
Abstract
Purpose:
To compare current minimally invasive strategies in renal stone treatment—shockwave lithotripsy (SWL), retrograde intrarenal surgery (RIRS), and minimally invasive percutaneous nephrolitholapaxy—with regard to interventional stress, measured by changes in interleukin (IL)-6 and C-reactive protein (CRP) serum levels during treatment.
Patients and Methods:
143 patients underwent stone therapy for renal pelvic stone (SWL, n=40, mean age±standard error of the mean [SEM]: 48.3±3.1 years; RIRS, n=74, 54.5±1.8; and minimally invasive percutaneous nephrolitholapaxy (MIP), n=29, 54.6±2.7) between 2006 and 2007. Blood samples were prospectively collected 24 hours before and 24 hours after the procedure. Interventional stress was analyzed by changes of the acute phase proteins IL-6 and CRP.
Results:
Mean IL-6 (ng/L) difference (±SEM; 95% confidence interval [CI]) before and after therapy was +8.7 (±10.5; −13.9–31.2), +7.3 (±3.2; 1.5–13.1), and +20.5 (±8.1; 4.0–36.0) in the SWL, RIRS, and MIP groups, respectively (P=0.20). Differences in mean CRP (mg/dL) levels (±SEM; 95% CI) ranged between +0.9 (±1.6; −2.3–4.1) in SWL, +1.6 (±0.5; 0.6–2.5) in RIRS, and +1.8 (±,0.3, 1.2–2.5) in MIP patients (P=0.79). Mean stone sizes (mean/median mm2±SEM) differed significantly between SWL (27/20±3), RIRS (70/16±36), and MIP groups (346/160±104, P<0.0005).
Conclusion:
Contrary to common opinion that SWL is the least invasive therapy, the reported stress parameters did not show significant differences between SWL, RIRS, and MIP, although significantly bigger stones were treated with MIP.
Introduction
Based on mini-PCNL, the MIP was developed to further minimize renal injury. 6,8,9 MIP combined minimal kidney and body wall trauma with effective stone management. Nevertheless, many clinicians recommend the SWL procedure for reasons of reduced invasiveness.
While it may be logical to consider that SWL is able to reduce interventional stress, no study has compared the extent of tissue trauma and the subsequent systemic response of SWL, RIRS, and MIP techniques by quantifiable variables. The acute phase parameters interleukin-6 (IL-6) and C-reactive protein (CRP) have been used in several clinical studies as criteria to evaluate peritherapeutic stress. Furthermore, the increased generation of IL-6 and CRP because of local activation of monocytes and macrophages is assumed to be proportional to the extent of tissue trauma during surgery. 10 –19 In the present prospective study, IL-6 and CRP serum levels have been used to evaluate tissue trauma by the three main therapeutic options in patients with renal pelvic stones.
Patients and Methods
Between May 2006 and March 2007, a total of 143 (40 SWL, 74 RIRS, and 29 MIP, respectively) consecutive patients were included in the study at two centers: University of Tuebingen, Tuebingen, Germany (n=95) and SMZ-Sued, Vienna, Austria (n=48). Patient selection between the different techniques was based on a joint decision by surgeons and patients without further randomization. Patients were appropriately informed about the stone removal procedures and possible complications. Treatment recommendations were based on recommended treatment schemes and guidelines. 20,21 Patients gave written consent to treatment and to the use of their clinical data. Patients with pregnancy, malignant disease, florid infection, and under anti-inflammatory or immunosuppressive treatment were excluded.
The extent of the systemic response to induced tissue trauma after stone treatment was measured by assessing the change in the levels of IL-6 and CRP. Blood samples of 7.5 mL were taken 24 hours before and 24 hours after the procedure. There was no difference in blood sampling. Untimely sampling and delayed blood tests were excluded from analysis. The serum was separated by centrifugation, and aliquots were stored at minus 70°C. We used chemiluminescence technique for IL-6 (range <5.9 ng/L, Immulite One, DPC Biermann, Germany) and turbidimetry for CRP quantification (range <0.5 mg/dL, CRP Turbidimetrie BM, Germany). All tests were performed as recommended by the manufacturers. Stone sizes and differences of post- and pretherapeutic values were calculated and compared according to the applied therapy form using one-way analysis of variance with Tukey-Kramer post hoc analyses with a two-sided P<0.05 considered to indicate significance. JMP 5.2 (SAS Inc, Cary, NC) was used for calculations.
Results
There were no significant differences between the treatment groups in the preoperative variables of age (P=0.10) or sex (P=0.23). Table 1 summarizes the clinical data of the patients analyzed. No significant differences were noted between the treatment groups in baseline levels of IL-6 (P=0.60); however, the SWL group showed significantly higher CRP levels compared with the RIRS (P<0.00001) and the MIP (P<0.00001) groups. Table 1 shows the absolute IL-6 (ng/L) and CRP (mg/dL) values. Changes in IL-6 levels (mean±standard error of the mean [SEM]; 95% confidence interval [CI]) before and after treatment were insignificant in the SWL (+8.7±10.5; −13.9–31.2), RIRS (+7.3±3.2; 1.5–13.1), and MIP (+20.5±8.1; 4.0–36.0) subgroups (P=0.20, Fig. 1). No relevant differences in CRP levels (mean±SEM; 95% CI) occurred after SWL (+0.9±1.6; −2.3 to 4.1), RIRS (+1.6±0.5; 0.6–2.5), and MIP (+1.8±0.3, 1.2–2.5) treatment (P=0.79, Fig. 2). Size of renal calculi (mean/median mm2±SEM) varied between patients who received SWL (27/20±3), RIRS (70/16±36, one patient with 2284), or MIP (346/160±104, one patient with 2893). Stone diameter was significantly increased in patients with MIP compared with SWL (P<0.0003) and RIRS (P<0.0005, Fig. 3).
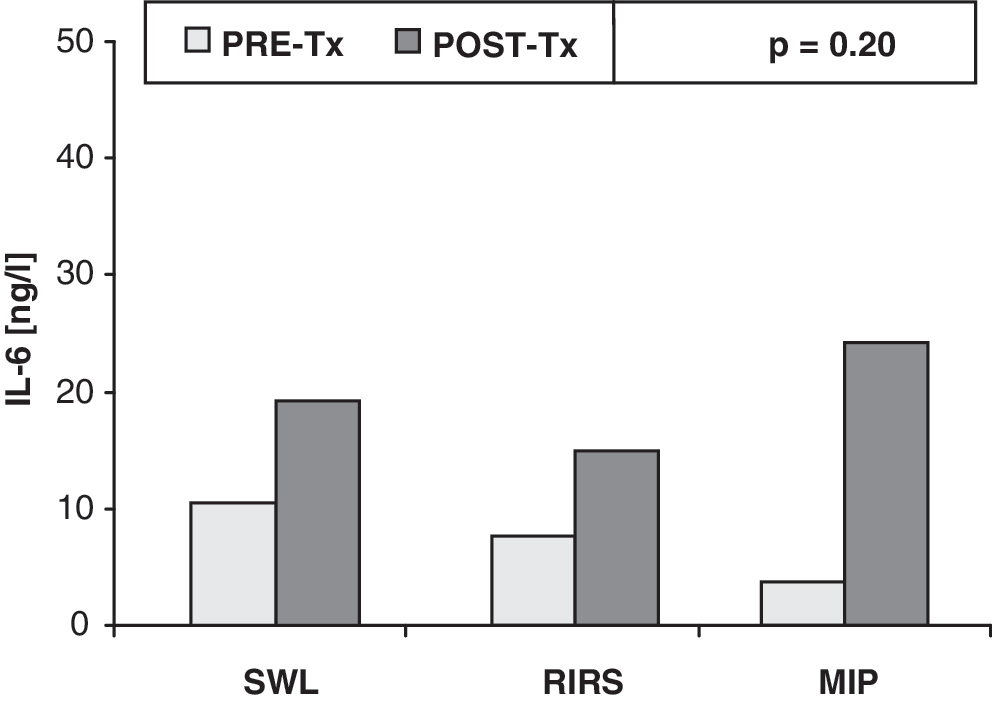
Changes in interleukin-6 (IL-6) levels (mean) between before (PRE) and after (POST) treatment (Tx, P=0.20). Blood samples were taken before and 24 hours after stone treatment. SWL=shockwave lithotripsy, RIRS=retrograde intrarenal surgery; MIP=minimally invasive percutaneous nephrolitholapaxy.

Changes in C-reactive protein (CRP) levels (mean) before (PRE) and after (POST) treatment (Tx, P=0.79). Blood samples were taken before and 24 hours after stone treatment. SWL=shockwave lithotripsy, RIRS=retrograde intrarenal surgery; MIP=minimally invasive percutaneous nephrolitholapaxy.
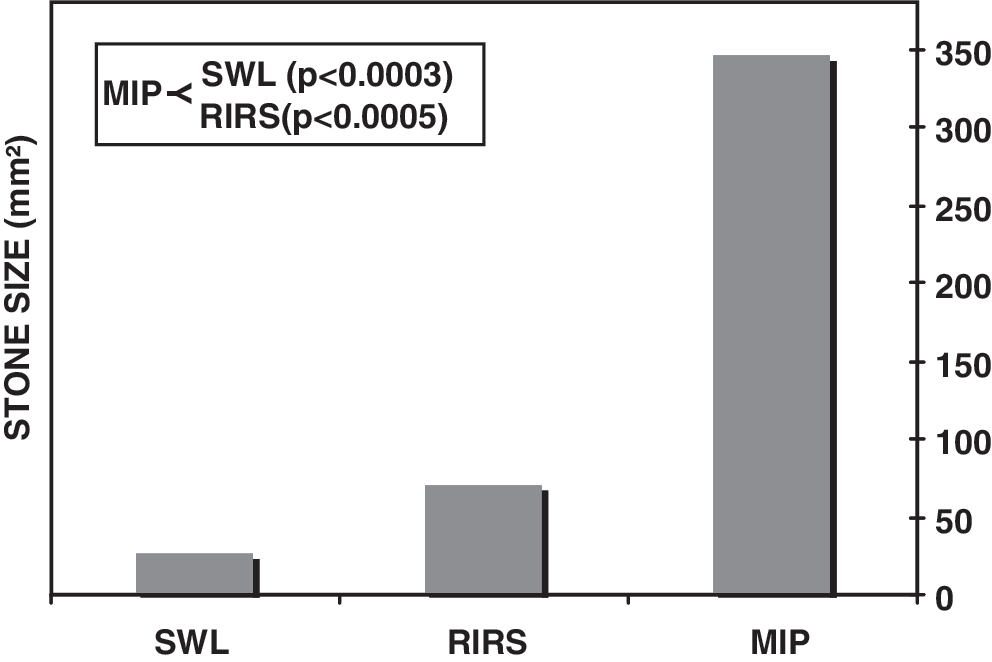
Mean stone sizes in mm2 between the different shockwave lithotripsy (SWL), retrograde intrarenal surgery (RIRS), and (MIP) treatment groups.
SWL=shockwave lithotripsy; RIRS=retrograde intrarenal surgery; MIP=minimally invasive percutaneous nephrolitholapaxy; IL-6=interleukin-6; CRP=C-reactive protein.
Discussion
Stone treatment has dramatically changed in the last two decades and revolutionized the management of upper urinary tract calculus. The advancements in minimally invasive RIRS techniques and auxiliary instruments have allowed access to the complete urinary tract, including lower-pole renal calculi. In addition, miniaturized nephroscope systems with single-step access tract dilation combined with ballistic lithotripsy and low-pressure irrigation using a special vacuum cleaner effect improved the stone-free rates, reduced transfusion rates, hospital costs, and convalescence periods. 6,8,9
Because of its less invasive nature, SWL has traditionally constituted the preferred therapy for patients with small to moderate sized renal calculi. Although RIRS is assumed to be a more invasive treatment option than SWL, this procedure has shown low morbidity and high stone-free rates in the treatment of patients with nephrolithiasis. 1,2 Today percutaneous techniques are taking up an elementary role in patients with a larger stone burden, because of lowered stone-free rates with SWL and RIRS. PCNL complication rates, however, of up to 83% and transfusion rates of up to 17.5% are discouraging in spite of a primary stone-free rate of more than 90%. 22
SWL has long been accepted as the least invasive method in stone treatment, and the safety and efficacy of SWL has been confirmed. 23 Despite its noninvasive nature, SWL is not complication free, 24 and the systemic response to trauma on the basis of objective biochemical parameters has never been compared between SWL, RIRS, and MIP.
Reports in the literature suggest that the intensity of tissue damage can be measured by cytokines and acute-phase proteins. 10 –19 After tissue damage, local neutrophil granulocytes and macrophages activate the cytokine cascade and lead to subsequent production of IL-6 with following local or systemic acute phase reaction. IL-6 can be detected 30 to 60 minutes after injury, and peak serum levels are reached within 6 hours. The IL-6 half-life is approximately 15 hours. 25
In the liver, IL-6 induces CRP production by activating CRP gene expression, leading to the production of CRP. CRP, a member of acute-phase reactants, helps to minimize the extent of local tissue damage and participate in tissue repair and regeneration. 13 CRP synthesis starts after trauma, serum concentrations rising above 5 mg/L by 6 hours with a plasma half-life of about 19 hours. 26 CRP peak levels are reached after approximately 48 hours.
Previous studies showed that IL-6 levels correlated with the operative time, extension of tissue trauma, and the development of postoperative complications. 10,11,14 IL-6 and CRP elevations depend on the type of invasive intervention, and several studies addressed changes in stress parameters in major and minor urologic surgery. A large prospective nonrandomized study compared different trauma derived from laparoscopic and open radical prostatectomy in 403 patients by assessing the levels of serum amyloid A, IL-10, CRP, and IL-6. Although postoperative CRP levels increased more than 100 mg/L and IL-6 values more than 40 ng/L after 12 to 48 hours, no difference in the level of investigated metabolites between laparoscopic and open groups was detected. 18
Fracalanza and associates 27 assessed the invasiveness of robot-assisted laparoscopic and retropubic prostatectomy by CRP and IL-6 analysis. In this trial, 35 patients were recruited for robotic and 26 for open surgery with a median IL-6 baseline of 2 ng/mL and 2.1 mg/L for CRP. Acute-phase response was measured 24 hours after surgery and showed increased IL-6 (24 ng/mL) and CRP (44.2 mg/L) levels, without significant differences between treatment groups.
In contrast, Fonara and colleagues 15 reported a clear advantage of laparoscopic nephrectomy and nephroureterectomy over open surgery in an animal and patient study by measuring CRP, IL-6, and IL-10 levels. This study found significantly higher median serum levels of CRP and IL-6 during and after open nephrectomy. Interestingly, 25 patients who underwent SWL for renal stones were also included in the analysis. The median CRP serum level was 0.5 mg/dL before SWL treatment and did not exceed 2.5 mg/L after treatment. Throughout different observation periods, no significant increase of CRP and IL-6 serum levels was found after SWL. 15
Another clinical trial evaluated 30 patients 24 hours before and after PCNL and open surgery using stress response parameters including CRP and IL-6. In accordance with significantly higher white blood cell counts and an increased risk of postoperative fever, authors reported significantly increased CRP levels in the PCNL group. 28 In a recent comparison with mini-PCNL and conventional PCNL, Li and coworkers 29 reported lower IL-6 (31.3 vs 34.7) and higher CRP (34.5 vs 33.9) levels after 24 hours with minimally invasive PCNL. The authors failed, however, to demonstrate a significant difference in the metabolite levels between both groups. 29
Taken together, these results suggest that there is a threshold for the triggering of acute-phase reactions and the detection of significant IL-6 and CRP differences. Interestingly, significant CRP and IL-6 elevations have been observed in patients with urinary tract infections. 30 –32 In light of these data, our results demonstrated higher baseline CRP levels in the SWL group. Although we ruled out preoperative acute urinary tract infections, a chronic inflammation of the upper urinary tract is often difficult to diagnose and can lead to higher CRP counts.
We noted minor, although not significant changes in IL-6 and CRP levels before and 24 hours after stone therapy in the comparison among SWL, RIRS, and MIP. Contrary to common opinion that RIRS and MIP are considered more invasive compared with SWL, none of them were able to exceed the aforementioned threshold. This might have been even more considerable taking into account that our data showed significantly increased stone sizes in patients who were treated with MIP compared with SWL (P<0.0003) and RIRS (P<0.0005). Despite the lack of a nonrandomized study design, these data may influence the discussion about invasiveness and impartial therapeutic burden in renal stone treatment. These results, however, need to be confirmed by further comparative studies in a larger series.
Conclusion
Therapy-associated invasiveness evaluated by changes in IL-6 and CRP levels showed no significant difference between SWL, RIRS, and MIP. The present study indicates the necessity for a reevaluation of invasiveness and impartial therapeutic burden in renal stone treatment with larger clinical studies.
Footnotes
Acknowledgment
We thank P. Stiefel for reviewing the manuscript.
Disclosure Statement
No competing financial interests exist.