
Abstract
Background and Purpose:
Hand-assisted laparoscopic surgery (HALS) is an integral part of the urologist's armamentarium. We aimed to perform a comprehensive meta-analysis comparing HALS renal surgery with open and laparoscopic techniques.
Methods:
A systematic review and meta-analysis of HALS renal procedures (donor nephrectomy, nephrectomy, or nephroureterectomy) from 1996 to 2007 was performed.
Results:
Sixty-two studies of 30 donor nephrectomy, 21 radical nephrectomy, and 14 nephroureterectomy procedures in 5446 patients were included in the analysis. In donor nephrectomy, estimated blood loss (EBL) was statistically significant for HALS vs the open and laparoscopic cohorts, −69.0 mL (95% confidence interval [CI], −129.7, −8.2) and −40.1 mL (95% CI, −68.2, −12.0), respectively. Length of stay (LOS) was shorter compared with the open group, −1.7 days (95% CI, −2.3, −1.1). For nephroureterectomy, EBL (−29.9 mL (95% CI, −242.3, 182.5)), and LOS (−1.5 d [95% CI, −2.8, −0.3]) again favored HALS vs open procedures. Operating room (OR) time and warm ischemia time (WIT) were statistically significant in favor of HALS donor nephrectomy vs the laparoscopic cohort; −36.8 minutes (95% CI, −61.3, −12.3) and −1.3 minutes (95% CI, −1.8, −0.7), respectively. For radical nephrectomy, both EBL −232.9 mL (95% CI, −383.6, −82.2) and LOS −2.4 days (95% CI, −3.5, −1.3) were statistically significant, favoring HALS vs the open group.
Conclusion:
We report the largest meta-analysis of HALS renal surgery to date. When compared with open surgery, HALS allows for a significant decrease in EBL and LOS. Compared with laparoscopic donor nephrectomy, HALS resulted in a significant decrease in blood loss, OR time, and WIT.
Introduction
Although studies have demonstrated advantages of HALS in terms of less bleeding, shorter operating room (OR) time, and WIT, there is no general consensus that HALS is the preferred method for laparoscopic nephrectomy. We therefore set out to perform a systematic review of the literature and meta-analysis intended to compare the efficacy and safety of HALS vs open and laparoscopic/laparoscopic (Lap/Lap)-assisted surgical techniques when used in donor nephrectomy, nephrectomy, and nephroureterectomy procedures.
Methods
Procedures for this review followed established best methods for the evolving science of systematic review research. 6,7 A written prospective protocol defined the objectives, search criteria, study selection criteria, data elements of interest, and plans for analysis. A more global review was initially undertaken to examine the safety and efficacy of HALS in both general surgery and urologic abdominal procedures. The findings for the use of HALS in urologic procedures are presented.
Data sources
English language literature was searched from January 1, 1996 to October 26, 2007. A search was performed in MEDLINE database (via PubMed) using the following search terms: Hand-assist* OR hand assist* OR HALS or “lap* disc” OR gelport OR “pneumo sleeve” OR pneumosleeve OR “hand port” OR handport OR “omni port” OR omni-port OR intromit. Analogous searches were also performed in EMBASE, Current Contents,™ and the Cochrane library. A manual reference check of all accepted articles and recent reviews was also performed to supplement the above electronic searches and identify additional potentially relevant studies.
Study selection for data extraction
All study designs were accepted in the overall review, including randomized controlled trials (RCTs), prospective and retrospective nonrandomized comparator studies, and single-arm studies with no comparator. Studies were required to use HALS in at least 15 patients per treatment group and report efficacy and/or safety outcomes. Primary outcomes were blood loss, transfusions, surgery time, length of hospital stay (LOS), and number of patients needing conversion to open surgery. WIT was also of interest for donor nephrectomy procedures. All safety outcomes were captured at extraction, including mortality and perioperative complications.
Multiple publications of the same patient population were pooled as one study (kinship) to the extent possible to avoid double-counting patients. All eligible studies were rated for level of evidence at the time of data extraction using the Center for Evidence-Based Medicine, Oxford, UK, rating scale. 8 Protocol-defined data elements from each eligible study were extracted by one researcher onto a data extraction form, and confirmed by a second researcher, checking all extracted data against the original report. Differences were resolved before data entry. The data were then entered into a relational database of clinical studies, checked for accuracy, and exported for analysis.
While all study designs were accepted in the overall HALS literature review, the meta-analysis results are focused only on outcomes in studies that directly compared HALS with conventional (open) or Lap/Lap-assisted techniques in donor nephrectomy, nephrectomy, and nephroureterectomy procedures. This was necessary to analyze the comparative effects between the surgical approaches, which is not possible in single-arm studies in which no comparator is present.
Statistical methods
Basic descriptive statistics were used to summarize overall and procedure-specific study, patient, and treatment data. For baseline patient characteristics, the number of patients enrolled (or randomized) was used as a denominator. Efficacy, safety, and utilization outcomes were summarized for the HALS, conventional (open), and Lap/Lap-assisted groups, and stratified by surgical procedure. Comparative meta-analyses of selected efficacy and safety outcomes were performed using restricted maximum likelihood random-effects methods 7,9 between HALS vs open, and HALS vs Lap/Lap-assisted techniques. Outcomes of primary interest included: Transfusions, blood loss, OR/surgery duration, WIT, number of patients needing conversions to open surgery, and LOS. The meta-analyses results of continuous variables were expressed as mean differences and as odds ratios for binary outcomes with 95% confidence intervals (CIs). Meta-analyses of the binary variables were conducted on the log-odds ratios to satisfy the assumption of normality of effect sizes. All analyses were stratified by surgery type. Meta-analytic results are only reported when at least three treatment arms contributed data. The Q-statistic (Cochrane Q) was used to evaluate heterogeneity between studies, with P values less than 0.10 and 0.01 denoted. Statistical calculations were performed using SAS® software version 9.1 and SPSS® software version 15.0. Statistical significance of effect estimates was defined by a P value <0.05.
Results
Study attrition is detailed in Figure 1. The search yielded 2824 citations, of which 413 full articles were retrieved for further screening. The studies were further winnowed down to focus on 107 studies involving urology procedures that used HALS. An additional nine studies were excluded for having mixed procedures, in which the outcomes were not separable by type, or only reported cost outcomes. In addition, one study involved robot-assisted HALS, another evaluated a bilateral nephrectomy procedure, and two studies were about partial nephrectomies; all procedures and techniques that were not comparable enough to include with the procedures, we stratified for analysis.
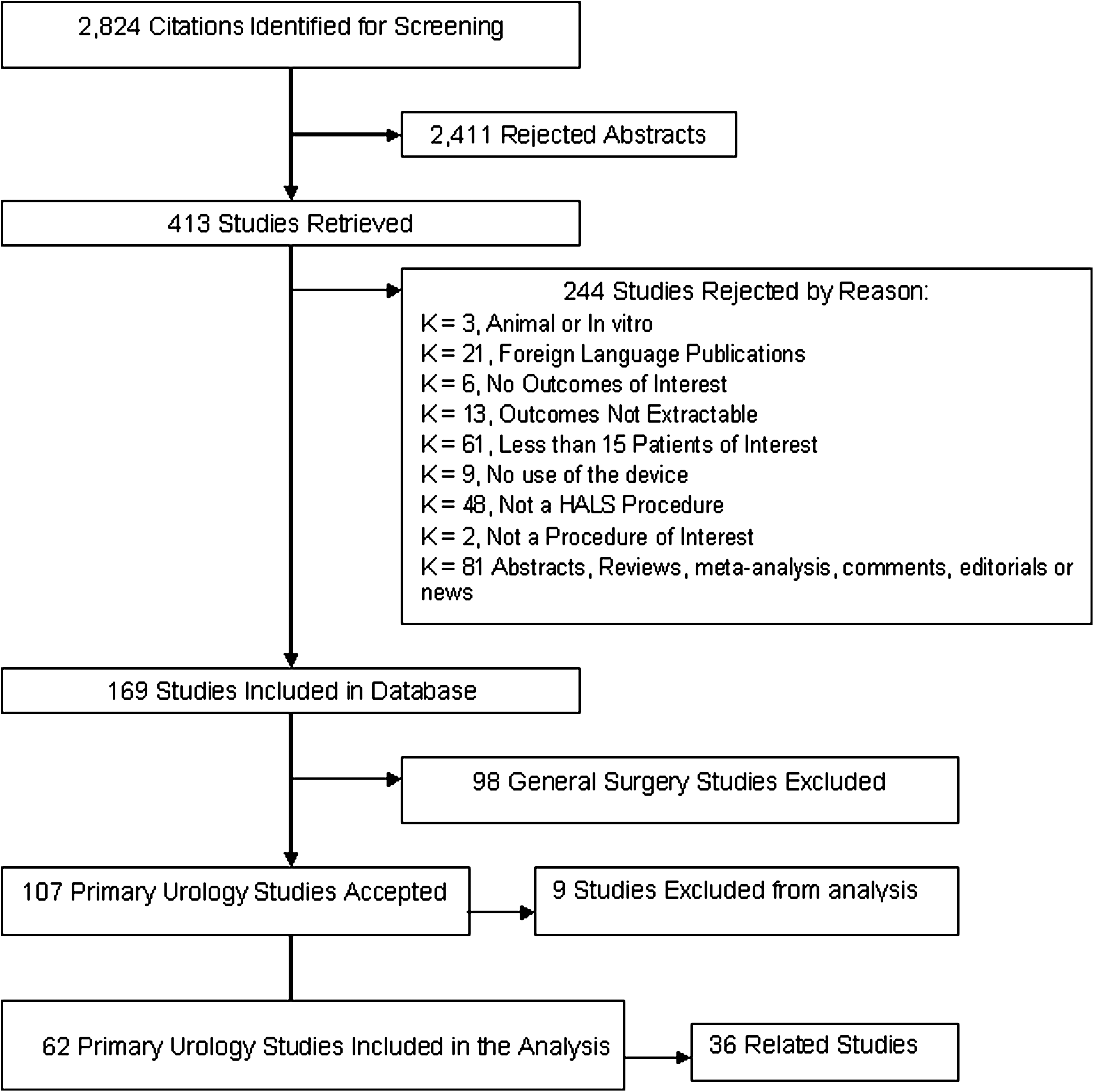
Study attrition.
Ultimately, 98 urology studies were included in the analysis, of which 62 were primary studies (k) with 121 treatment groups (t), enrolling 5466 patients (n); 36 studies involved the same or overlapping patient populations and were linked as related publications, to avoid double counting of participants at analysis (Table 1). Three of these studies reported more than one type of surgical procedure. 10 –12 Most of the studies were published after 2001 and were conducted in North America and Asia. The vast majority were from single centers (87%). Sixty percent of studies were prospective and retrospective nonrandomized comparator studies, 35% were single-arm studies with no comparator, and there was only one RCT. Thus, based on Center for Evidence Based Medicine criteria, 8 the majority of studies (92%) yielded only level III or IV evidence.
k=number of studies.
t=number of treatment groups.
N=number of patients in treatment group.
RCT=randomized control trial; nRCT=nonrandomized comparative trial.
Studies of 30 donor nephrectomy, 21 nephrectomy, and 14 nephroureterectomy procedures are included in the analysis with the majority comparing HALS with an open technique (k=28). Donor nephrectomy (k=19) and radical nephrectomy (k=12) studies were conducted predominately in North America, while nephroureterectomy studies were published solely in North America and Asia with each contributing an equal number of publications (k=7).
Patient demographic characteristics are summarized in Table 2. Patient characteristics were minimally described; however, for studies reporting mean age, the overall range was 31 to 73 years across 51 treatment arms. When baseline characteristics were not explicitly reported by treatment group, the authors did confirm that groups were statistically similar at baseline. Donor nephrectomy patients were typically younger than those undergoing radical nephrectomy or nephroureterectomy procedures with a nearly equal sex distribution among groups. Patients undergoing radical nephrectomy were predominately male, and patients undergoing laparoscopic procedures were older than those who underwent HALS or open procedures, 69.2 years vs 59.4 years and 58.9 years, respectively. Patients undergoing nephroureterectomy were older than those undergoing donor nephrectomy and radical nephrectomy procedures, with similar age and sex distributions across groups, with the exception of the laparoscopic group, which was predominately female. Body mass index was similar across treatment groups with an overall range of 21.5 to 38.7 kg/m2.
t=number of treatment groups.
N=number of patients evaluated.
n=number of patients with characteristic.
range of means.
HALS=hand–assisted laparoscopic surgery; lap=laparoscopic; BMI=body mass index.
Efficacy and utilization outcomes
From the available data, the efficacy and utilization outcomes for HALS, open, and Lap/Lap-assisted groups were summarized. The most commonly reported outcomes across all surgical procedures were length of OR/surgery time, blood loss, LOS, and transfusions. Meta-analysis results for HALS vs open and HALS vs Lap/Lap-assisted are presented in Tables 3 and 4, respectively. Trends and statistically significant findings for efficacy and utilization outcomes are described below for each procedure category.
t=number of treatment comparisons.
n=number of patients evaluated.
=P value for test of heterogeneity <0.01.
=P value for test of heterogeneity <0.10.
=statistically significant difference between HALS vs open.
HALS=hand-assisted laparoscopic surgery; M-A=meta-analysis; CI=confidence interval; OR=operating room.
t=number of treatment comparisons.
n=number of patients evaluated.
=p-value for test of heterogeneity<0.01.
=statistically significant difference between HALS vs laparoscopic.
HALS=hand-assisted laparoscopic surgery; M-A=meta-analysis; CI=confidence interval.
Donor nephrectomy. Blood loss was less in the HALS group when compared with both the open and Lap/Lap-assisted groups with a meta-analytic statistically significant (P<0.05) mean difference of −69.0 mL (95% CI, −129.7, −8.2) and −40.1 mL (95% CI, −68.2, 12.0) respectively. As might be expected, OR/surgery time was statistically significant in favor of open procedures when compared with HALS, with a mean difference of 31.5 minutes (95% CI, 12.5, 50.4); however, when compared with the Lap/Lap-assisted group, there was a statistically significant difference favoring HALS of −36.8 (95%CI, −61.3, −12.3).
While definitions of WIT were minimally reported in these studies, definitions were similar, and thus, data for WIT were pooled across all studies. When comparing HALS with open, WIT favored the open group, but the mean difference was less than 1 minute (0.7 min) (95% CI, 0.0., 1.4). WIT, however, favored HALS when compared with the Lap/Lap-assisted group, −1.26 minutes (95% CI, −1.83, −0.69).
Hospital LOS was shorter in the HALS compared with the open group with a statistically significant difference of −1.7 days (95% CI, −2.3, −1.1). The HALS group also had a shorter LOS when compared with the Lap/Lap-assisted group; however, this difference was not statistically significant.
Radical nephrectomy. Because of the paucity of Lap/Lap-assisted radical nephrectomy procedures, meta-analytic results were only possible for HALS vs open procedures. Trends in the data were the same as for donor nephrectomy procedures with blood loss and LOS statistically significant in favor of HALS, −232.9 mL (95% CI, −383.6, −82.2), and −2.4 days (95% CI, −3.5, −1.3), respectively. OR/surgery time was longer in the HALS group with a mean difference of 42.3 minutes (95% CI, 5.8, 78.7).
Nephroureterectomy. Meta-analytic comparisons were not possible for HALS vs Lap/Lap-assisted nephroureterectomy procedures. Statistically significant results for blood loss (−29.9 mL [95%CI, −242.3, 182.5]), and LOS (−1.5 days [95% CI −2.8, 0.3]) again favored HALS when compared with open procedures. OR/surgery time was statistically significant in favor of open procedure with a mean difference of 73.9 minutes (95% CI, 28.6, 119.2).
Safety outcomes
Data for mortality, perioperative, and long-term complications were sought from all studies. Reporting of these outcomes, however, was highly variable across studies and by each surgical procedure. In most instances, only a few treatment arms contributed to the data, and the number of patients with complications was small. Safety outcomes data for all comparator studies is presented in Table 5. Meta-analytic results were possible only for HALS vs open procedures (Table 6); however, the number of treatment arms contributing data is small, and there was no statistically significant difference in safety outcomes for these two groups.
t=number of treatment groups.
N=number of patients evaluated.
n=number of patients with characteristic.
as reported in studies that did not report specific safety outcomes.
HALS=hand-assisted laparoscopic surgery; Lap=laparoscopic; DVT=deep vein thrombosis; PE=pulmonary embolus.
t=number of treatment comparisons.
n=number of patients evaluated.
Includes related studies not included in primary baseline characteristics.
HALS=hand-assisted laparoscopic surgery; M-A=meta-analysis; CI=confidence interval; DVT=deep vein thrombosis; PE=pulmonary embolus.
Discussion
To our knowledge, this is the largest and most comprehensive systematic literature review and meta-analysis evaluating HALS for urologic renal procedures. Findings from this review support that HALS offers a significant (P<0.05) improvement in blood loss and LOS across all procedures when compared with open and Lap/Lap-assisted techniques. For donor nephrectomy, shorter WIT favored the open group, although this difference was not significant. HALS, however, was associated with a significantly shorter WIT when compared with the Lap/Lap-assisted group. OR time, as expected, was shorter in the open group across all surgical procedures compared with both HALS and Lap/Lap-assisted, but HALS was in favor when compared with Lap/Lap-assisted.
The mean difference in WIT and LOS when comparing surgical approaches is not clinically relevant, but the results indicate that for some patients, HALS may offer clinically relevant advantages. In six studies, the mean blood loss was 400 mL or more in the open group, and in four studies, it was >500 mL, ranging up to 1143 mL. Differences of this magnitude indicate that for some patients, the difference is not only statistically relevant but also clinically.
With respect to decreased blood loss, there are multiple possible explanations for this phenomenon. Tactile feedback provided by HALS may make dissecting out the renal artery and vein easier and safer, especially for surgeons in the learning phase or with limited experience, thereby decreasing inadvertent injuries to hilum vessels. HALS allows the surgeon to provide direct pressure to bleeding vessels with either hand or fingertips. The HALS device also offers a means by which one can use laparoscopic sponges as packing within the abdomen to potentially decrease blood loss. Severe sudden bleeding can also occur with experienced surgeons—for instance, with the malfunctioning of an endovascular stapler. 13 –15 There are numerous reports where the hand-assisted technique has been helpful in such situations. 16 –19 Bleeding is the most common reason for conversion to open surgery during a procedure, and reoperation can be difficult to manage using laparoscopic instruments alone. 15,19,20
In this review, there were significantly more conversions in the LAP/Lap-assisted group compared with HALS for donor nephrectomy in trials that compared the two surgical approaches (Table 4). This indicates there is a clinically relevant difference in favor of HALS, compared with HALS for donor nephrectomy. The results of the meta-analysis, however, were not statistically significant.
LOS was shorter in the HAL group compared with both the open and laparoscopic cohort. Smaller incisions, placed lower on the anterior abdominal wall, which do not transect muscle, can account for less trauma leading to decreased postoperative pain and decreased LOS compared with the open cohort. It is unclear why LOS was decreased compared with the standard laparoscopic group. One possible explanation is that a decrease in OR time may indirectly lead to a decrease in hospital stay. This study did note a significant decrease in operative time with HALS compared with standard laparoscopy. The shorter operative time achieved with HALS compared with Lap/Lap-assisted can also be important relative to the potential for long-lasting discomfort and/or severe complications, such as neuromuscular injuries and rhabdomyolysis from the somewhat awkward patient positions needed for these procedures. 20 –24 Although speculative, longer anesthesia times necessitate increased analgesics and narcotics at the time of surgery, which may lead to delayed postoperative ambulation, increased ileus, and thus a longer LOS.
For donor nephrectomy, shorter WIT favored the open group, although this difference was not significant. HALS, however, was associated with a significantly shorter WIT when compared with the Lap/Lap-assisted group. For donor nephrectomy, preserving the integrity of the kidney and optimal kidney function are crucial. A less traumatic handling of the kidney and shorter WIT can be achieved in HALS compared with Lap/Lap-assisted techniques. The long-term clinical significance of decreased warm ischemia is debatable; however, few would argue that decreasing warm ischemia and manipulation is preferable when possible.
While well-designed RCTs provide the most rigorous evidence, there is an overall lack of RCTs in the surgical setting and, in this review, only one RCT was identified. Given the lack of available studies with randomized designs, all comparative studies were included in the meta-analysis. Despite this limitation, the findings remain valid and provided statistically significant results for several outcomes of interest.
Another limitation was the high incidence of studies with small sample sizes. Among the included studies, the number of patients enrolled ranged from 20 to 553, with the majority of the studies (67%) enrolling fewer than 100 patients and only one large study 25 evaluating 553 patients. The evidence we present in this review would be strengthened with the addition of more large randomized trials comparing HALS vs other surgical techniques.
Conclusion
The findings of this systematic review and meta-analysis indicate that HALS allows for a significant decrease in blood loss and LOS when compared with open surgery in donor nephrectomy, nephrectomy, and nephroureterectomy procedures. When compared with standard laparoscopic donor nephrectomy, HALS resulted in a significant decrease in blood loss, OR time, conversions, and WIT. Although the mean difference may not be of clinical relevance, for some patients, HALS may offer significant clinically relevant advantages, such as avoidance of major blood loss.
Footnotes
Acknowledgment
Funding for the systematic literature review was provided by Ethicon Inc.
Disclosure Statement
United Biosource Corporation employees acted as consultants for Ethicon Inc. For the other authors, no competing financial interests exist.