
Abstract
Purpose:
Increasing diagnosis of small renal masses (SRMs) necessitates trainees to be familiar with available therapies. We hypothesized that involvement in conservative treatments (ablation and/or active surveillance) occurs infrequently. Therefore, we evaluated resident exposure and participation in treatments as well as proposed management for SRMs.
Methods:
A survey was distributed to residents of the American Urologic Association and queried exposure to ablation and surveillance for SRMs. Three case scenarios (SRM in a healthy 55-year-old, healthy 75-year-old, and comorbid 75-year-old patient) were presented for management.
Results:
Two hundred fifty-seven residents responded to the survey. Two hundred thirty-four (91%) reported ablation was offered at their institution, although only 140 (54%) ever participated in this procedure. Of these, 80 (57%) were involved in fewer than five procedures. Experience with ablation did not increase at higher levels of training (U3-61%, U4-66%, and U5-63%). Two hundred twenty-four (87%) residents noted exposure to surveillance for managing SRMs, increasing from 70% in U1 to 94% in U5. When considering case scenarios, management strategy shifted significantly from extirpation to ablation or surveillance as patient age and comorbidity profile increased. In particular, almost 50% of respondents advocated ablation for SRMs in a comorbid 75-year-old patient.
Conclusions:
Although most residents are adequately exposed to surveillance strategies for SRMs, only 54% participated in an ablative procedure. Nonetheless, almost 50% of residents recommended ablation to manage SRMs in the aging, comorbid patient. This suggests a disconnect between training and future practice pattern.
Introduction
A central tenet of urology training involves providing a knowledge and skill set that is sufficient to allow implementation into future practice. 12 Urology residency training has classically included exposure to extirpative renal procedures, including nephrectomy or partial nephrectomy, via either an open or minimally invasive approach. With the evolution to less invasive therapies for SRMs, one questions if residency training accurately reflects these inherent changes in practice environment. In 2006, Duchene and colleagues 12 reported survey results from 372 urology residents and noted that laparoscopic and percutaneous needle renal ablation was performed in only 51% and 63% of respondent institutions, respectively. Further, at that time, 69% of residents indicated that laparoscopic radical nephrectomy was the gold standard for managing renal cancers.
On the basis of these data, we questioned whether current residency training provides urology trainees adequate exposure to less invasive (thermal ablation) or noninvasive (active surveillance) therapies for managing SRMs. To better address this, we evaluated via a survey instrument resident exposure and participation in various treatments as well as their proposed management strategies for SRMs.
Materials and Methods
In January 2009, all residents-in-training as listed in the American Urological Association (AUA) access directory were contacted by electronic mail (e-mail) and were asked to complete an online survey. The survey was circulated for 90 days by a commercially available Internet-based survey company (
Residents were queried regarding level of exposure and participation in thermal ablative procedures (cryoablation or RFA) and active surveillance regimens for managing SRMs. Additionally, residents were presented with three case scenarios regarding management of SRMs. All three patients were presented with the diagnosis of a 2.5 cm incidental enhancing left renal mass that was partially exophytic in nature and located on the lateral aspect of the kidney. The differentiating factor in the three case scenarios was patient age and health status. Specifically, patients were described as follows: (1) a healthy 55-year-old man with normal renal function; (2) a healthy 75-year-old man with normal renal function; and (3) a 75-year-old man with hypertension, diabetes, and coronary artery disease, although with normal renal function. Available treatment options presented to the respondents included nephrectomy (open/laparoscopic), partial nephrectomy (open/laparoscopic), thermal ablation (RFA/cryoablation via laparoscopic or percutaneous approaches), or observation with serial imaging. The distributed survey is shown in Figure 1.
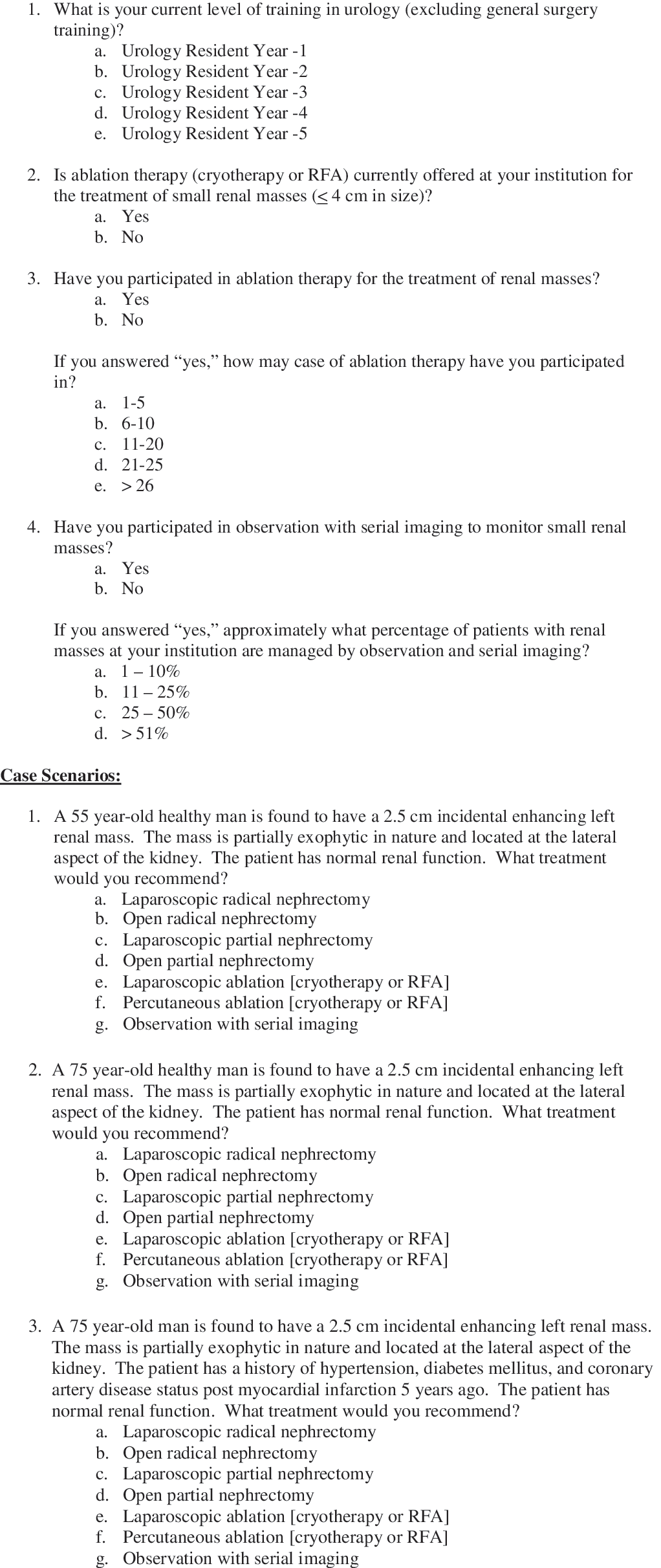
Survey questions distributed to residents-in-training of the American Urological Association.
Descriptive statistics were performed using software from the survey company. The chi-square test evaluated the association between level of training and exposure to ablation or surveillance strategies. Statistical analysis was performed with S-Plus Professional (MathSoft Inc., Seattle, WA).
Results
Surveys were distributed electronically to 1129 urology residents with available e-mail addresses listed in the AUA residents-in-training directory. Ninety were undeliverable leaving a final group of 1039 urology residents, who were contacted by e-mail. Of these, 257 (24.7%) completed the survey. The distribution among the various AUA regions and level of training is highlighted in Table 1.
AUA = American Urological Association.
Of the 257 resident respondents 231 (91%) noted that ablative techniques (either percutaneous or laparoscopic) were offered at their institution of training for the management of SRMs. Despite the vast majority of training institutions offering renal thermal ablation, only 140 (54%) residents reported every participating in one of these procedures. Involvement in ablative procedures increased when comparing junior- and senior-level residents (U1/U2 vs. U3-U5; 38% vs. 63%, p < 0.001), although exposure failed to increase beyond the U3 year (p = 0.38) (Table 2). Finally, when stratifying by number of procedures completed, 80 residents (57%) were involved in 1 to 5 procedures, 35 (25%) in 6 to 10 procedures, 20 (15%) in 11 to 15 procedures, and a 5 (3%) in >15 procedures.
Laparoscopic or percutaneous; cryoablation or RFA.
RFA = radiofrequency ablation.
Residents were polled in a similar fashion concerning their participation in active surveillance regimens for SRMs. Of the 257 respondents, 224 (87%) residents reported having participated in active surveillance. Similar to ablative experience, exposure increased when comparing junior- and senior-level residents with over 90% of senior residents noting participating in surveillance protocols (U1/U2 vs. U3-U5; 77% vs. 93%, p < 0.001).
With regard to the three case scenarios presented, 98% (251) of residents chose a partial nephrectomy (laparoscopic or open) for management of an SRM in a relatively healthy 55-year-old man. Further, no residents chose to treat this same patient with a radical nephrectomy (laparoscopic or open), whereas 3% of respondents elected for thermal ablation or active surveillance regimens (Table 3). For a relatively healthy 75-year-old man, over 60% of residents continued to elect for a partial nephrectomy, whereas the percentage recommending ablation or surveillance increased to 35%. Finally, in a comorbid 75-year-old patient, thermal ablation was the most popular treatment selection as recommended by 48% of residents. Over one-third of respondents advocated surveillance in this patient group, whereas 16% still recommended a partial nephrectomy despite multiple comorbid conditions.
Open or laparoscopic.
Laparoscopic or percutaneous; cryoablation or RFA.
Discussion
The stage migration observed for renal cell carcinoma necessitates urologists to appropriately adapt management strategies for these smaller, potentially more indolent renal lesions. Thus, although nephrectomy by laparoscopic or open techniques yields excellent oncologic outcomes, the sequelae of chronic kidney disease, cardiovascular disease, and resultant increased mortality necessitate consideration. 6,13,14 Contemporary practice has therefore evolved to include more kidney preserving strategies, including partial nephrectomy, thermal ablation, and observation with serial imaging. Although partial nephrectomy has increasingly become the treatment of choice for renal lesions <4 cm, the complication rate and substantive learning curve for these higher complexity procedures are notable. 7,15 As such, both renal ablation and observation with promising intermediate term data have become increasingly utilized for management of SRMs in elderly comorbid patients. 8,16,17
In a 2006 resident survey of laparoscopic and robotic surgery, Duchene and colleagues 12 observed that only 50%–60% of residents reported on thermal ablation being performed at their academic institution. Further, almost 70% noted that laparoscopic nephrectomy was the gold standard for managing renal tumors. A subsequent study in 2008, however, by Bandi et al 18 suggested that ablation use at tertiary care academic centers was more prevalent. Specifically, in this electronic survey of 68 academic urologists, 93% noted that thermal ablation (laparoscopic or percutaneous; cryoablation or RFA) was offered at their institution. These two studies present somewhat disparate data on ablation use in academic centers and perhaps a dichotomy in perceived use between urology residents and mentors.
In this study, we surveyed 257 urology residents with a relatively equal distribution across levels of training regarding exposure to both thermal ablation and surveillance regimens for SRMs. We believe that the lower number of U5 residents (12%) in this study is simply a function of the declining number of programs that currently offer a fifth year of specialized urology training. We observed that while 91% of urology residents reported availability of thermal ablative procedures at their institution, only 54% had ever participated in a procedure. Further, when considering urology chief level residents (U4 or U5), only 65% (68 of 105) had ever participated in an ablative procedure during their residency. Exposure to surveillance regimens, however, was far better particularly for the senior level residents. In particular, 95% of chief level residents (U4 or U5) had participated in surveillance regimens for SRMs.
These data are particularly interesting when considering treatments proposed by residents for SRMs when presented case scenarios. It appears that the concept of kidney preservation has largely been espoused by urology trainees. In particular, when considering a 55-year-old patient with a 2.5 cm renal mass, 98% advocated partial nephrectomy and no respondent recommended a radical nephrectomy. As age and comorbidity profile increased, resident respondents also demonstrated their understanding of the role for less invasive therapies. While only 2% of respondents recommended surveillance for SRM in a healthy 55-year-old patient, this increased to 8% and 37% for the healthy and comorbid 75-year-old patient, respectively. Trends for ablation use similarly rose from 2% for a healthy 55-year-old patient to 27% and 48%, respectively, for a healthy and comorbid 75-year-old patient.
Despite these trends, over 60% of residents still advocated surgical extirpation in a healthy 75-year-old man. Further, 16% of respondents recommended partial nephrectomy in a 75-year-old patient with multiple medical problems. These latter observations are particularly notable when considering competing causes of mortality in this patient population. In particular, Hollingsworth and colleagues 19 noted in a population-based study that the estimated 5-year competing-cause mortality for patients >70 years of age was 28.2%. This was greater than the estimated 5% cancer-specific mortality for renal tumors <4 cm in this same patient population, suggesting that surgery may represent overtreatment for these SRMs. Such considerations appear to need further emphasis among residents-in-training.
Perhaps a greater concern is the disparity in training exposure to ablative procedures and subsequent recommendation for management of SRMs. In particular, despite most institutions offering renal thermal ablation (>90%), only 54% of residents were ever involved in such a procedure. Even for chief level residents (U4/U5), less than two-thirds had ever participated in renal ablation. Paradoxically, however, thermal ablation was the most commonly selected therapy for an SRM in a comorbid, older patient with almost 50% of residents advocating this therapy. Such a discrepancy raises the question if such cases will simply be referred to radiology colleagues for management. Indeed, Bandi and colleagues 18 noted a collaborative approach (urology and radiology) for managing SRMs occurred in only 50% of cases. More recently, Long and Park 20 further observed differences in ablation approach (laparoscopic vs. percutaneous), re-ablation rate, and need for nephrectomy when stratified by medical specialty (urology vs. interventional radiology). In particular, they observed that both RFA and cryoablation recurrence rates were higher when a percutaneous approach was used and appeared to correlate with medical specialty. In a similarly designed literature review, Kunkle and Uzzo 21 noted similar discrepancies when comparing urology and radiology literature on ablation.
Given the suggested disparity in outcomes for thermal ablation between urology and radiology literature, we believe that it is imperative that urologists managing patients with SRMs collaboratively work with radiology colleagues when a patient elects for an ablative therapy. This is particularly true for lesions approach percutaneously under image guidance. Unfortunately, results from our survey suggest that most urology residents (including graduating chief residents) may be ill equipped to adequately function in this role. Similar future trends risk relegating urologists to diagnosticians of SRMs while limiting our unique knowledge and experience as it pertains to kidney tumor biology, relevant anatomy, and inherent procedural complications. Thus, although both ablative and surveillance regimens are seemingly less attractive resident training exercises compared with extirpative procedures, we would argue that participation is necessary to ensure appropriate treatment for SRMs in the future.
We acknowledge several limitations in this study. First, the nature of this survey study may bias toward urology residents with a particular interest in management of SRMs and thermal ablation, thereby impacting likelihood of involvement in certain cases. Second, since this was an Internet-based study, a bias was introduced to those who would regularly check and use their e-mail. Third, in an effort to broadly query exposure to ablation, both RFA and cryoablation were grouped together as was operative approach. Thus, specific differences between ablative techniques or approaches were not available for analysis. Finally, this study fails to address the therapeutic efficacy of thermal ablation in the management of SRMs. Here, we simply query training exposure to this treatment modality. Nonetheless, despite these limitations, we believe that this study accurately captures experience of a significant cross section of current urology residents with respect to management of SRMs.
Conclusions
The increasing diagnosis of incidental SRMs in older comorbid patients has prompted an evolution in therapies offered by practicing urologists. The increased use of surveillance and ablation treatments necessitates urology residents to be familiar with such strategies when completing training. This study suggests that although resident exposure to surveillance is appropriate, participation in ablative procedures is low particularly when considering that many residents would eventually recommend such treatment to manage SRMs. Urology training must continue to evolve and incorporate current techniques into their curriculum.
Footnotes
Disclosure Statement
No competing financial interests exist.