
Abstract
Flexible nephroscopy while using carbon dioxide to insufflate the collecting system has been described as a “good trick” to remove caliceal stones during laparoscopic pyelolithotomy. We found this true only for those calices with undisturbed urine drain into the renal pelvis, while it provided suboptimal view of stones that were located in dependent lower pole calices. We describe how we dealt successfully with a group of lower pole caliceal stones during laparoscopic pyeloplasty.
Problem
The use of irrigation during the nephroscopy phase may represent a serious drawback to this technique, because large amounts of fluid are collected in the peritoneal cavity, which is hard to remove intraoperatively and may produce postoperative ileus, obscure, or even give the false sensation of anastomotic leak as a larger than usual amount of fluid comes out through the drain during the first postoperative days.
Mason and associates 2 recently described the technique of carbon dioxide (CO2)-based nephroscopy during laparoscopic pyelolithotomy. The advantage of this interesting and novel technique is evident, because it avoids unnecessary irrigation of the abdomen and prevents vision impairment that may occur with the interface of a liquid and the carbon dioxide gas used to establish pneumoperitoneum.
We report our experience with this technique in a patient with UPJO and multiple lower caliceal stones.
Technique
A right laparoscopic pyeloplasty and flexible nephroscopy were performed in a 56-year-old woman with the diagnosis of right UPJO according to clinical and radiologic parameters. A preoperative CT showed hydronephrosis and a calcified 1.5 cm mass inside a lower calix, being unable to differentiate between a single and multiple small stones. Both laparoscopic and endoscopic carts were prepared. The patient was placed in a 60-degree flank position, and four laparoscopic ports were placed as follows: 11 mm at the umbilicus for the camera, 12 mm lateral to the rectus muscle two fingers below the costal rim, 5 mm below the xiphoid process for liver retraction, and a 5 mm port lateral to the rectus muscle at the umbilicus level for the surgeon's left hand.
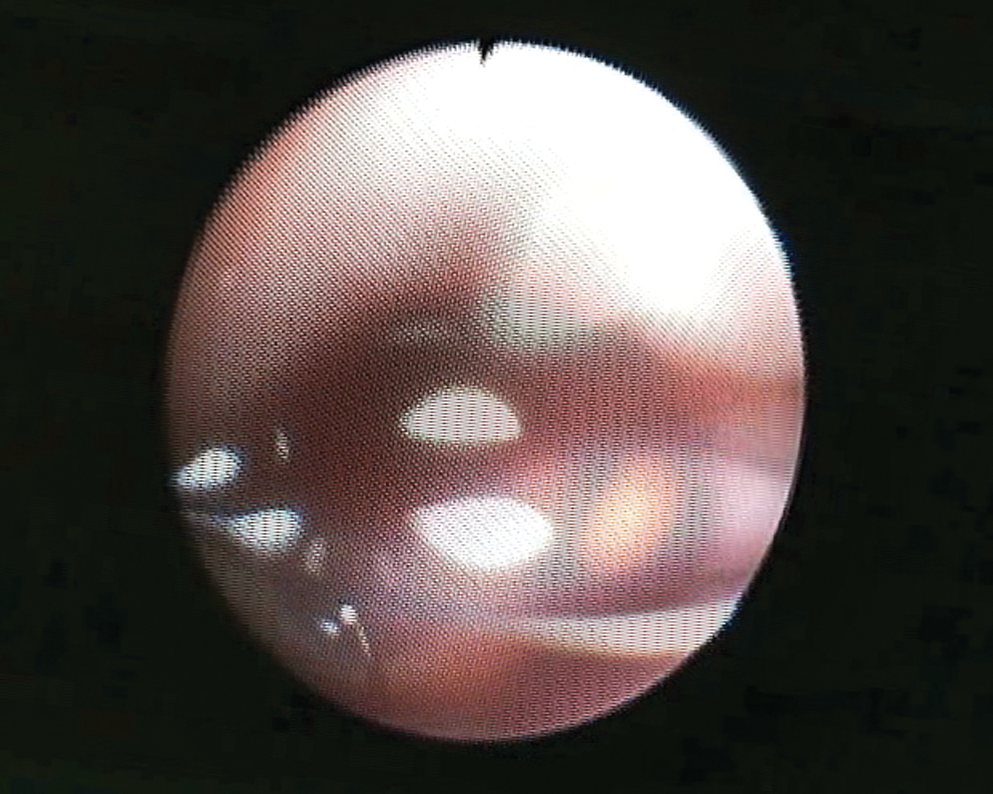
The ascending colon was reflected medially; the renal pelvis was dissected and incised with cold scissors after placement of a stay suture. Urine was aspirated from inside the kidney, and a flexible nephroscope was inserted inside the renal pelvis through the 12-mm port. As described by Mason and colleagues, 2 the CO2 cannula was removed from the laparoscopic port and inserted through the irrigation channel of the flexible nephroscope. Once the renal pelvis was filled with air, we found an excellent view of it and of those calices, mainly anterior ones, in which anatomic configuration with respect to the patient position allowed undisturbed urine drain into the renal pelvis (Fig. 1).

Excellent view of all nondependent calices was achieved with carbon dioxide nephroscopy.
Stones that were located inside any of these calices would have been taken out easily with nitinol baskets with an excellent view. We found, however, that stones located in a dependent calix that does not naturally drain into the renal pelvis with the patient lying in the flank position were hard to identify clearly. Constant production and accumulation of urine in these calices after removal of the obstruction created an air-water interface with the CO2 coming through the nephroscope, producing large amounts of bubbles and obscuring vision. We were not able to effectively basket stones in this setting (Fig. 2).
Identification of lower caliceal stones while on CO2 nephroscopy was suboptimal because of water-gas interface and constant presence of bubbles.
To overcome this difficulty, we decided to bring back the CO2 cannula to the laparoscopic port and replace it with a 50 mL Luer Lock syringe with saline that was connected to the irrigation port of the nephroscope (Fig. 3). Small pushes by the assistant were enough to precisely identify, trap, and remove stones (Fig. 4) with minimal irrigation until all of them were taken out. Some tiny ones were just aspirated with the laparoscopic suction probe gently placed at the infundibulum of the lower calices, while some others that were embedded in blood clots were removed with an ordinary laparoscopic grasper (Fig. 5).

The CO2 insuflator is brought back to the laparoscopic port. A lock adaptor with a 2 way stopcock is connected to the nephroscope working channel and used to introduce working elements such as nitinol baskets. One side of an extension tube is connected to the stopcock and the other to a 50 mL Luer Lock syringe filled with saline.

Small pushes of saline were enough to obtain an excellent view, allowing extraction of lower pole stones.

A regular grasper was used to remove stones that were embedded in a blood clot.
Footnotes
Disclosure Statement
No competing financial interests exist.