
Abstract
Background and Purpose:
Robot-assisted radical prostatectomy (RARP) has been performed in Rochester, NY, since 2003. Currently, 10 area urologists perform RARP, and robotic training has become an important component of the residency. We present data describing the timeline for adoption, both in clinical practice and in the residency program.
Materials and Methods:
We reviewed the operating logs for all surgeons who were performing prostatectomies in all hospitals in Rochester, NY, from 2003 to 2007. We examined the influence RARP had on other treatments, including brachytherapy and cryotherapy. Surgical logs of graduating chief residents were also reviewed.
Results:
Eleven surgeons in Rochester regularly perform radical prostatectomy (10 perform primarily RARP, one performs only open prostatectomy). Three of the city's four hospitals have robotic systems. In 2003–2004, there were 30 open prostatectomies performed monthly and fewer than 10 performed robotically. By 2006, the trend was reversed, with 50 robot-assisted prostatectomies performed each month and fewer than 10 open prostatectomies (P<0.05). The rate of brachytherapy fluctuated, increasing in centers without a robot. The number of open prostatectomies in centers without a robot dropped significantly to fewer than 10 cases per year. There was also a significant decrease in the number of open prostatectomies performed by chief residents.
Conclusions:
Since the introduction of surgical robotics, significant changes have been seen. The volume of radical prostatectomies performed by surgeons at institutions with robotics has increased; the volume at robot-free institutions has become nominal. There is a trend toward increased radiation therapy at robot-free institutions. While radical prostatectomies logged by graduating chief residents have increased, open prostatectomy experience is now minimal.
Introduction
Compared with the generally slow, deliberate adoption of other technology and methods for performing urologic procedures, the adoption of robotics and robot-assisted prostatectomy has been rapid. After relatively few years of clinical use, numerous manuscripts from academic and community-based centers reported comparable, and in some cases better, short-term outcomes and lower complication rates. 4,6 –15 Robot-assisted surgery was adopted in Rochester, NY, in 2003. There are currently five robotic systems operating in three hospitals that are located within a 5-mile radius of one another.
We present data to elucidate how robot-assisted surgery has influenced the treatment of patients with prostate cancer and urologic education in a midsized American city.
Materials and Methods
Rochester is a medium-sized city located in upstate New York with a city population of approximately 210,000 and a metropolitan area population of just over 1 million. It is bordered by two other medium-sized cities—Syracuse and Buffalo. Each city has its own academic center and maintains its own referrals. Within the city of Rochester, there are four hospitals: One academic center with an affiliate hospital and two community-based hospitals. There are currently five da Vinci Robotic Systems installed in three of the four hospitals. Two are located in the university hospital (Strong Memorial Hospital) and one in its affiliate (Highland Hospital). The remaining two are located in one of the community based hospitals (Rochester General Hospital), which also participates in the training of residents from the university. The last hospital (Park Ridge Hospital) does not have a robot.
All urologic robotic cases performed in Rochester were prospectively enrolled in our central quality assurance database by an independent, nonmedical person. These data were checked monthly against each hospital's operating room log. To obtain the data on open prostatectomy, we retrospectively reviewed the case logs for all surgeons who were performing open prostatectomies in all hospitals in Rochester, NY, between 2003 and 2007. We also assessed other modalities of prostate cancer treatment, including brachytherapy and cryotherapy, to evaluate the influence that robot-assisted prostatectomy has had on other modalities of treatment. The linear regression model was used to study the relation between the number of operations and time and the Durbin-Watson (DW) test was used to test autocorrelation. In addition, the surgical logs of the graduating chief residents with respect to open and robot-assisted case numbers were reviewed.
Results
Prostatectomy trends
During the years 2003 to 2007, there were 11 urologic surgeons in Rochester, NY, who regularly performed radical prostatectomy. Before 2003, most prostatectomies were performed via an open approach with only one surgeon performing laparoscopic prostatectomies. That surgeon switched to the robotic technique in 2003 when the university hospital acquired Rochester's first da Vinci robot. The larger of the two community-based hospitals (Rochester General Hospital) acquired the city's second system in 2004. Subsequently, demand for robot-assisted surgery has increased in Rochester such that there are now five robots in three hospitals, all within a 5-mile radius of one another.
Citywide, between the years 2003 and 2004, there were 30 open radical prostatectomies performed each month and fewer than 10 performed via the robotic approach (Fig. 1A–C). In 2006, the trend was significantly reversed, with 50 robotic cases performed each month and fewer than 10 performed via the open approach (P<0.05), representing a decrease in open cases of more than 66% (Fig. 1A). The break point was March of 2004, and by the end of 2007, the number of open prostatectomies performed monthly had fallen by 90%. The rate of brachytherapy has fluctuated over time and increased in centers that did not have a surgical robot but was still used less often as a definitive treatment modality when compared with radical prostatectomy (Fig. 1C). The yearly totals for radical and laparoscopic prostatectomies performed in centers that did not have a robot dropped significantly, with fewer than 10 cases performed per year. In the hospital that did not acquire a surgical robot, there have been no prostatectomies performed since 2004 (Fig. 2).
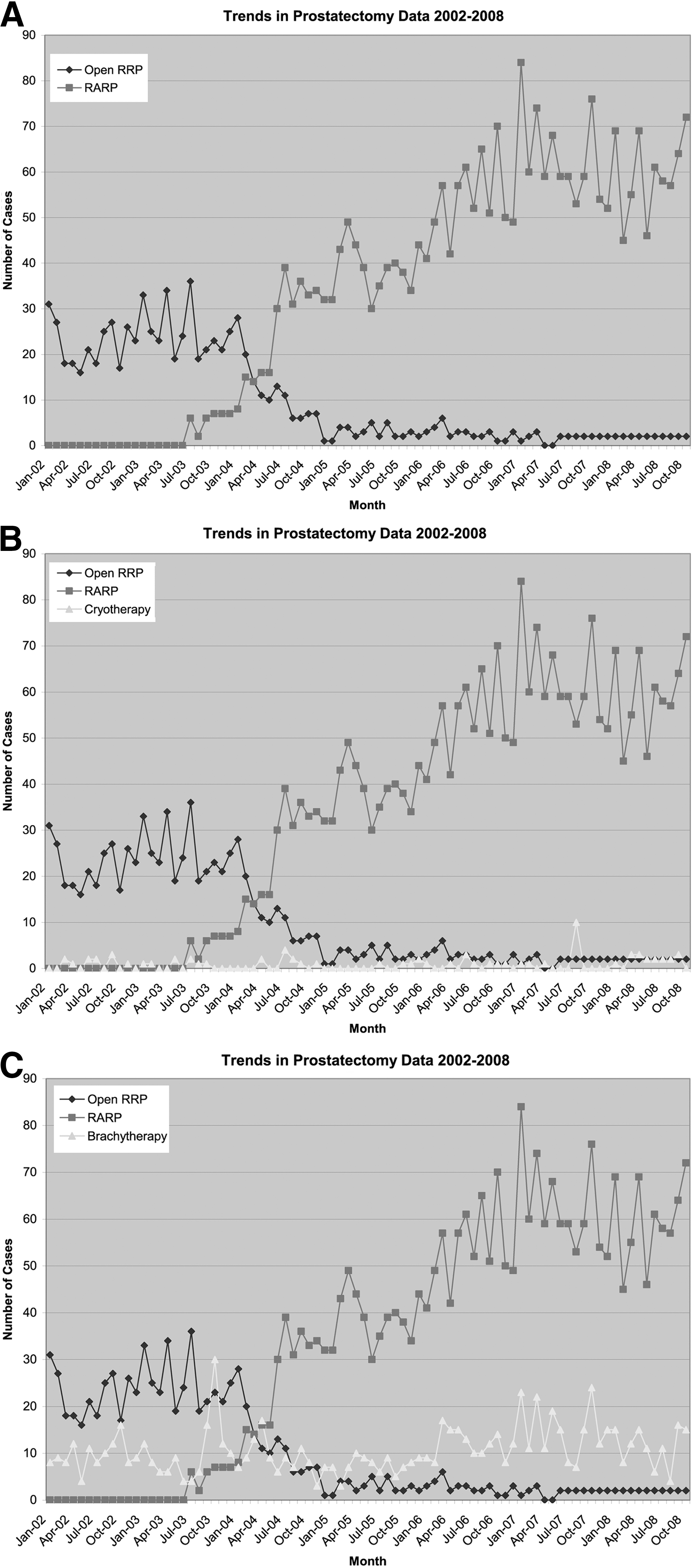
Trends in prostatectomy in Rochester, NY, by all modalities between 2002 and 2008.
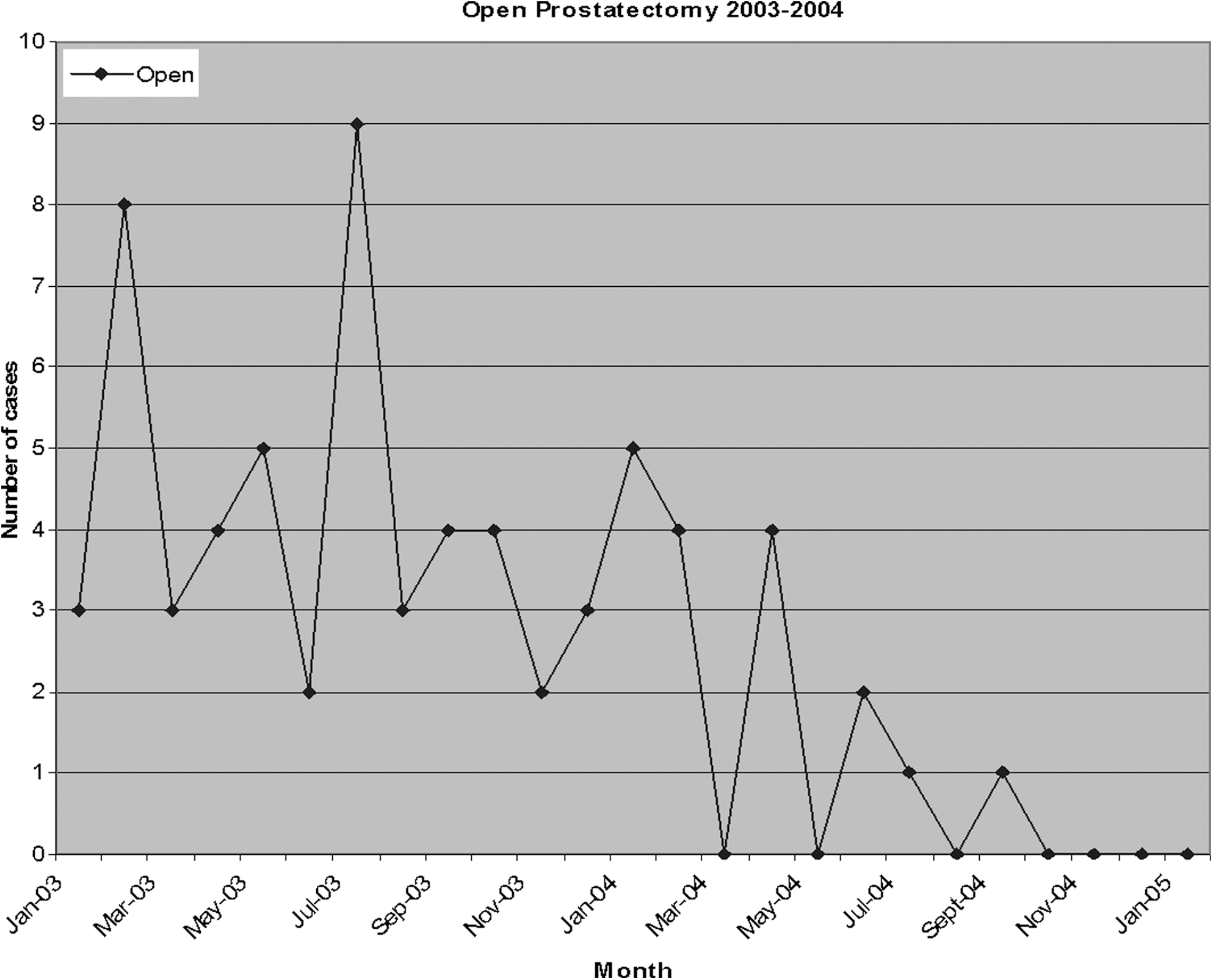
Prostatectomy log from one of the Rochester hospitals without a robotic platform.
The trend over time for different treatment modalities was also analyzed. The linear regression model with time as the covariate was used to study the relation between the number of operations and time. In the regression, we assumed the first order autoregressive error structures in the time series. The DW test was used to test the autocorrelation in the time series (Table 1 and Table 2).
The number of open procedures decreased significantly with time (at a rate of 0.36/month). The number of robot-assisted procedures and brachytherapy treatments both increased significantly with time. The DW test shows significantly positive autocorrelation among the observations.
DW=Durbin-Watson.
The t test was used to compare the time trend of three procedures. The t test shows significant difference among the three procedures.
Educational implications
Resident teaching has also been impacted by the widespread incorporation of robot-assisted surgery. Most concerning is the significant decrease in the number of open prostatectomies that have been performed by graduating chief residents. Overall, however, there has been an increase in the number of prostatectomies that have been performed by the graduating chief residents over time. In 2002, the graduating chief residents averaged 28 prostatectomies, while in 2006, they averaged 98 cases (Fig. 3). In 2002, all cases that were performed by the chief residents were using an open approach, while in 2006, 98% of the cases that were performed by the chief residents were performed robotically (Fig. 3). In 2006, the chief residents logged only four open radical prostatectomies.
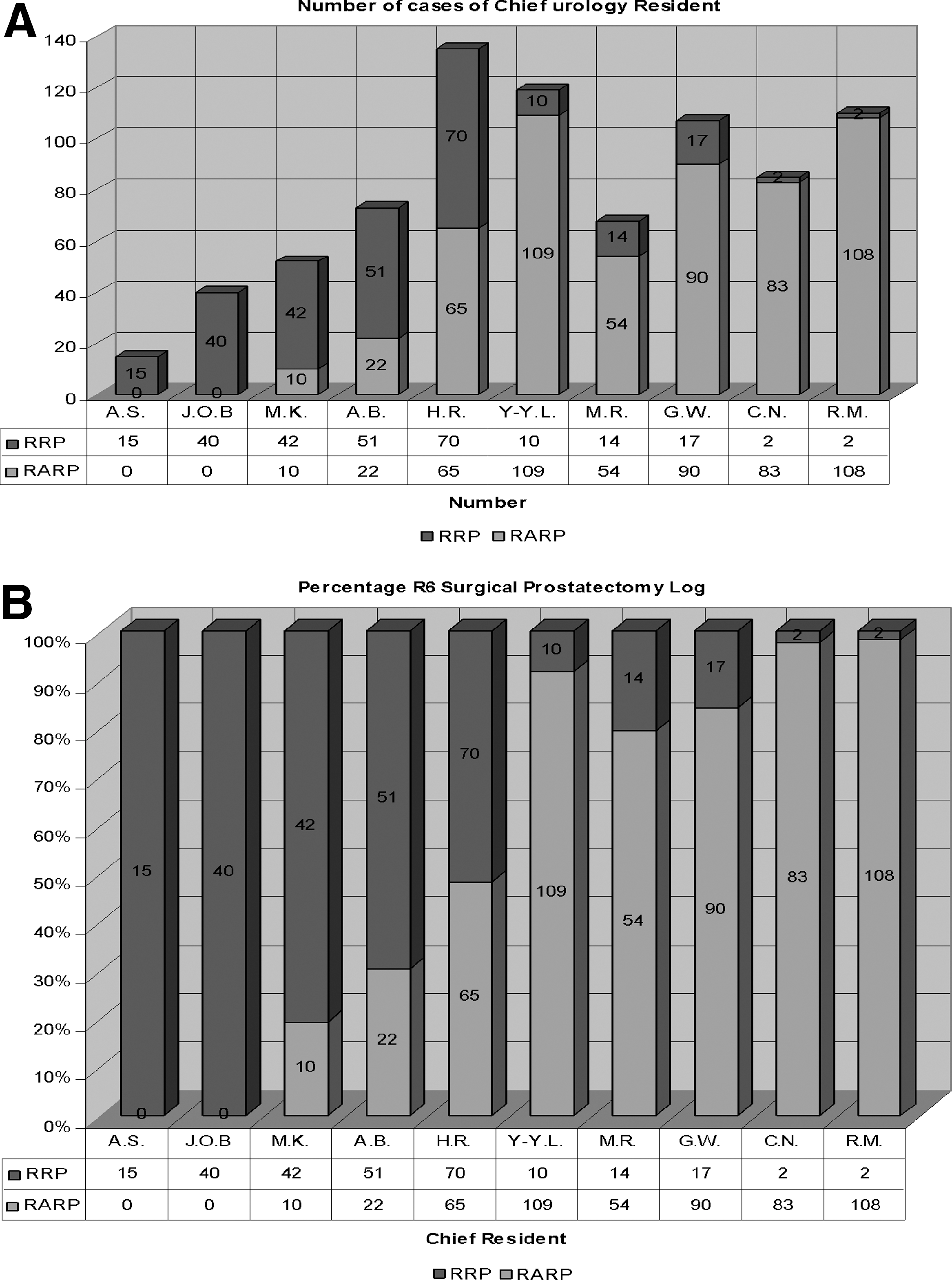
Chief resident log of all prostatectomies between 2002 and 2006.
Discussion
Since the acquisition of Rochester's first robotic surgical system in 2003, individual and group practice patterns, as well as resident training, have changed considerably. While our data confirm this shift toward minimally invasive therapy, we feel this phenomenon is likely multifactorial and because of both physician and patient driven parameters.
From a surgical perspective, the rapid adoption of robot-assisted prostatectomy by the majority of surgeons in our city (only one surgeon still routinely performs open radical prostatectomy) can be explained by two main factors. First, the majority of surgeons in our area made a concerted effort to train to perform robot-assisted radical prostatectomy (RARP) by observing and emulating experts that had superior outcomes and high patient satisfaction. Second, the many benefits of the robotic system (magnified three-dimensional vision, the high precision articulating robotic instrumentation, and the bloodless field secondary to the pneumoperitoneum) fostered a more precise dissection of the prostate with less morbidity. Taken together, these two factors have made a marked difference with regard to oncologic results in Rochester.
Our previously published data have demonstrated that within a surgeon's first 50 robot-assisted cases, positive surgical margins can be greatly reduced. Looking at the data from two of our surgeons, we saw overall positive margin rates drop from 26% to 18% and 44% to 20%. For pT2 tumors, their positive margin rates dropped from 37% to 5.7% and from 27.5% to 7%. 7 While long-term oncologic results are not yet available, these surrogate data are promising.
A recent review of studies that included 200 or more patients who were undergoing either open, laparoscopic, or RARP demonstrated comparable rates of postoperative complications with all three techniques, lower transfusion rates with either laparoscopic radical prostatectomy or RARP, and confirms our finding of improved positive margin rates. 16
Recently, Menon and colleagues 17 reported on the longest term oncologic outcomes yet available in the RARP literature. With a median follow-up of 5 years, they reported a biochemical recurrence ( PSA level ≥0.2 ng/mL) rate of 13.6%, demonstrating that oncologic outcomes are not compromised by this technique.
From a patient perspective, various factors apart from these data may explain a preference for the robot-assisted approach. Notably, there is the intense marketing campaign for newly available and less invasive therapies, which is being fostered by the robot's manufacturer as well as by the hospitals. There has been no greater advertisement campaign in either the university or private health systems in Rochester than for robot-assisted prostatectomy. In some part perhaps because of marketing, many with newly diagnosed prostate cancer see robot-assisted prostatectomy as a means to undergo curative therapy with a faster, less painful recovery.
The cost of purchasing five robotic surgical systems must also be acknowledged. With a $1.75 million purchasing price and the steady-state cost of nonreusable maintenance equipment, it is not surprising that several studies have demonstrated the increased cost associated with robot-assisted prostatectomy. 18 –20 Many hospitals continue to find the da Vinci Robotic System to be cost-prohibitive. Despite this, they also fear the loss of patients to other centers and physicians who have the ability to offer robotic technology. Therefore, an increasing number of centers appeal to philanthropy to purchase their systems.
With just over 1100 da Vinci robots currently installed in United States hospitals and an average yearly increase of approximately 200 machines over the last 3 years, 21 this platform is likely to continue expanding and being applied for other major urologic operations. Although the procedure might lose money directly, the greater loss comes from the loss of the patient to another health care system and the indirect revenue from ancillary tests as well as future care. Many of the available studies examine only direct cost and do not consider the indirect losses, such as the revenue diverted to competing health care systems for primary or ancillary procedures.
The absence of a robotic platform may also affect physician recruitment. Currently, most graduating residents, as can be seen from our data, are performing robot-assisted prostatectomies. Understandably, it could be difficult for a hospital without a robotic platform to attract a graduating chief resident whose number of open prostatectomies could be counted on one hand. Hospitals with the robot often use it as a recruitment tool for high-demand surgical subspecialists in urology, gynecology, and colorectal surgery.
From the viewpoint of the health care insurance industry in Rochester, the conversion from open to RARP will likely continue to be a cost saving proposition. Conversion to robot-assisted surgery has not led to an increase in reimbursement. In fact, the insurance guarantors reimburse the same amount for a robotic-assisted as for a standard laparoscopic radical prostatectomy. With shorter hospital stays, upfront savings are seen, and the insurance companies may look forward to future savings as well. If one uses positive margins as a surrogate marker for a higher likelihood of prostate cancer recurrence, one can imagine that the lower positive margin rate previously described in this community after the transition to RARP may translate into lower rates of adjuvant pelvic radiation therapy, androgen blockade, imaging, and other ancillary cost, thus reaping greater savings in the future. 7
With regard to surgical training, we have had to modify our training techniques significantly so that residents can learn to perform robot-assisted surgery while maintaining patient safety. The exact techniques used to accomplish this have been previously reported. 22 The fact that all of our graduating residents who have access to a robotic system perform radical prostatectomy robotically is a testament to the effectiveness of the teaching program and also, unfortunately, speaks to the dearth of experience with the open approach. Not only are our residents exposed to the robotic platform, they are also logging real console time. By the time our residents reach their chief year, their skills have developed to the point that they perform the majority of all robotic cases from skin to skin. Often this is performed with the attending surgeon as their bedside assistant. The systematic approach to robotic training of our residents has previously been reported, including the demonstrated significant improvement in both operative time and performance scores over time. 22
From an historic perspective, the transition from open to laparoscopic or robotic surgery for many urologic procedures has not always been smooth. This was first seen with laparoscopic radical nephrectomy and partial nephrectomy, then with laparoscopic radical prostatectomy, and now with RARP. The primary concern has always been the ability to perform an oncologically and functionally equivalent operation with the new technique. We now, however, have up to 7-year follow-up data for several mature series showing equivalent, and in some cases improved, oncologic and functional results in addition to lower complication rates. 7,23,24 For better or for worse, we predict that at some point in the future, many surgeons will not be able to perform open radical prostatectomy when robot-assisted surgery is inappropriate or impossible because of adhesions from previous surgery. These patients may need referral to an open surgical specialist to have an open prostatectomy performed.
Conclusion
Since 2003, the availability of robotic surgical systems has clearly changed the way patients with prostate cancer are treated in Rochester, NY. The nearly complete conversion from open to robot-assisted prostatectomy has changed both individual and group practice patterns, the training of residents, and has created new challenges in resident education.
Footnotes
Disclosure Statement
Louis Eichel is the owner of Intuitive Surgical® stock. The other authors have no conflicts of interest to declare.