
Abstract
In patients with vesicouterine fistula (VUF), identification of the fistulous tract during laparoscopic surgery remains difficult. Hysterography and intravesical instillation of dye have been the traditional methods for diagnosing VUF; now, they have been supplanted by ultrasonography, CT, and/or MRI. Unfortunately, none of the above mentioned investigations aid in identification of the fistulous tract during laparoscopic surgery or ease laparoscopic dissection. We describe a simple procedure, which we term cystohysteroscopy, that aids the diagnosis of VUF and also simplifies laparoscopic dissection. A guidewire/ureteral catheter is coiled in the uterine cavity through the fistulous tract with the help of a cystoscope. By cystohysteroscopy, this guidewire/ureteral catheter is pulled out through the vagina using a semirigid ureteroscope. The advantage of cystohysteroscopy is that the presence of the guidewire/ureteral catheter across the fistulous tract aids laparoscopic dissection even in the presence of fibrosis and can be used for traction/manipulation during dissection in the vesicouterine area. This is the first report in the literature depicting the use of a semirigid ureteroscope for the purpose of cystohysteroscopy.
Introduction
The visualization of an orifice in the bladder during cystoscopy strengthens the clinical diagnosis. A guidewire may be passed through the fistula and its coils can then be detected on fluoroscopy (Fig. 1). This is suggestive of VUF but cannot confirm the site of the fistulous opening inside the uterus.
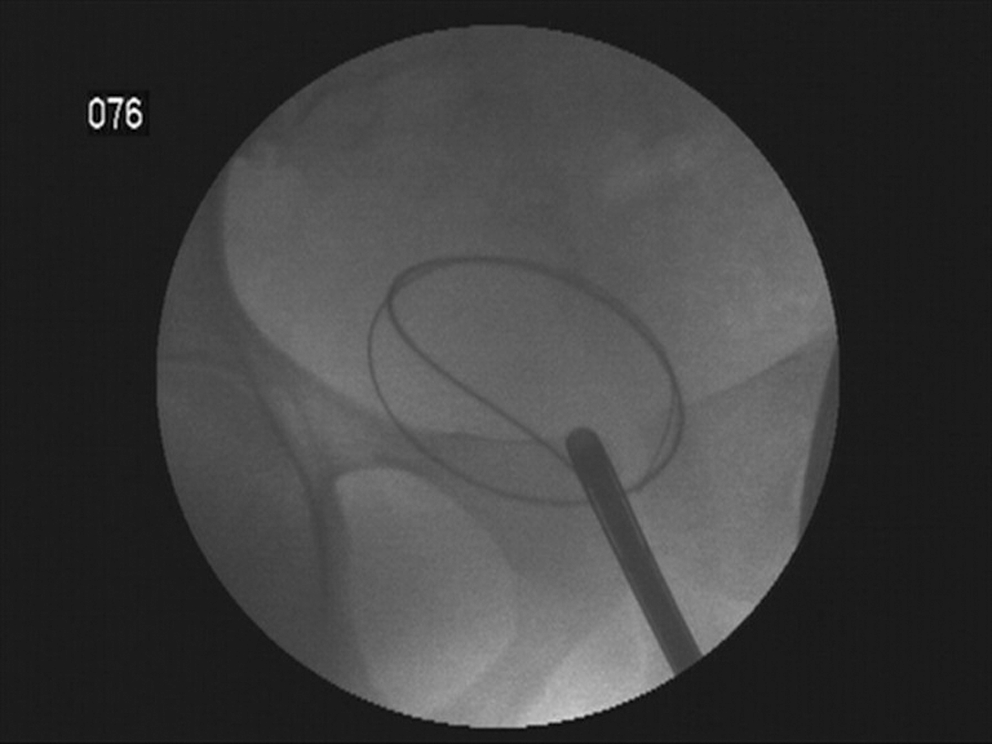
Fluoroscopic view showing oval coil of the ureteral catheter/guidewire.
Ultrasonography is a noninvasive method of demonstrating VUF but needs a high level of expertise. Doppler ultrasound may improve the diagnostic yield by assessing the flow of fluids between the two hollow cavities and may demonstrate the size and site of a fistula. Drawbacks of ultrasonography are that it is operator dependent and might miss small fistula. CT with intravesical instillation of contrast may demonstrate VUF but emits radiation that might be hazardous for the potentially fertile females. MRI is the investigation of choice for demonstrating VUF, but its limitations are availability and cost. The drawback of the above mentioned radiologic modalities is that none of them can help in identification of the fistulous tract during laparoscopic surgery. 1,2
Hysteroscopy has been described in the literature for confirming the diagnosis of uterine fistula that are visualized on CT. 3 We describe the technique of cystohysteroscopy, which is performed with a semirigid ureteroscope under anesthesia (general or spinal) to confirm the diagnosis of VUF preoperatively and also aid in laparoscopic dissection.
Technique
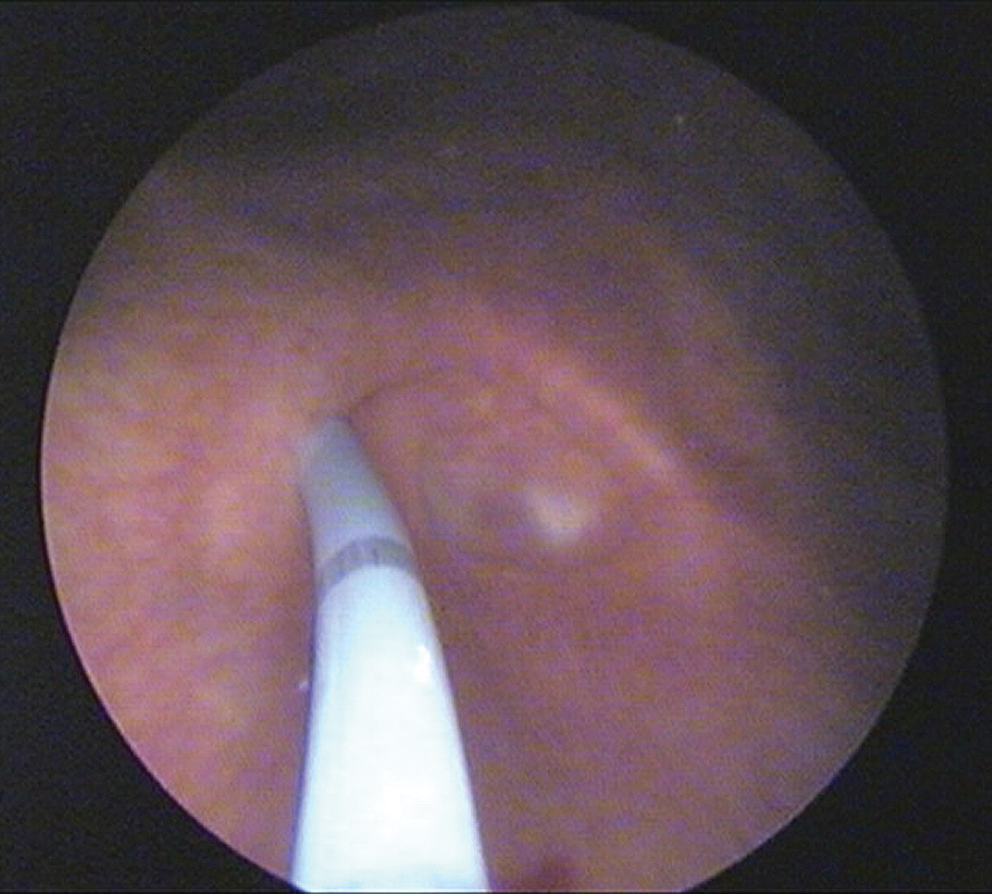
A woman, aged 34 years, presented with cyclical menouria of 10 years' duration after LSCS performed 10 years previously. Her clinical history and per-vaginal examination were suggestive of VUF. Cystoscopy revealed an orifice (10 mm in diameter) in the supratrigonal region (Fig. 2). A 6F ureteral catheter over a Terumo guidewire was inserted through the fistula (Fig. 3). Fluoroscopy showed the oval coil of the ureteral catheter/guidewire suggestive of coiling inside the uterine cavity (Fig. 1). A Sims vaginal speculum was used to retract the posterior vaginal wall. The anterior cervical lip was then grasped with vulsellum forceps. Subsequently, the cervical os was dilated with Hegar dilators. Then, a 7.5F ureteroscope (Wolf) was introduced inside the uterine cavity, and the ureteral catheter/guidewire (Fig. 4) was grasped with flexible forceps and brought out through the vagina. The ureteroscope was reinserted in the uterine cavity to visualize and confirm the point of entry of the ureteral catheter/guidewire, which was in the lower anterior part of the body of the uterus.
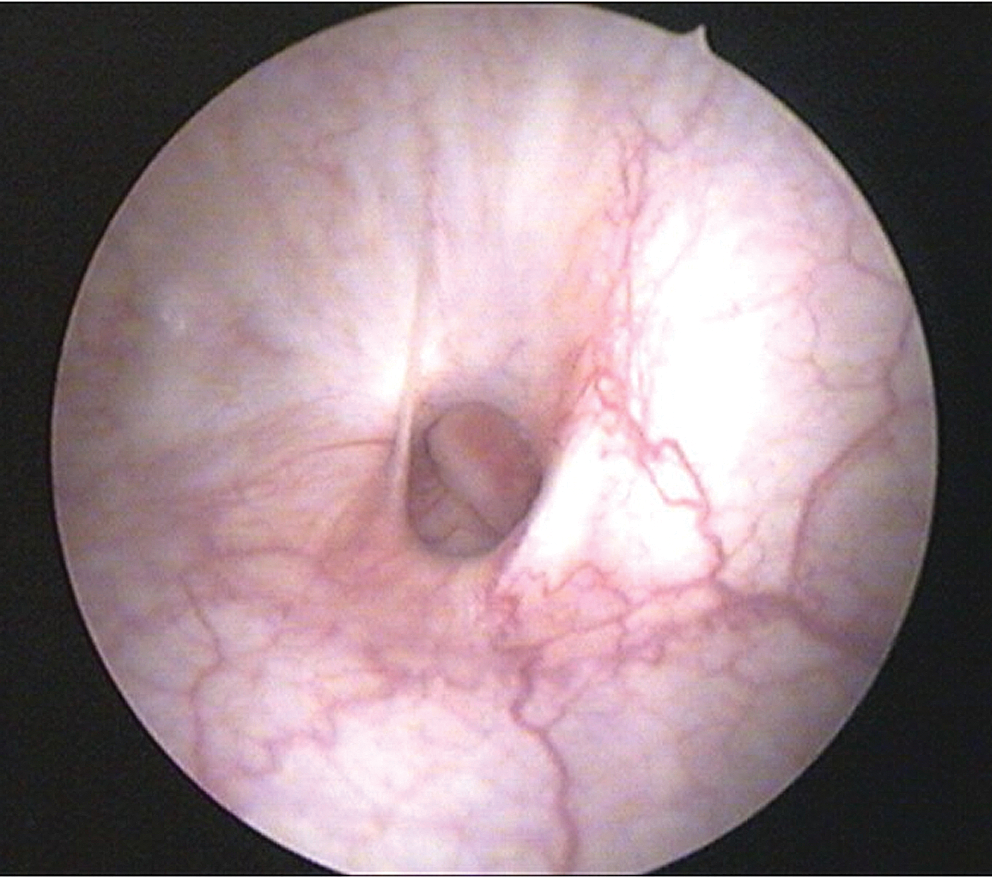
Cystoscopic view of the vesicouterine fistula orifice on the posterior wall of the urinary bladder.
Cystoscopic view showing the ureteral catheter inside the vesicouterine fistula.

Hysteroscopic visualization of the ureteral catheter/guidewire inside the uterine cavity with the aid of a semirigid ureteroscope.
After this, the patient was maintained in the supine position with head tilted downward. Pneumoperitoneum was established; a 12-mm camera port was inserted in the midline just below the umbilicus, and two 5-mm ports were inserted lateral to the rectus abdominis (halfway between the umbilicus and the anterior superior iliac spine). The vesicouterine fold of the peritoneum was reflected, and a plane between the urinary bladder and anterior surface of the uterus was created. The patient subsequently underwent laparoscopic fistula disconnection, closure of the bladder and uterine fistulous openings, and interposition of vesicouterine fold of peritoneum.
The presence of the ureteral catheter/guidewire between the uterus and the bladder helped in identification of the tract intraoperatively, even in the presence of fibrosis. Because both ends of the ureteral catheter/guidewire were outside the body, they could be secured easily, and there was no danger of slippage of the ureteral catheter or guidewire during the laparoscopic procedure. The ends were used for traction/manipulation during dissection in the vesicouterine area and were of immense help in laparoscopic surgery. The ureteral catheter/guidewire was pulled out after the fistulous orifice of the uterine end was properly identified and dissected before closure.
The main advantage of this technique is through-and-through establishment of access between bladder and vagina via the fistulous tract. The presence of the ureteral catheter and its manipulation aids in laparoscopic dissection of tough fibrous tissue and also helps in identification of the fistulous site by visible movement of the tissues during traction of the ureteral catheter. Thus, cystohysteroscopy in the preoperative period made the subsequent laparoscopic repair much easier to perform. The patient is doing well as per her last follow-up at 1 year and has started menstruating per vaginum.
Footnotes
Disclosure Statement
No competing financial interests exist.