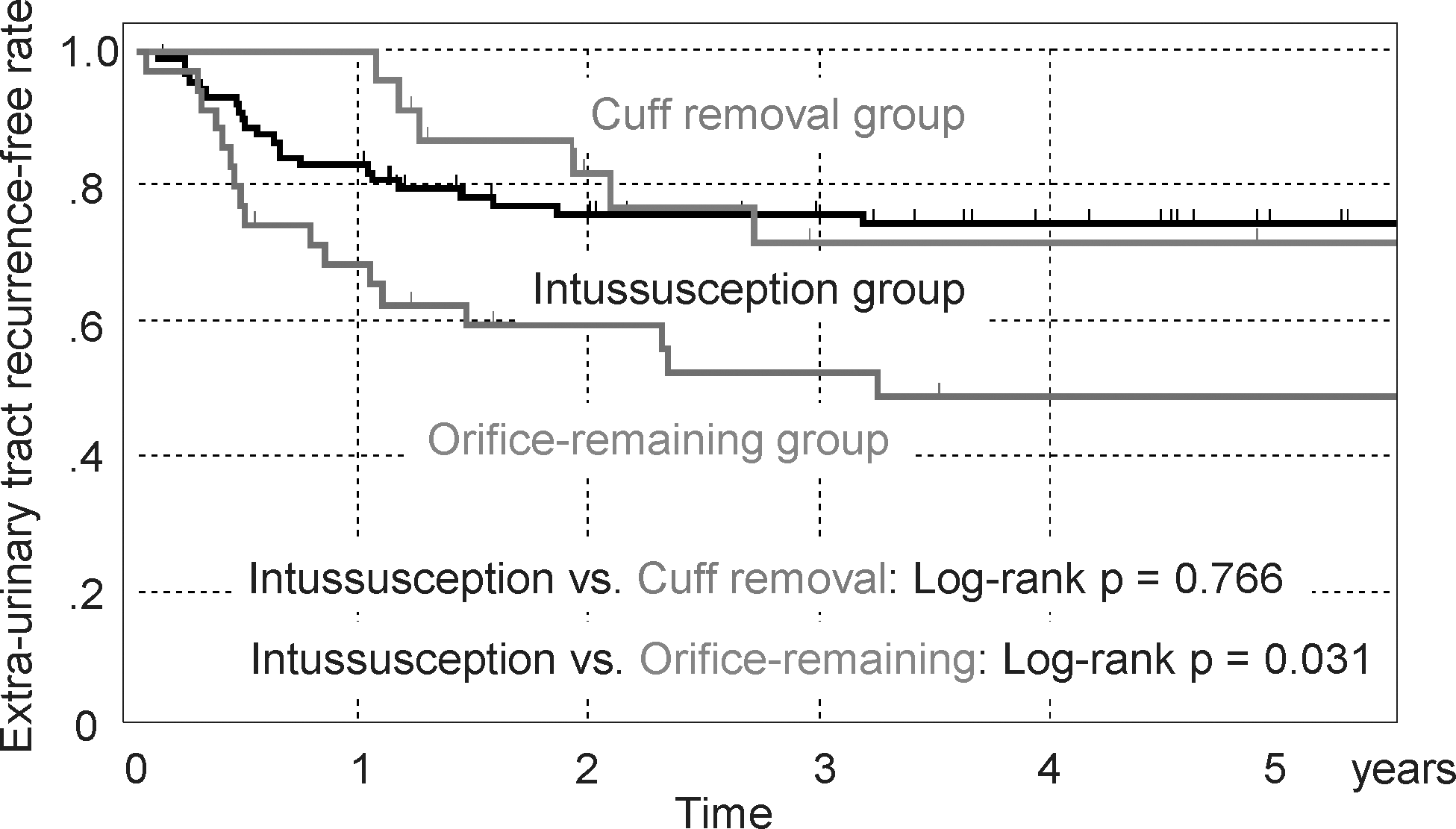
Extraurinary tract recurrence-free survival.
Figure 3 shows urinary tract recurrence-free survivals. The overwhelming majority of patients who experienced urinary tract recurrence had recurred tumor in the bladder, and one patient in the orifice-remaining group had recurrence in the residual distal ureter. The 5-year urinary tract recurrence-free survival rate in the intussusception, cuff removal, and orifice-remaining groups was 76.6%, 65.0%, and 65.0%, respectively, and the urinary tract recurrence-free survival rate did not differ among the three groups (intussusception vs cuff removal: P = 0.089, intussusception vs orifice-remaining: P = 0.188).
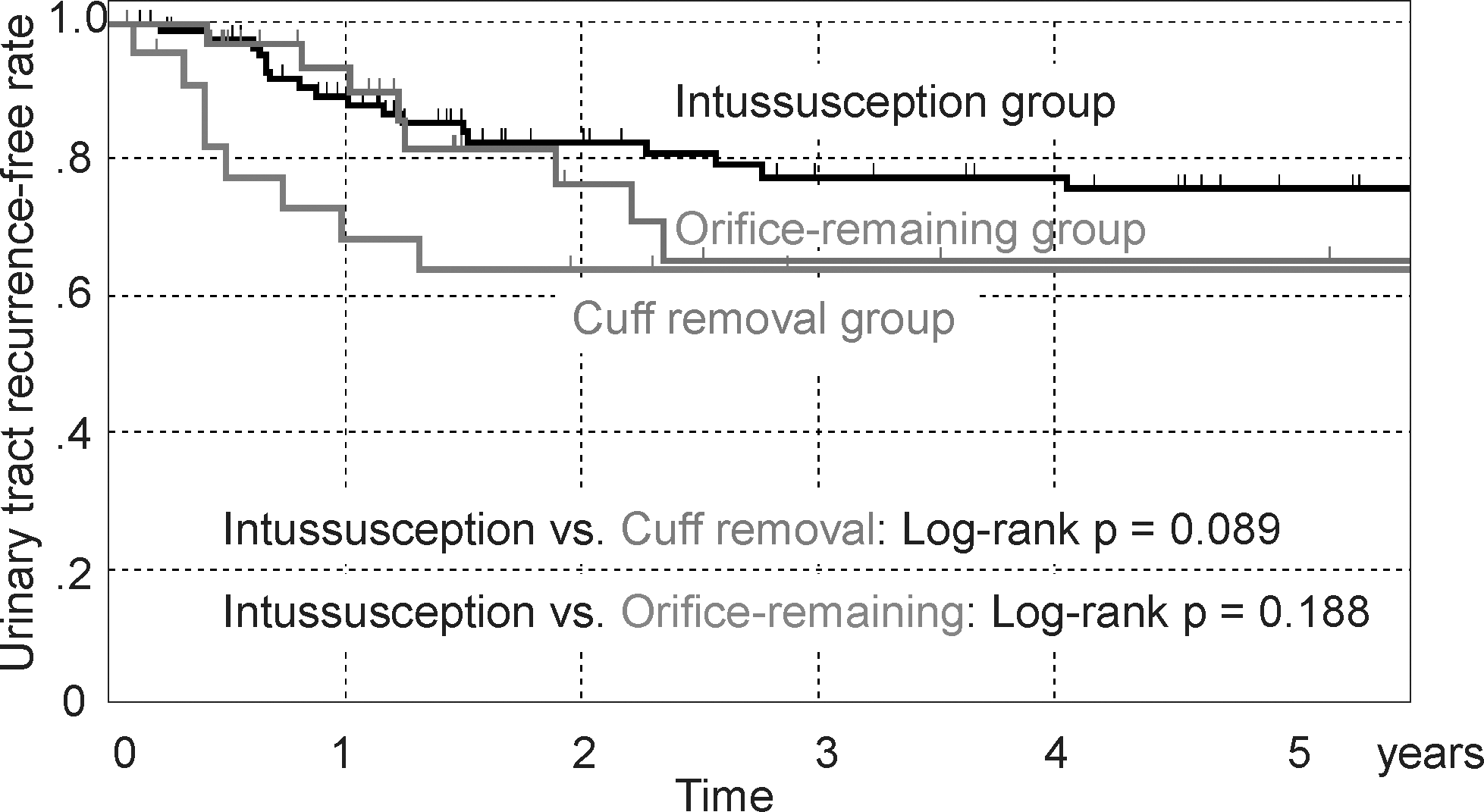
Urinary tract recurrence-free survival.
Table 2 shows univariate and multivariate analyses for risk factors in urinary tract recurrence. In univariate analysis, the urinary tract recurrence rate was lower in patients with a solitary tumor than in those with multiple tumors (P = 0.043). In multivariate analysis, the absence of coexistent bladder cancer was an independent factor for less urinary tract recurrence (hazard ratio = 0.257, P = 0.009). The intussusception had little impact on the urinary tract recurrence (hazard ratio = 0.784, P = 0.553). In the intussusception group, one patient with pT4 pN1 disease without coexistent bladder cancer experienced intravesical recurrence and died from systemic metastases 8 months postoperatively; 18 patients with pT3–4, pN0 without coexistent bladder cancer had intravesical recurrence 3 to 18 months after surgery. Two patients with pTa without coexistent bladder cancer had intravesical recurrence 6 and 27 months after surgery, and both of them were disease-free over 7 years. In this group, four patients with pT3, pN0, and coexistent bladder cancer had intravesical recurrence 3 to 15 months after surgery, and one of them had cause-specific death 14 months after surgery.
CI = confidence interval.
Discussion
The possible problems/limitations for intussusception ureterectomy represent ureteral transection/incision and technical failures. The former might be associated with seeding of malignant cells, leading to local recurrence. 8 The rationale of surgery for malignant tumors is excision: Complete en-bloc resection to prevent tumor dissemination. 1 The ordinary open method, which appears to promise whole resection of the distal ureter and orifice, meets such underlying principle, and has therefore been continued. 1,3,8 The specimen was also incised around the orifice in cuff removal; urine extravasation possibly occurs in the retrovesical site in both cuff removal and intussusception ureterectomy. 12 The present study suggested that disease recurrence from dissection of the specimen has barely been encountered in both cuff removal and intussusception ureterectomy.
Technical failure may also be a matter of concern in the intussusception technique. In a recent review of 146 patients in eight previous series, who underwent intussusception ureterectomy, the mean failure rate was 13.3% (range 0%–26.3%). 8 Macejko and colleagues 8 thus concluded that the routine use of the ureteral stripping technique is not recommended. In the present study, the majority of patients had renal pelvic cancer alone, and coexistent ureteral tumors were significantly less frequent in the intussusception group. Also, patients with a history of pelvic or abdominal surgery, who were thought technically and anatomically problematic for intussusception ureterectomy, were treated with conventional nephroureterectomy plus bladder cuff removal. These patients' background/selection possibly contributed to the high success rate in our study.
A learning curve is seen in surgical procedures, 13 and this is also the case in intussusception ureterectomy. Yet it is easy to learn and can be performed successfully just following the aforementioned technical notes and a few experiences. No specific device is needed, and the present results also showed its safety.
The current study showed the postoperative extraurinary tract recurrence rate comparable between the intussusception technique and conventional nephroureterectomy with complete bladder cuff removal in patients with renal pelvic cancer. In addition, this study suggested the possible poorer prognostic outcome in patients who were receiving incomplete orifice removal (Fig. 2); however, it is also conceivable that curable surgery might be difficult in these patients because of disease extension, anatomic limitations, or comorbidities. Urinary tract recurrence appeared less frequent in the intussusception group, although the difference was not significant with the log-rank test (Fig. 3).
A relatively high intravesical recurrence rate after this procedure was reported in a previous comparative study by Saika and associates 14 ; 10 of the 28 (35.7%) patients who were receiving intussusception ureterectomy had postoperative intravesical recurrence. In their procedure, retrograde ureteral catheterization was first performed during surgery, whereas antegrade ureteral catheterization was conducted after nephrectomy in our patients. Such variance might involve different outcomes. Also, patient characteristics, study design/volume, and preoperative staging modalities varied among previous reports. Because the patient demographics having an influence on oncologic outcomes were different among the present patient groups, we applied multivariate analysis to compare urinary tract recurrence between the intussusception and cuff removal groups, but the hazard ratio by intussusception ureterectomy was not significant (Table 2).
In the present study, the intussusception group had larger tumor size, higher histologic grade, and more advanced pathologic stage than the cuff removal groups (P = 0.005, 0.021, and 0.030, respectively, Table 1); it was speculated that the transabdominal surgical approach in radical nephrectomy plus intussusception ureterectomy was preferred to obtain a surgical field probably proper for patients with advanced stage disease. Despite the poorer disease characteristics, oncologic outcomes in the intussusception group were not inferior to those in the cuff removal groups. Also, intussusception ureterectomy has been associated with less patient morbidity, 11,15 although we could not provide evidence except for shorter operative time, because of the limitation of data acquisition in the present study. Shorter operative time and hospital stay in patients receiving intussusception ureterectomy were reported in a previous study with the smaller number of participants. 11
In terms of development for less invasive surgery, laparoscopic nephrectomy followed by endoscopy-assisted intussusception ureterectomy may be a feasible approach, and a study with combined laparoscopic nephrectomy and intussusception ureterectomy is currently under way with longitudinal surveillances of functional results such as health-related quality of life.
Conclusion
Nephrectomy plus endoscopy-assisted intussusception ureterectomy can be a feasible and safe alternative for patients with renal pelvic cancer, which is associated with equivalent oncologic outcomes and probable less patient morbidity compared with conventional nephroureterectomy with bladder cuff removal. Our study had several limitations, such as the retrospective design, absence of randomization, and the relatively small number of patients in control groups. To overcome these restrictions and to develop less invasive and oncologically safe procedures for patients with renal pelvic cancer, further studies are warranted.
Disclosure Statement
No competing financial interests exist.