
Abstract
Background and Purpose:
Cadmium exposure has been associated with a greater risk of kidney stone formation in occupational exposure studies, but data on such an association in the general population are scarce.
Subjects and Methods:
We assessed the National Health and Nutrition Examination Survey data from 1988 to 1994 in terms of the risk of stone formation. Persons reporting a history of kidney stones were defined as stone formers (n=749), and the association between a positive history of kidney stones and high environmental cadmium exposure levels (defined as urinary cadmium >1 μg/g) was analyzed by logistic regression analysis, stratifying by sex and adjusting for age, race/ethnicity, body mass index, smoking habits, region of residence, and daily intake of calcium and sodium.
Results:
The odds ratio of lithiasis associated with urinary cadmium >1 μg/g was 1.40 (95% confidence interval 1.06, 1.86) in females (P=0.019). The association between urinary cadmium and kidney stones was not significant in males.
Conclusions:
These findings suggest that moderately high levels of urinary cadmium are associated with a greater propensity for kidney stone formation in females in the general population.
Introduction
Subjects and Methods
The NHANES is a nationally representative, cross-sectional survey of the noninstitutionalized civilian population 8 that is conducted regularly in the United States (U.S.) by the National Center for Health Statistics. It is based on standardized questionnaires that are administered at home by trained interviewers, followed by a detailed physical examination at a Mobile Examination Center. We limited our analysis to the NHANES III (1988–1994) survey (because it was the only one to include data on the interviewees' history of kidney stones) and to subjects ≥20 years of age. The information relevant to our analysis included age, sex, race/ethnicity, body mass index, urinary cadmium, serum calcium, serum alkaline phosphatase, serum 1,25-dihydroxy-colecalciferol, and self-reported details of dietary intake of calcium and sodium, smoking habits, high blood pressure, and a history of kidney stones. We also analyzed data on the use of diuretics and the frequency of ingestion of the dietary items considered in the NHANES database 8 with a view to identifying any correlations between diet and both urinary cadmium and kidney stones. Our model was further adjusted to take into account the area where the persons surveyed lived (based on the U.S. census regions—ie, Northeast, Midwest, South, West). The NHANES dataset does not include data on blood cadmium or urinary calcium levels, or on stone composition, so these variables could not be used in our analysis.
The laboratory procedures used for the variables analyzed here are described on the NHANES website. Briefly, urinary cadmium was measured by atomic absorption spectrometry using a modified version of the method described by Pruszkowska and associates 9 and a Perkin-Elmer Model 3030 atomic absorption spectrophotometer with Zeeman background correction; serum calcium was measured with a Nova 7 electrolyte analyzer (NOVA Biomedical, Waltham, MA); serum alkaline phosphatase was measured with a 2-amino-2-methyl-1-propanol buffer; serum 1,25-dihydroxy-colecalciferol was measured with a DiaSorin radioimmunoassay kit (DiaSorin Inc, Stillwater, MN).
We defined all persons who reported an episode of kidney stones as stone formers, and those who reported more than one episode as recurrent stone formers. A high environmental cadmium exposure was assumed for persons with urinary cadmium values >1 μg/g creatinine, a cutoff suggested by previous studies on cadmium toxicity in the general population. 7,10,11 Persons who reported having smoked at least 100 cigarettes during their lifetime were classified as active smokers if they were currently smoking or as former smokers if they quit smoking.
To assess the daily intake of calcium and sodium, a dietary interview was used. Participants were asked to report all food and beverages consumed for the previous 24 hours, from which the daily amount of nutrients was obtained using the U.S. Department of Agriculture Nutrient Database. Continuous variables were reported as means (standard deviation), except for urinary cadmium, which was reported as median (interquartile range) because of its skewed distribution. Categorical variables were reported as crude numbers and prevalence percentages. Significant differences for continuous and categorical variables between groups were tested using the Student t test (and Mann-Whitney for urinary cadmium) and the chi-square test, respectively. Correlations between continuous variables were tested in univariate models with the Pearson test and in multivariate models by multiple linear regression.
We assessed the strength of the association between cadmium exposure and kidney stones by means of a logistic regression stratified by sex and adjusted for potential confounders—eg, age, race/ethnicity, body mass index, smoke, region of residence, and diet.
The accepted level for a significant two-tailed difference was P<0.05. All statistical analyses were performed using the survey package in the R statistical language to account for the complex sampling design and weights in NHANES surveys. Figures were obtained with GraphPad Prism rel. 5.0 (GraphPad Software, San Diego, CA).
Results
The overall analysis included 15,690 subjects; 749 (4.8%) were stone formers, and 176 (1.1%) of these were recurrent stone formers. Their characteristics are shown in Table 1. The stone formers were a mean 12 years older, with a significant prevalence of males, higher body mass indices, and higher serum alkaline phosphatase levels, and slightly but still significantly higher serum 1,25-dihydroxy-colecalciferol levels, while their serum calcium levels did not differ to a statistically significant degree from those of the group with no history of kidney stones (P=0.190). Stone formers made greater use of diuretics, and whites were more prevalent than other ethnic groups. Females had higher urinary cadmium levels than males (median urinary cadmium 0.48 vs 0.36 μg/g, P<0.001). A high cadmium exposure was identified in 16.4% in the no-stones group and 21.4% among the stone formers, with median urinary cadmium levels of 0.42 vs 0.67 μg/g (P<0.001). The proportion of subjects with a high cadmium exposure was higher among those living in the Northeastern regions than for those living elsewhere (P<0.001), while stone formers were more common in the Southern region than in the Western regions (P=0.002; Fig. 1). The median urinary cadmium levels in stone formers and no-stone formers are shown in Figure 2, divided by sex. The only significant difference between recurrent and single-episode stone formers was the prevalence of males (68.8% [95% confidence interval (CI) 61.9, 75.6] vs 57.7% [95% CI 53.6, 61.7], P=0.009).

The proportion of subjects with high urinary cadmium (circles) and kidney stones (triangles) by geographic region. CI=95% confidence interval.
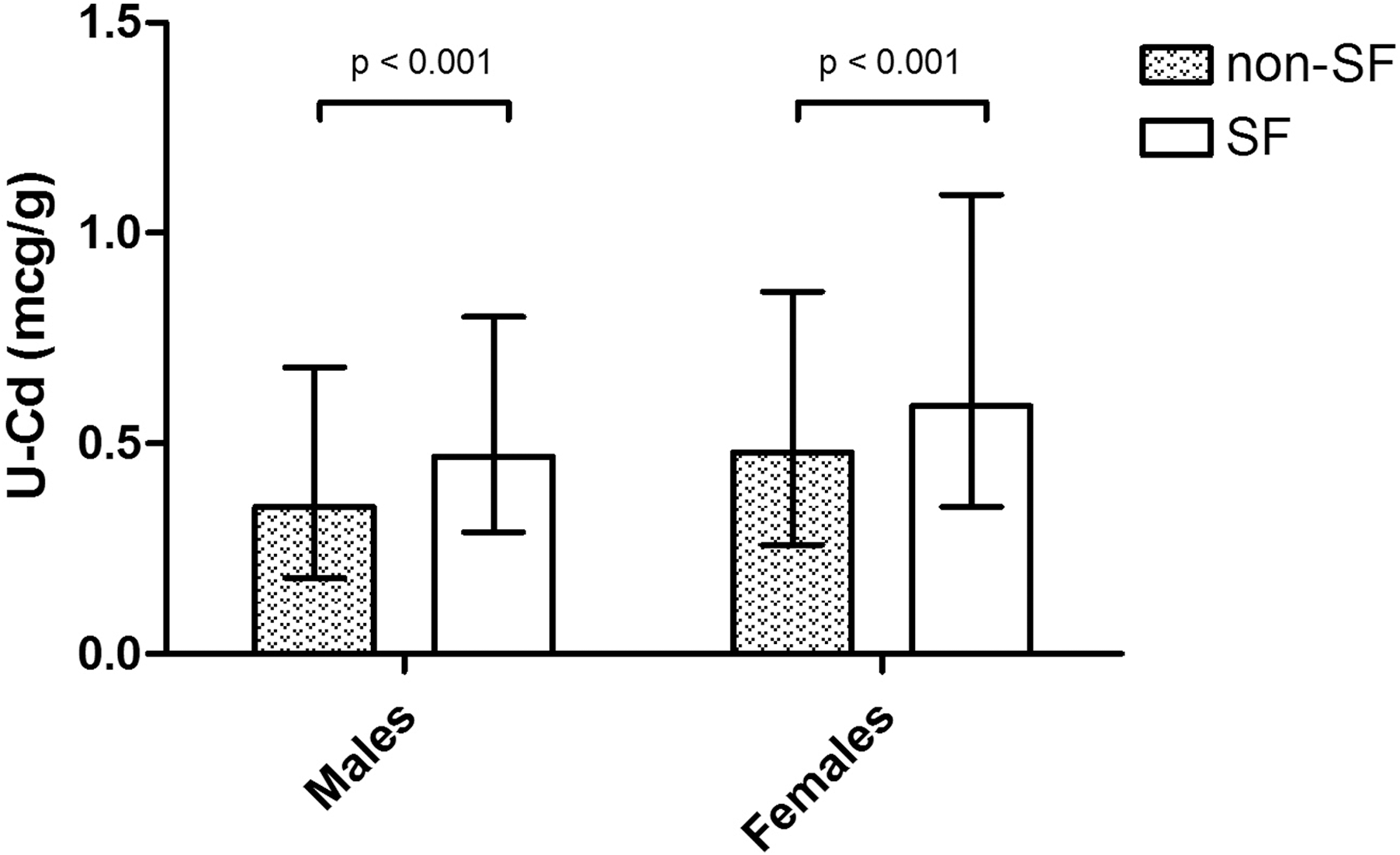
Median values of urinary cadmium in stone formers and nonstone formers divided by sex. Vertical lines represent 25th and 75th percentiles.
Parentheses report point estimate (mean for continuous variables, median for urinary cadmium, percent for categorical variables); brackets report 95% confidence interval for the point estimate (5th and 95th percentiles for urinary cadmium).
We found a slight but significant correlation between log-transformed urinary cadmium and serum alkaline phosphatase levels (r=0.15, P<0.001), but serum alkaline phosphatase was only slightly associated with stone forming by multivariate analysis (odds ratio [OR] 1.002, 95% CI 1.001, 1.004). We found no significant correlation between urinary cadmium and serum 1,25-dihydroxy-colecalciferol levels (r=−0.08, P=0.321).
We sought a correlation between urinary cadmium and the food categories in the nutritional enquiry on the study population, building a stepwise multiple linear regression model that was adjusted for age and sex with log-transformed urinary cadmium as the dependent variable and the self-reported frequency of assumption of the food categories as independent variables. The food categories considered were: Bread and cereals, fruit, vegetables, meat, fish, eggs, milk and dairy products, various beverages. A high consumption of coffee (F=14.9), bread (F=9.4), fruit (F=7.9), corn bread, muffins, tortillas (F=6.5), and beer (F=5.4) was associated with higher levels of urinary cadmium.
After adjusting for age, race/ethnicity, body mass index, smoke, region of residence, and daily intake of calcium and sodium, the logistic regression analysis showed that females in the high cadmium exposure group had an OR of kidney stones of 1.40 (95% CI 1.06, 1.86). Further adjusting for the nutritional items found associated with stone forming did not change the results (Table 2).
OR=odds ratio; CI=confidence interval.
On multivariate analysis, the association between high cadmium exposure and kidney stones was not significant for males.
When the same logistic model was applied to the recurrent stone formers, it showed a similar trend of the results, but it failed to reach statistical significance, probably because of the small number of subjects involved.
Discussion
Although nephrolithiasis is considered to be a multifactorial disorder related primarily to dietary factors, a higher incidence of kidney stones has been reported in subjects occupationally exposed to cadmium. 3 –5 Blood and urinary cadmium are associated with possibly cadmium-related toxic effects in the general population at much lower exposure levels than was previously believed. Concentrations one order of magnitude lower than those considered toxic in industrial medicine have been associated with a number of disorders, 6,7,12 –14 but—to the best of our knowledge—the association between cadmium exposure and kidney stones has yet to be reported in the general population. We used the large NHANES dataset to investigate this issue and demonstrated that females with urinary cadmium levels >1 μg/g have a 40% higher risk of forming kidney stones than females with urinary cadmium levels ≤1 μg/g, after adjusting for age, race/ethnicity, body mass index, smoking habits, region of residence, intake of calcium and sodium, and food items. We did not adjust our model for other factors known to be associated with kidney stones—ie, high blood pressure and diabetes mellitus, because it has been demonstrated that both these conditions can be caused by cadmium exposure and may therefore be a part of the causal pathway of cadmium-induced kidney stone formation. 14,15
It is hard to explain the greater use of diuretics among stone formers, partly because it is not clear which diuretics are involved. Renal calcium stone patients may have been prescribed thiazides to prevent further kidney stones, but by far the majority of our participants had experienced only one stone-forming episode and were unlikely to have been recommended such a treatment. Furosemide increases calciuria and could theoretically raise the risk of renal stones, but it also increases diuresis and, as far as we know, no one has reported on any renal lithogenic risk being associated with this drug. Diuretics may have been prescribed to treat hypertension, which is very frequently associated with renal stone disease. 16 The prevalence of hypertension reported by stone formers was higher than in controls in our study, too (Table 1).
As for smoking habits, a higher prevalence of smokers among patients with urolithiasis has never been reported before. Although smoking has been shown to damage the kidney through various mechanisms, 17,18 it is difficult to guess the putative pathogenic mechanisms leading to lithogenesis. One possibility relates to the cadmium contained in tobacco. Cigarette smoke contains thousands of different chemical substances, including toxic metals such as cadmium, and smoking a packet of cigarettes a day results in the inhalation of a mean 3.6 to 6.0 μg of cadmium. 19 It has been demonstrated that, while the cigarette is burning, 30% of the cadmium contained in the cigarette is released in the smoke. In the case of cadmium, there is a high positive correlation between the amount of the metal contained in cigarettes and tobacco and its release in the smoke. In addition, persons who smoke cigarettes containing the highest cadmium levels have higher blood cadmium concentrations than smokers of cigarettes with a lower cadmium content. 20 In areas without cadmium pollution, cigarette smoking may thus be a serious source of chronic cadmium exposure. 19 Our analysis, however, shows a significant correlation between cadmium exposure and kidney stones in women even after adjustment for smoke.
Another possible source of cadmium is food. Amzal and associates 21 reported the results of a 20-year dietary follow-up in a group of 680 nonsmoking women whose daily dietary cadmium intake ranged between 7 and 27 μg, and their urinary cadmium levels were in the range of 0.09 to 1.23 μg/g. They found that the main dietary sources of cadmium were bread (36%), cereals and vegetables (20%), and potatoes (17%). Our results are consistent with these findings, in that vegetables, cereals, and potatoes were found significantly associated with urinary cadmium levels in our study population. The strong association that we found between urinary cadmium and coffee consumption (F=14.9, P<0.001) is also consistent with previous reports of a high rate of adsorption of this divalent ion by coffee plants, 22,23 reflecting the level of soil pollution and possibly contributing to chronic cadmium toxicity in the general population. As for the association with beer, wine, and spirits, these beverages reportedly account for a large fraction of cadmium intake—up to 15.38 μg/L in wine and 11.52 μg/L in other alcoholic beverages. 24
Women of childbearing age tend to be more exposed to cadmium toxicity, because cadmium is absorbed by the same carrier as iron in the small intestine, the divalent metal transporter-1. 25 This could explain why females have higher cadmium levels (Fig. 2), and why the association between cadmium exposure and renal stones only emerges for women.
Notwithstanding the fact that the composition of the kidney stones considered in this study was not known, the correlation between cadmium and nephrolithiasis can be seen as a particular feature of the toxic effects of this metal on bone and calcium metabolism, given that the kidney stones in cadmium-exposed subjects are calcium stones. 26 Several mechanisms have been postulated to explain bone anomalies related to cadmium exposure 27 —ie, direct toxic effects on tubular cells leading to hypercalciuria; a reduced intestinal calcium absorption; a reduced activity of the kidney enzymes that hydroxylate 25-hydroxy-colecalciferol to 1,25-dihydroxy-colecalciferol; the interference of parathyroid hormone stimulating vitamin D activation in kidney cells; direct effects on bone (eg, the stimulation of osteoclast activity and collagen breakdown in bone cells).
In vitro experiments have shown that adding cadmium to a culture of osteogenic cells induced a decrease in mineralization, collagen content, and alkaline phosphatase activity. 28 A population study conducted in Belgium on subjects with environmental cadmium exposure (mean urinary cadmium 1 μg/g) found that urinary cadmium correlated with both urinary calcium (which rose by 0.25 mmol daily for every twofold increment in urinary cadmium excretion) and declining bone density (a decrease of 0.01 g/cm2 for each twofold increment in urinary cadmium excretion). 29 In a group of 85 Swedish postmenopausal women, moreover, those with high urinary cadmium levels (median urinary cadmium 1.00 μg/L) had significantly lower bone mineral density and parathyroid hormone levels, and significantly higher levels of urinary deoxypyridinoline (a marker of bone resorption) than those with low urinary cadmium levels (median urinary cadmium 0.25 μg/L): The serum 1,25-dihydroxy-colecalciferol levels did not differ significantly between the two groups, although there was a trend toward higher levels in the group with high cadmium levels (median serum 1,25-dihydroxy-colecalciferol 125 pmol/L in the high-cadmium group vs 111 pmol/L in the low-cadmium group, P=0.08). 30 Our finding of significantly higher levels of serum 1,25-dihydroxy-colecalciferol and serum alkaline phosphatase in stone formers confirms these findings in a much larger group.
The above evidence of cadmium possibly interfering with calcium metabolism in bone and causing increased calciuria might also explain the relationship between renal stones and cadmium exposure in females, who are already at higher risk of osteoporosis (on which cadmium may have an unfavorable impact).
Although our study analyzed a large dataset containing data collected by means of strict, validated protocols, it has some limitations. The history of kidney stones is only self-reported, for instance (although, as other authors have also mentioned, 31 this condition is so readily identifiable that it is unlikely to be misreported by patients), and we had no details of urinary calcium (which would have been useful to better speculate on the mechanism by which cadmium could induce stone formation). Nor did we have any information on the stone's composition, so different pathogenic processes could have been involved. On the other hand, because most stones are composed of calcium (in any of its multiple crystallized forms), the proposed mechanisms linking cadmium toxicity to a greater prevalence of kidney stones from the metal interfering with calcium metabolism at kidney and bone level are reasonable. We also had no data on tubular proteinuria, which might have been able to reinforce the hypothesis that cadmium-induced tubulopathy/nephrotoxicity is behind an impaired tubular calcium reabsorption and its precipitation in urine. We have observed in the NHANES population, however, that the same low level exposure to cadmium as in the present stone-prone patients could be nephrotoxic, because it is associated with reduced glomerular filtration rate and albuminuria. 7
Finally, as in any cross-sectional studies, we cannot rule out the possibility of stone formers having adopted dietary changes to prevent recurrent stones (ie, a higher intake of water, which may be polluted with cadmium) resulting in higher urinary cadmium levels.
Conclusion
The cross-sectional analysis of the large NHANES dataset on the general population suggests that even low cadmium exposure levels may be associated with renal stones in women. The mechanisms behind such an association remain to be seen and warrant further investigation. Our data, together with those drawn from similar studies on cadmium exposure in the general population, 6,11 suggest the need to reconsider the currently accepted safety level for this pollutant.
Footnotes
Acknowledgments
NHANES is a program run by the Centers for Disease Control and Prevention (CDC) and the National Center for Health Statistics. We recognize the inestimable value for science and medical progress of the free access to the NHANES data granted by the CDC. A part of our findings were presented to the 50th Italian Congress of Nephrology 2009, Bologna, Italy, and at the 6th Meeting of the Eurolithiasis Society 2009, Como, Italy.
Disclosure Statement
No competing financial interests exist.