
Abstract
Background and Purpose:
Urethral dilation in the setting of difficult urethral catheterization is sometimes necessary to avoid suprapubic catheterization. Anecdotally, we have observed that less dilation is needed when advancing a silicone catheter over a
Materials and Methods:
A BOSE Electroforce load testing device was used to test 12F and 16F silicone and latex catheters under tensile and compressive forces. This information was used to characterize the buckling (kinking) behavior of the catheters.
Results:
Silicone catheters showed more than 50% greater resistance to kinking when compared with regular latex or coude latex catheters.
Conclusions:
In the setting of the difficult urethral catheterization, silicone catheters should be used after urethral dilation, advanced through a Glidewire, because they offer more resistance to buckling and might necessitate less dilation than conventional latex catheters.
Introduction
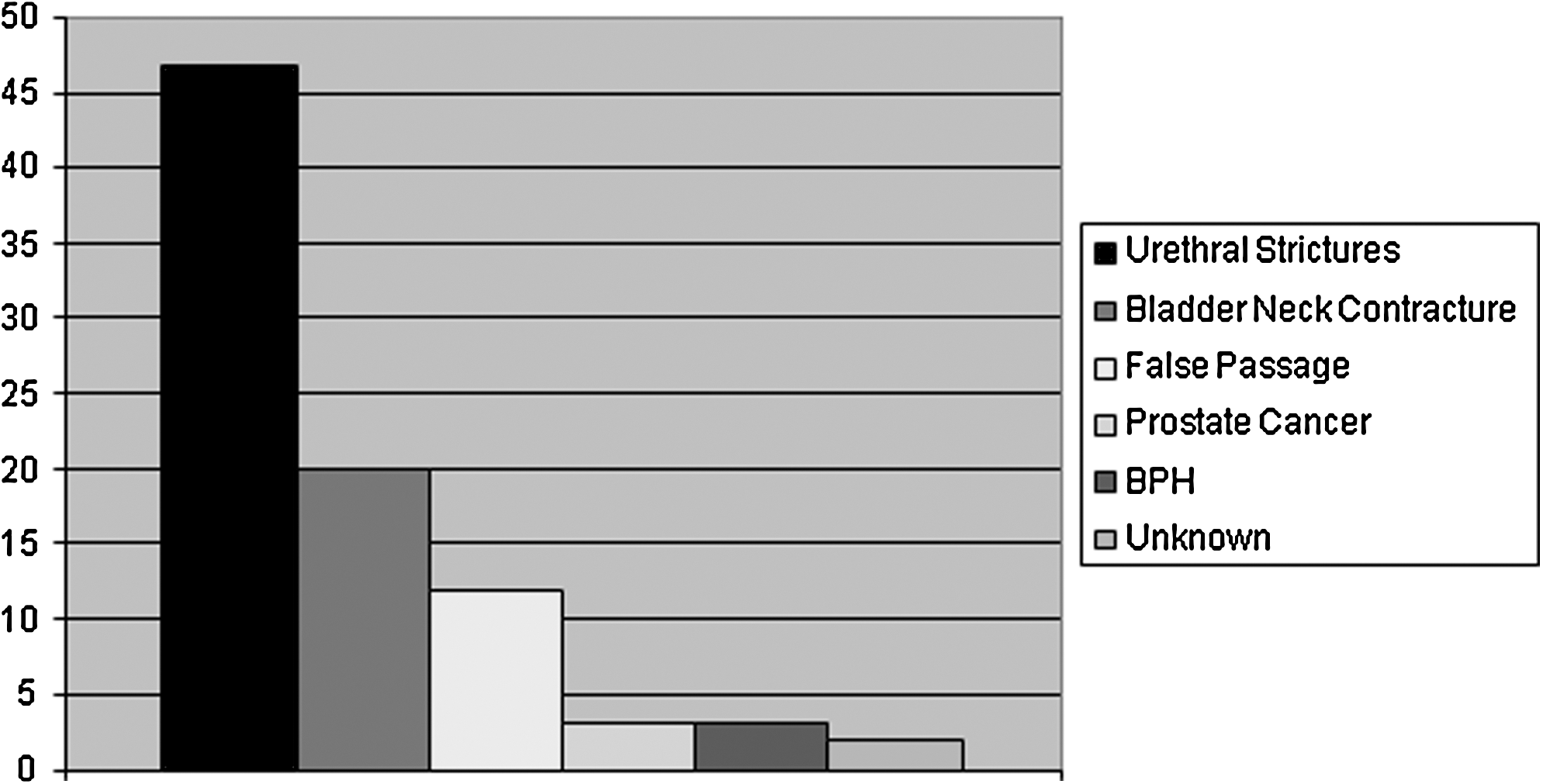
Most common causes of difficult urethral catheterization. Pooled data from Beaghler,1 Freid,2 and Mistry3 series. Included are the 54 patients from the Beaghler series, all of whom underwent flexible cystoscopy, and the 13 patients in the Mistry series who underwent flexible cystoscopy. Twenty patients from the Freid series were included, too, but it was not mentioned in the article how the cause of difficult urethral catheterization was found in these patients.
The fact that strictures and bladder neck contractures are common in cases of DUC suggests that many of these patients end up needing urethral dilation to achieve a successful catheterization.
Urethral dilation in an awake patient is a very painful procedure. Urethral dilation using Heyman dilators or filiforms and followers can result in serious trauma. Dilation performed in the setting of infection or anticoagulation can result in sepsis or severe bleeding.
More and more evidence has recently been accumulating regarding the low success rates of endoscopic approaches to urethral stricture disease (direct vision internal urethrotomy and dilation). 4 Some have now claimed that urethral stricture is an open surgical disease. The purpose of dilating a urethral stricture in the setting of DUC is to be able to drain the bladder as a temporizing measure before definitive surgical repair of the stricture.
For these reasons, it is of utmost importance to dilate up to where a reasonable size catheter can be placed in the patient to avoid unnecessary pain, trauma, bleeding, and the possibility of infection. Most patients without hematuria will do fine with a 12F Foley catheter, whereas in cases of gross hematuria with clots, larger catheters are needed.
In theory, dilation to a certain size (ie, 16F) should allow the placement of a same size catheter. In practice, that is not the case, and usually one has to dilate at least 2F sizes above the catheter needed to pass a urethral catheter over a Glidewire® after dilation. The explanation is that urethral dilators offer more resistance to kinking compared with a urethral catheter that tends to kink more easily.
In our experience with 65 DUC, three patients underwent urethral dilation to achieve urethral catheterization. These patients were dilated with a 12F ureteral access sheath after which a 12F silicone catheter was advanced over a Glidewire successfully. Anecdotally, we have tried doing the same with latex catheters unsuccessfully. Our clinical experience has shown that latex catheters kink more easily than silicone catheters and thus need dilation to a larger F size when compared with silicone catheters. This could mean that when using latex catheters, patients are subjected to unnecessary pain and complications in the setting of urethral dilation during DUC.
In this study, our aim was to quantify the difference in the susceptibility to kinking of silicone catheters compared with latex catheters to translate our clinical experience into something more objective.
Materials and Methods
For the experiment, 12F and 16F catheters of three different types (regular latex, latex coude, and silicone) were used. The initial objective was to test these catheters under tensile and compressive loading. A BOSE ElectroForce® load testing device was used to perform these tests (Figs. 2 and 3). From these load tests, it would be possible to find the Young modulus of the materials, which would be used later to characterize the buckling (kinking) behavior of the catheters. Young modulus, or material stiffness, is a measure of how much a material will deform when subjected to either compressive or tensile load. 5
Bose ElectroForce instrument setup.

Close-up of catheter sample in tensile grips of Bose instrument.
For both tests, samples were cut out of the catheters—longer samples for tensile tests and shorter samples for compressive tests. The geometry of the samples was measured and recorded. For tensile tests, the samples were clamped using the clamping grips of the BOSE ElectroForce load testing device, and for compressive tests, samples were held between flat platens of that device. Three samples were tested for each type of catheter without repeating from the same catheter. The principle of the load testing device was to apply displacement on the sample using its electromagnetic actuators and record the corresponding load on the load cell. The values for the maximum displacements were kept in the linear region (small amounts of stretch, consistent with the kinking phenomenon being studied) so that the materials could be assumed as linear elastic.
Results
Tables 1 and 2 show the results obtained from the load tests on the 16F and 12F catheters. In Tables 1 and 2, one can clearly observe (despite sample-to-sample variations in stiffness) that the silicone catheter material is significantly stiffer than either the regular latex or latex coude material. A stiffer material, simply put, is more resistant to kinking. This trend is illustrated in Figure 4, using the average stiffness values from Tables 1 and 2.
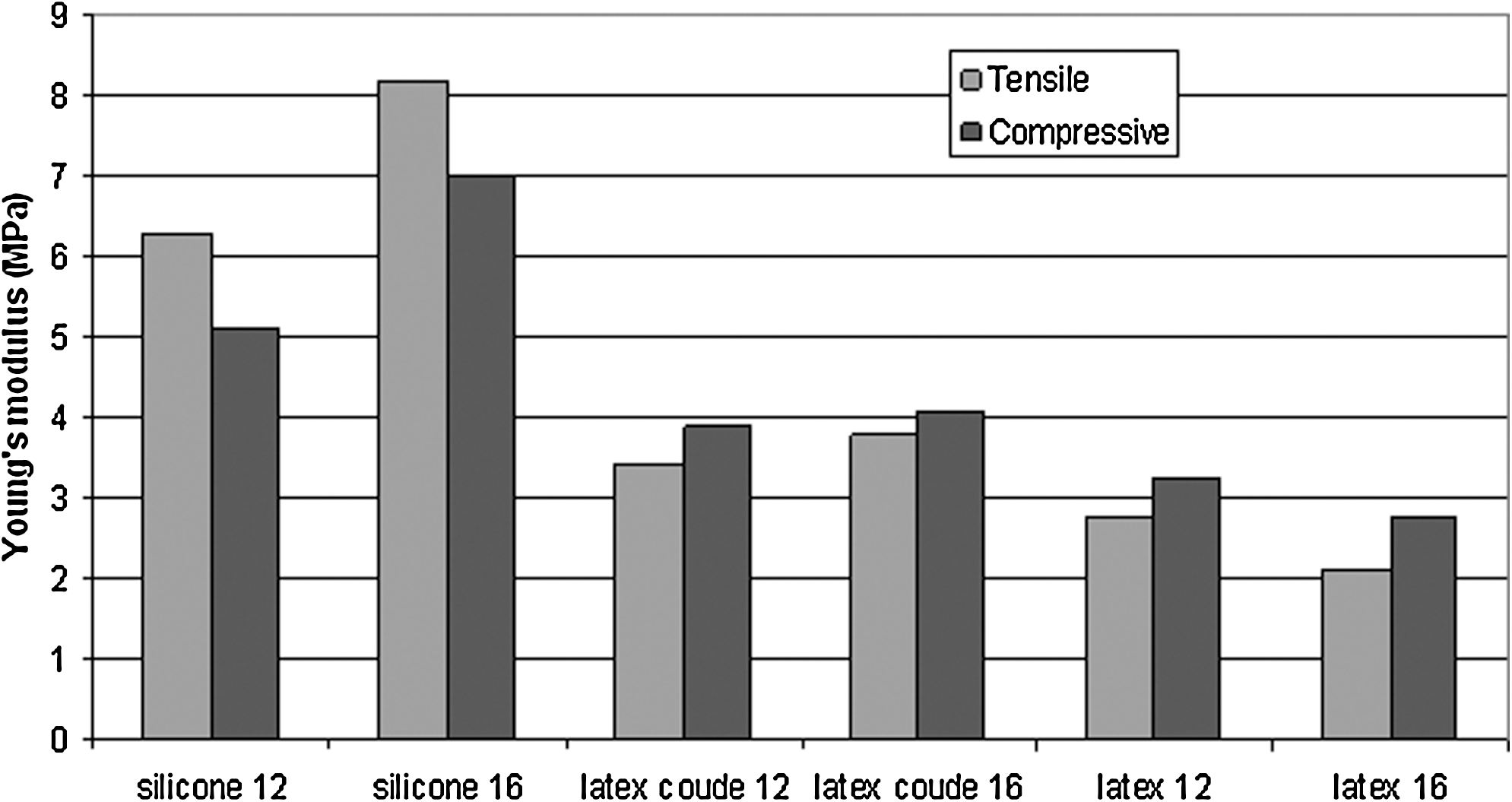
Stiffness values for three different catheter materials taken from two different size catheters.
Combining measurements of the tested catheter cross-sections with the compressive material stiffness data from Figure 4, the overall flexural rigidity, or resistance to kinking, is shown in Figure 5 for the different catheters tested. It is clearly observed that despite a larger cross-section contribution from the latex catheters, the stiffness of the silicone material causes it to dominate in overall flexural rigidity.

Model prediction of resistance to kinking for 16F catheters.
Discussion
Two factors play a role in the susceptibility to kinking of a urethral catheter. The first one is the stiffness of the catheter, which was addressed in Tables 1 and 2. The other factor that plays a role in susceptibility to kinking is the geometry of the specimen (primarily the cross-section shape of the catheter). When a catheter pushes against a stricture, it is analogous to a structural column holding up the weight of a building. The shape and size of the column determine how much load it can carry before it buckles. Likewise, the cross-section geometry of the catheter helps determine how much resistance it can overcome in the stricture without kinking. Thus, the resistance to kinking is related to the product of Young modulus and a geometric property called “second moment of area” or “area moment of inertia.” 5,6 Simply put, a catheter cross-section with material distributed away from its center (like a hollow tube) has a higher second moment of area than a catheter cross-section with material distributed at or near its center (like a solid cylinder), and will thus be more resistant to kinking. The combination of both factors is illustrated in Figure 5.
These experiments provide an explanation of why less urethral dilation is needed when using silicone catheters passed over Glidewires in clinical practice, because these catheters showed more than 50% greater resistance to kinking when compared with latex or coude catheters. We believe that when urethral dilation is needed in the setting of the DUC, it should be minimized to prevent complications and the smaller catheter passed over a Glidewire that could appropriately drain the bladder should be used. To achieve these goals, this study provides a basic science basis to recommend the use of silicone catheters in this setting.
There are other advantages to the use of silicone catheters. Silicone catheters are safe in cases of latex allergy. According to the Centers for Disease Control and Prevention catheter-associated urinary tract infections guideline, 7 silicone might be preferable to other catheter materials to reduce the risk of encrustation in long-term catheterized patients who have frequent obstruction. Silicone catheters are just slightly more costly than latex catheters, so cost should not be a consideration when using them.
Nevertheless, for the same reason that silicone catheters may be superior when passed over a wire (because of their increased stiffness as demonstrated in our experiment), they probably should not be used in all urethral catheterizations. Because of their stiffness, when advanced blindly without a Glidewire to guide them into the bladder, they can potentially cause more trauma than the regular softer latex catheters. In the case of a urethral stricture, for example, a silicone catheter can potentially cause a larger deeper false passage compared with a latex catheter if advanced forcefully.
Conclusion
Urethral dilation in the setting of the DUC carries many risks and can be very unpleasant to the awake patient. Urethral dilation is a suboptimal treatment for strictures or bladder neck contractures. Despite these drawbacks, dilation is occasionally needed to place a urethral catheter if suprapubic catheterization is to be avoided (patient receiving anticoagulants, etc.). When dilation of the urethra needs to be performed, dilating to the smallest size that would allow the passage of the smallest catheter that could drain the bladder appropriately can minimize trauma, pain, and other complications and potentially make a future urethroplasty easier. To achieve this goal, silicone catheters passed over a Glidewire should be the first choice, because they offer more resistance to kinking and thus may necessitate less dilation for the same size catheter compared with regular or coude latex catheters.
Footnotes
Disclosure Statement
No competing financial interests exist.