
Abstract
Robot-assisted surgery is becoming more widespread, but despite adoption by most academic institutions, curricula for training residents in robotics have yet to be developed fully. Even after teaching surgeons have mastered robotic techniques, an inherent risk of avoidable injuries may persist as they seek to impart their knowledge of this relatively new surgical modality to trainees. Two cases of aortic injury during access for robot-assisted prostatectomy are described along with their successful robotic repair with root-cause analysis of the events. Robotic surgeons who are involved in training programs should be prepared to handle even major potential complications of robot-assisted surgery regardless of their own expertise or experience.
Case 1
A 57-year-old man was positioned in a steep Trendelenburg poition for robotic-assisted laparoscopic prostatectomy (RALP). Veress needle insufflation was performed, and all ports were placed under laparoscopic guidance per routine. The robot was then brought into position and secured to the ports. The surgeon placed the two left-sided robotic instruments, but during simultaneous placement of the right-sided robotic scissors by a fourth-year resident, resistance was noted and reported to the surgeon. The angle of entry of the instrument was seen to be too acute such that the instrument was removed and reinserted by the surgeon.
On sitting at the robotic console, blood was seen on the tip of the robotic scissors even before any dissection had been performed. The robotic camera was used to survey the abdomen, which revealed brisk bleeding from the retroperitoneum (Fig. 1). The initial suspicion was of mesenteric artery injury, because the source of bleeding was constant and bright red but did not appear initially to be of high pressure. Dissection through the retroperitoneal fat beginning at the puncture defect led to more extreme bleeding under high pressure but without a discernible direction.
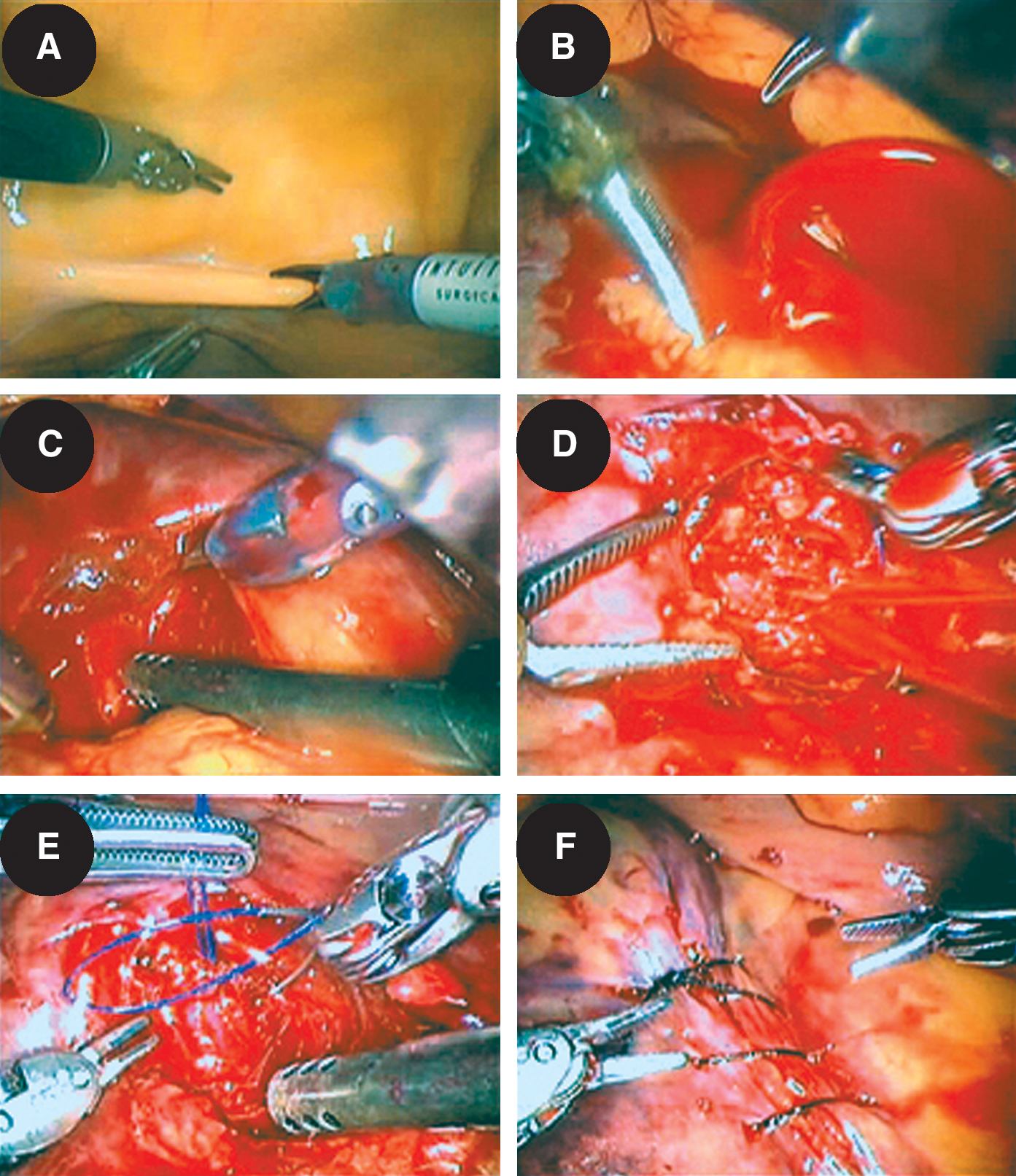
Intraoperative images from aortic injury and repair, including
Suspicion of aortic injury as the source based on flow alone led to attempts to tamponade the bleeding for temporary control with the robotic instruments but without success because of the overlying fatty tissue dissipating applied pressure. It was then decided to quickly separate the fat bluntly until the aortic wall itself was reached, thereby allowing direct pressure to stop the bleeding.
After this allowed successful temporary control, a polypropylene suture was then quickly placed and held on tension with the robotic fourth-arm instrument to allow further dissection to delineate the edges of the aorta. Controlled suture repair was then performed for a definitive closure. Silk suture was used to reapproximate the posterior peritoneum over the repair.
Given the estimated blood loss of approximately 1L over the course of less than 5 minutes, the decision was made not to proceed with the prostatectomy in the event an unexpected amount of bleeding might be encountered during that procedure. The patient was therefore admitted for observation with routine robot-assisted prostatectomy performed the following day.
The patient was discharged on the first postoperative day per routine without further complications now more than 2 years later.
Case 2
More than 1 year later, a 74-year-old man with local recurrence of prostate cancer after external beam radiation therapy was positioned in a steep Trendelenburg position for salvage RALP after external beam radiation. An incision was made just left of the umbilicus for Veress needle insertion per routine. The Veress needle was inserted by a fourth-year resident with brisk return of blood from the needle's hub. The needle was immediately removed by the surgeon, and the Hasson technique was used to gain access to the peritoneum in less than 1 minute. On entering, no free peritoneal blood was identified such that it was decided to quickly place a 12-mm port and insufflate the abdomen for visualization of the source of the bleeding initially identified. Insufflation was set at 20 mm Hg temporarily because the bleeding from the Veress needle had not been pulsatile or bright red, so that a venous source was suspected first. A retroperitoneal hematoma was then identified with the laparoscope and inspected for expansion while deciding whether to perform laparotomy.
Because the hematoma appeared stable and the patient remained clinically unchanged, the decision was made to proceed with investigation of the hematoma robotically without open conversion. After placing all ports and docking the robot, the site where the Veress needle had punctured the posterior peritoneum overlying the hematoma was identified and used to guide careful dissection through the hematoma with the robotic instruments. Although aortic injury had not yet been suspected based on the nature of the initial blood return and stability of the hematoma, separation of the retroperitoneal fat overlying the aorta revealed that the injury had indeed been to the aorta. On clearing the overlying retroperitoneal fat, bleeding restarted from the puncture area, but given the small size of the puncture, a robotic instrument was able to tamponade bleeding while clearing the aortic surface for repair with polypropylene suture. The posterior peritoneum was then closed over the repair once completed. Given that the blood loss had been contained by formation of the hematoma with no clinical effect on the patient's vital signs throughout, the decision was made to proceed with the salvage RALP, which was completed uneventfully. The patient remained stable throughout his hospital admission and was discharged on postoperative day 1 per routine without further complications.
Discussion
Robot-assisted prostatectomy has become a common procedure in the United States. 1 While high-volume and extensively experienced surgeons may regard RALP as a routine procedure, it remains major abdominal urologic surgery and carries real risks of serious complications. At our institution, robot-assisted laparoscopic surgery is performed with active participation by residents of various training levels and exposure to robotic procedures. In general and in this setting in particular, surgeons should not minimize the critical nature of even the most routine portions of any surgical procedure.
The first step of any laparoscopic procedure is gaining access for creation of pneumoperitoneum. The two prevalent techniques include direct access by way of controlled incision using the Hasson technique and placement of the Veress needle using tactile cues in the absence of direct vision. 2 Complications that arise from this method of access occur in up to 0.25% of cases with major vascular injury accounting for only 8% of these complications. 3 While the Veress needle injury reported here was to a major vessel, it has not changed the technique used at our institution, given that it occurred only once in more 1000 RALP procedures performed by the surgeon using the Veress needle routinely in all cases.
In addition to establishment of pneumoperitoneum to create the working space, robot-assisted surgery also requires that the robot be docked and instruments placed before the procedure is begun, steps that are again subject to minimization by an experienced surgeon because of their routine nature. While aortic injuries from the Veress needle or even port placement have been reported for other laparoscopic procedures, 3 the injuries reported here that occurred with robot-assisted surgery as well as their repair robotically are, to our knowledge, unique. As with any major iatrogenic injury, reporting and root-cause analysis are both important to avoid future similar occurrences and to educate others on prevention.
Our analysis of the events revealed several modifiable risk factors and teaching points. In the instance of the first injury involving advancement of the robotic scissor instrument through the aorta, immediate review by the surgical team and later in departmental monthly morbidity review conference identified multiple contributing factors. While the surgeon involved was extensively experienced with robot-assisted surgery, the event occurred during only his second procedure at the institution after relocating from another teaching hospital. Therefore, the surgeon was unaware of the experience level of each resident in the program and mistakenly made an assumption regarding the amount of robotic training residents obtained before his joining the institution.
In addition, key aspects of access and docking techniques varied between the previous surgeon and the surgeon involved. These included that the previous surgeon instructed residents to use the robotic camera to visualize instruments being placed into the abdomen. While this in general is good practice, especially for trainees, many surgeons who are experienced in robotics and particularly in laparoscopy do not continue to do this once they become comfortable with directionality in the laparoscopic environment and with the tactile forces involved. The resident involved observed the surgeon doing so as he had been trained and had done hundreds of times and attempted to do the same with only minimal such experience. He therefore misjudged the angle of entry of the instrument and did not recognize the improper amount of force applied in advancement of the instrument believing that the robot would prevent overshooting as it does on subsequent instrument changes once unclutched.
After this first event, several measures were taken to prevent a similar occurrence. Immediate measures included taking inventory of each resident's experience with robotic procedures and increased supervision of less-experienced residents during even mundane tasks. Next, a dry-lab and didactic laparoscopy training curriculum was instituted and contributed to by other members of the faculty who were performing laparoscopic procedures. The more experienced chief residents then began instructing lower level residents in assisting from the bedside before transitioning to the console, where they would rely on these more junior residents themselves for assistance. Finally, a concerted effort was made on the part of the teaching faculty and residents to increase the level of resident participation in robotic procedures because previously, physician assistants and fellows had inadvertently restricted their role. Since then, a physician assistant has been reintroduced at the bedside but has been instrumental in training new residents in bedside assisting.
Root-cause analysis of the Veress needle injury (second event) revealed unexpected contributing factors. Given that the two events were more than 1 year apart, there was no lack of laparoscopy training on the part of the resident or inadequate estimation of experience on the part of the surgeon. Nevertheless, despite adequate training and supervision, the Veress needle was inadvertently placed into the aorta, underscoring how such injuries can occur in seconds even with the surgeon standing across the table and observing the resident throughout.
One of these contributing factors was the patient's body habitus as the resident continued to advance the needle waiting for the second click, which was never felt because the patient was extremely thin. As in other such patients where the preperitoneal fat may be minimal or nonexistent, the two clicks of the Veress needle typically encountered on traversing the fascia and then peritoneum were one, given that both layers were essentially contiguous. Because the resident had been taught to listen for two clicks, he did not realize his depth of penetration until the return of blood.
The second factor involved was the trajectory of needle insertion, because the surgeon routinely places the patient in a steep Trendelenburg position even before draping the patient to ensure that there is no slipping that would necessitate repositioning before starting the procedure. This places the abdomen at an angle, which the surgeon accounts for by angling the Veress needle from the insertion point at the umbilicus toward the pelvis and not straight down. When the needle is inserted perpendicular to the ground, it is actually angled toward the head from the patient's perspective and therefore in the direction of the aorta, rather than beyond its bifurcation in the pelvis. The surgeon had not emphasized this previously, but it has become a routine teaching point when instructing residents in access since this incident.
By presenting these complications and their management, we hope to prevent similar occurrences at other teaching institutions or elsewhere. We certainly do not present these complications to advocate that all such injuries be managed in similar fashion. As stated, the surgeon involved had performed hundreds of robotic procedures before these complications and had performed robot-assisted aortic surgery in a porcine model as well as robotic repair of vascular injuries occasionally encountered during pelvic and retroperitoneal lymphadenectomies. In addition, the surgeon may be more comfortable with vascular surgery than some, given that he had previously performed renal transplantation and other vascular surgery, such as vena caval tumor thrombectomy routinely before dedicating his practice to robot-assisted surgery.
While the decision to convert to open surgery should never be criticized, it is a complicated decision that can only be made by the surgeon with individual patient and surgeon factors playing a greater role in whether to convert than the type or severity of an injury alone. On occasion, conversion to open surgery can exacerbate bleeding by releasing pneumoperitoneum, and gaining control of bleeding after conversion to open surgery is not always expeditious itself. Some may feel that all such injuries should always be managed with open surgery, but such attitudes may change as we enter an era of surgeons equally or even more comfortable with robotic than open surgery.
Conclusions
Unexpected major vascular injuries can occur during access for minimally invasive surgery, but although conversion to open surgery was certainly justified, robotic instrumentation allowed repair in the two cases presented. Root-cause analysis of these aortic injuries has lessons for surgeons who are involved in training programs, who should be prepared to handle any potential complications of robot-assisted surgery no matter how severe and should be vigilant during even the most mundane portions of any operation.
Footnotes
Disclosure Statement
No competing financial interests exist.