
Abstract
Background and Purpose:
Real-time tomographic reflection is a novel technique that uses a geometrically fixed arrangement of a conventional ultrasound transducer, a transducer-incorporated monitor, and a half-silvered mirror. This device, dubbed the Sonic Flashlight, generates a virtual anatomically scaled image, obviating the need for a separate monitor. It may therefore facilitate invasive procedures, such as percutaneous access to the kidney. This proof-of-concept study assesses the feasibility of this technique for renal imaging and concomitant needle puncture guidance.
Materials and Methods:
In a swine model with induced hydronephrosis, the Sonic Flashlight was used to visualize and guide needle access to the renal pelvis. Passage of a 7-inch, 18-gauge spinal needle was performed. Entry into the collecting system was confirmed by the aspiration of urine.
Results:
The anechoic renal pelvis and hyperechoic needle tip could be seen with the Sonic Flashlight device. Successful access to the collecting system was obtained twice without dificulty. The sonographic image, appearing to emanate from the tip of the transducer, makes visualization and manipulation more intuitive. Furthermore, by placing the operator's eyes and hands in the same field as the sonogram, image-guided procedures are potentially easier to learn.
Conclusion:
The relatively shallow depth of penetration of the current device limits its clinical usefulness. A new Sonic Flashlight with a greater depth of penetration is in development.
Introduction
Some researchers addressed this dilemma by exploring less conventional ways for viewing ultrasonographic images. One example is the development of head-mounted display (HMD) systems, which successfully tie the image, the patient, and the operator's hands in the same field. 1 These systems, however, are often cumbersome in size, low in resolution, limited in field of view, and costly. Furthermore, multiple observers of the procedure would each need their own HMD, increasing costs even more.
To address the advantage of having the operator's hands and eyes within the same environment as the image and concomitantly minimize cost, real-time tomographic reflection (RTTR) was created. 2,3 RTTR uses ultrasound technology, a transducer-mounted monitor, and a half-silvered mirror, all fixed in relative geometry, to create an anatomically scaled image that appears to emit from the tip of the probe. Appropriately called the Sonic Flashlight, this device produces virtual images that can be projected in situ anywhere on the body, thereby facilitating image-guided procedures because the operator does not need to look away from the patient. Several clinical and feasibility studies have already shown its ability to ease placement of venous or arterial catheters, localize brain lesions, and guide retrobulbar optic nerve blocks. 4 –6 Urologic applications for the Sonic Flashlight have not yet been explored.
In urology, conventional ultrasound is regularly used for diagnostic and therapeutic purposes. In pregnant women and children, ultrasonography (the imaging modality of choice because it is nonionizing) is often used to look for stones, assess for signs of obstruction, and follow disease processes such as hydronephrosis. Ultrasound is also used for renal biopsies, percutaneous ablation of renal tumors, and placement of nephrostomy tubes, although fluoroscopy is also commonly used to access the renal collecting system.
With the prevalence of sonography in urology, determining the feasibility of the Sonic Flashlight in urologic procedures is a natural extension of the device. The goals of this proof-of-concept study are to assess the ability of the Sonic Flashlight to visualize the renal pelvis and aid in its access for percutaneous procedures.
Materials and Methods
Animal experimentation protocols used in this study were approved by the Animal Care and Use Committee and the Institutional Review Board of the University of Pittsburgh.
Sonic Flashlight prototype
The Sonic Flashlight prototype has three key components: a conventional ultrasound system (Terason 2000; Teratech, Burlington, MA), a half-silvered mirror with 30% reflectance (Edmund Optics, Barrington, NJ) custom cut to meet specific dimensions (25×50×2 mm), and a light-emitting display monitor (OLED; AM550L; Kodak, Rochester, NY) measuring 44×33 mm, all of which are specifically arranged as shown in Figure 1. Because the monitor is 44 mm, the maximum depth of visualization is 4.4 cm. The ultrasound probe is custom-fitted with this display, and a disposable frame holds the mirror in place (Fig. 2). Of note, the OLED monitor is ideal because it is lightweight and has excellent off-angle viewing quality.
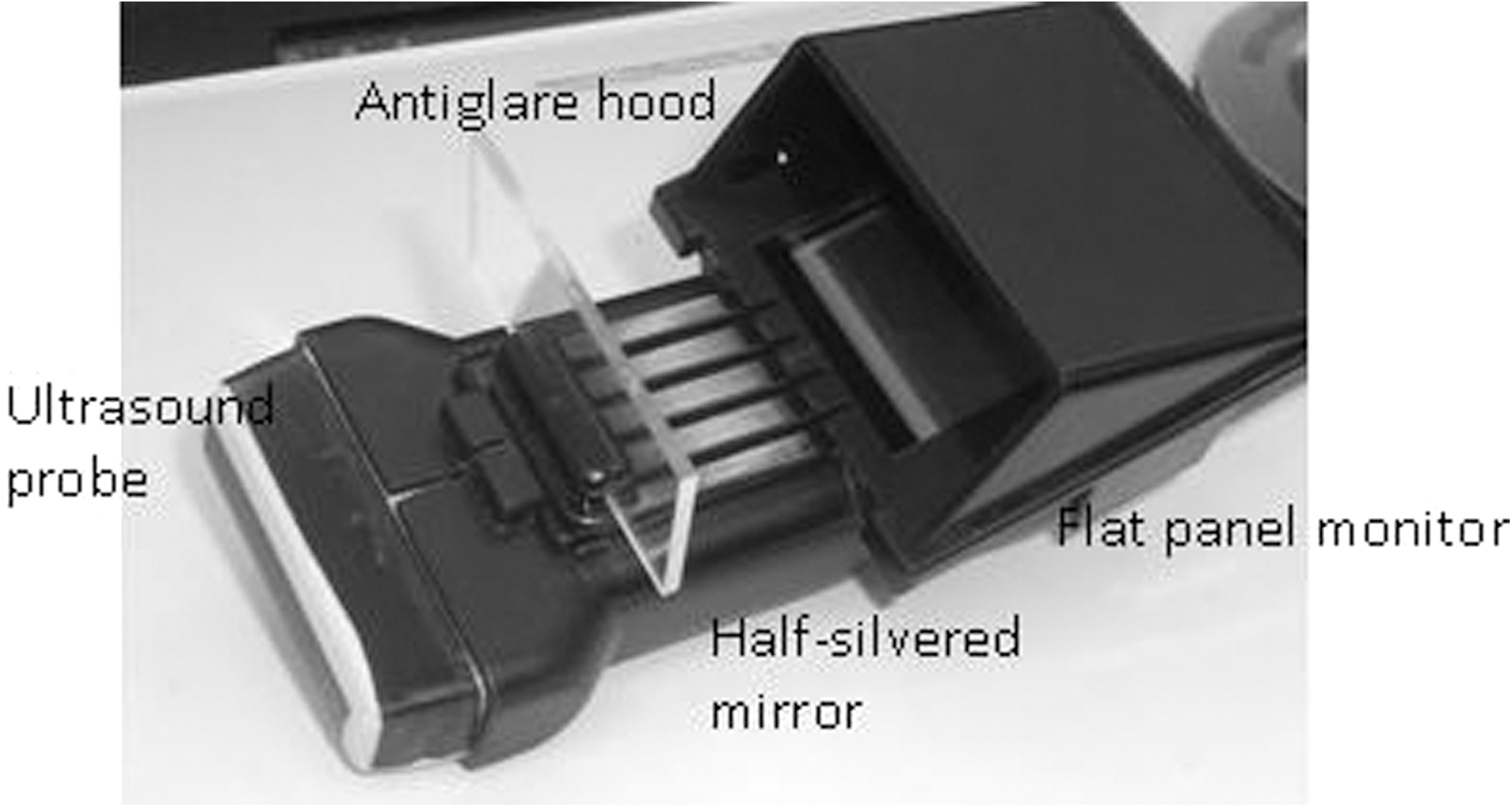
Components of the Sonic Flashlight. The ultrasound probe, the probe-mounted monitor, and the half-silvered mirror are fixed by a disposable frame. There is an antiglare hood over the monitor.
Experimental setup
The experiment was conducted in a swine model anesthetized with the induction drug ketamine (10 mg/kg intramuscular injection, one-time dose) and maintenance agent isoflurane (1% continuous). The animal was placed in the left lateral decubitus position. A Veress needle was then introduced in the right upper quadrant to insufflate the abdomen, followed by the placement of laparoscopic ports. The right kidney and ureter were identified, and the ureter was dissected free and subsequently occluded with two staples. The abdomen was then desufflated by opening the ports.
Accessing the renal pelvis
A urologist with no previous experience with the Sonic Flashlight was instructed on its usage for 5 minutes before percutaneously accessing the right renal pelvis. The Sonic Flashlight was then situated on the animal's right flank to attempt imaging the renal pelvis. The 7-inch, 18-gauge spinal needle was subsequently directed toward the region of the sonographic image that appeared to be the renal pelvis. An empty syringe was attached to the needle to aspirate urine if present.
Results
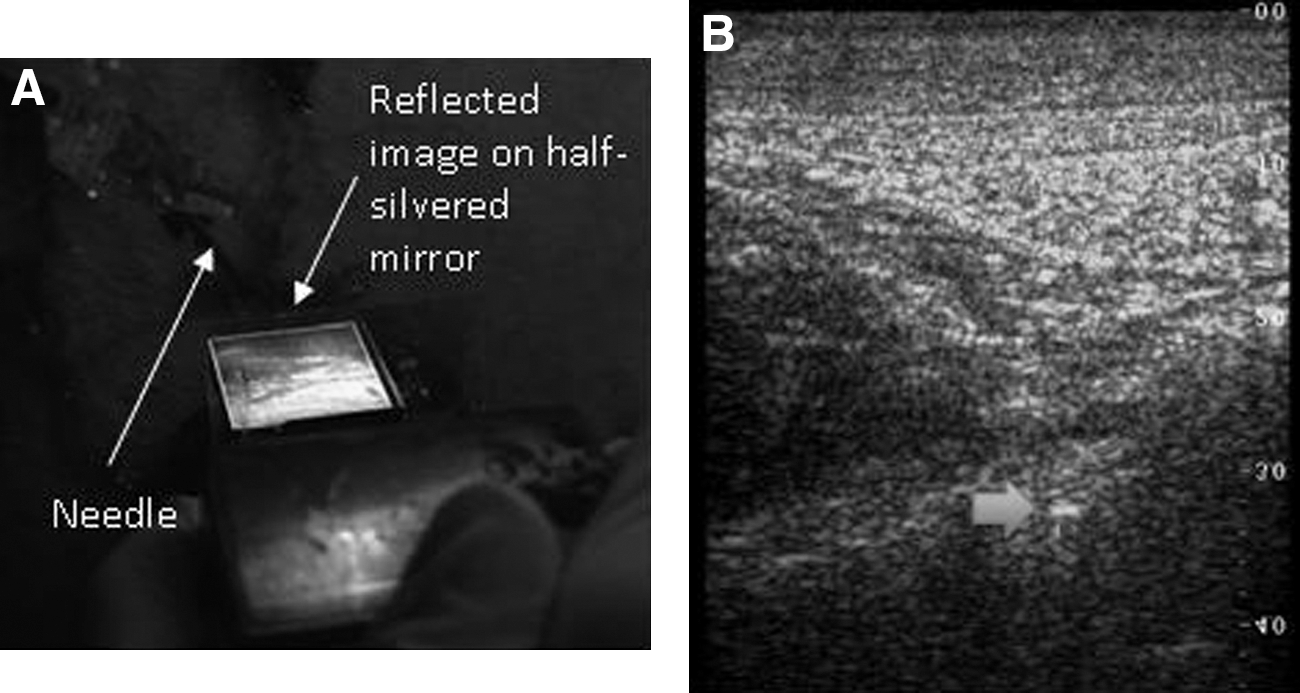
With the use of the Sonic Flashlight, the anechoic renal pelvis was visualized at its expected location seemingly within the animal in anatomic scale (Fig. 2). The needle was inserted directly at the renal pelvis image outside the plane of the RTTR tomographic slice. Therefore, the needle was not sonographically seen until it entered the plane of the virtual image slice. In this fashion, the renal pelvis was accessed on two of two attempts, confirmed by visualizing the hyperechoic needle in the anechoic renal pelvis and by aspirating urine. Anecdotally, the operator thought the device was intuitive and easy to use, but that the image was much smaller than traditional ultrasound machines. The Sonic Flashlight was easiest to use when the operator also inserted the needle.
Discussion
Real-time tomographic reflection integrates the operator's view with the sonographic image, nullifying the disjointed experience of performing a procedure while looking at a monitor away from the region of interest. The Sonic Flashlight uses RTTR to take advantage of natural hand-eye coordination in facilitating various procedures. Multiple proof-of-concept studies with this device have shown its ease of use and its success in targeting veins, arteries, optic nerves, and brain lesions. 4 –6 Clinical studies currently include image-guided placement of peripherally inserted central catheter venous access lines. 7 Future directions include other percutaneous procedures such as breast biopsies and nephrostomy tube placement.
In our preclinical study, we hypothesized that the Sonic Flashlight could be useful for accessing the renal collecting system. Although initially difficult to visualize the kidney secondary to the device's shallow 4.4 cm depth of visualization, the renal pelvis with iatrogenically induced hydronephrosis was eventually found and easily accessed with the spinal needle. Because the Sonic Flashlight produces a virtual anatomically scaled image in real time, there was a great degree of freedom in placing the needle, unlike ultrasound probes with fixed needle tracts. This made percutaneous access less restricted and more intuitive as the needle was aimed directly at the image. This method did not sonographically show the hyperechoic needle throughout its course as placing the needle in the plane of the image would have, but by separating image and needle, small adjustments during needle passage could be made with ease. Keeping the needle in the image plane is an option with the Sonic Flashlight.
The main limitation of the current model of the Sonic Flashlight is its shallow depth of penetration, because this model was designed for vascular access and not for kidneys. This made locating the kidney with the current model somewhat more difficult, but induced hydronephrosis facilitated localization of the anechoic renal pelvis. A Sonic Flashlight with a larger screen and greater depth of penetration could certainly be built. Another limitation was the small image compared with the magnified images on conventional machines. This feature could not be addressed, because magnification of the image would distort the anatomic scale inherent to the device. Nevertheless, the Sonic Flashlight guided access to the renal pelvis in our animal model, although it is not yet ready for clinical urologic trials because of its limitations.
Conclusion
The Sonic Flashlight successfully visualized and guided access to the renal collecting system. The sonographic image, appearing to emanate from the tip of the transducer, makes visualization and manipulation more intuitive. The relatively shallow depth of penetration of the current device limits its usefulness, however. A Sonic Flashlight with a greater depth of penetration is currently in development.
Footnotes
Disclosure Statement
No competing financial interests exist.