
Abstract
Purpose:
To describe our experience with robot-assisted laparoendoscopic single-site (R-LESS) surgeries and evaluate a homemade port system as an effective access technique.
Patients and Methods:
Between May 2009 and April 2010, 68 consecutive R- LESS urologic operations were performed in our institution. A 4 to 5 cm long incision was made over the umbilicus. After the inner ring of the Alexis wound retractor was placed into the peritoneum, a common size 7 surgical glove was then applied over the external side of the wound retractor. A homemade single port was established by inserting two 12-mm trocars and two 8-mm trocars through fingers of a surgical glove and securing it to the port.
Results:
Sixty-eight patients underwent R-LESS, including partial nephrectomy in 51, nephroureterectomy in 12, radical nephrectomy and adrenalectomy in 2 each, and simple nephrectomy in 1. Mean patient age was 56 years (range 16–81 y). Mean body mass index was 23.9 kg/m2 (range 17.2–32.9 kg/m2). The mean operative time was 219 minutes (range 109–382 min). Mean estimated blood loss 319 mL (range 50–1550 mL), and change in hematocrit was 5.2 % (range 0.0–14.8%). At a mean follow-up of 8 months, there were no port-related complications, and cosmesis was excellent.
Conclusions:
R-LESS is feasible and can be safely applied to a variety of urologic operations, considering the low intraoperative complication rate. Our homemade single-port device provides adequate range of motion and is more flexible in port placement for R-LESS than the current multichannel port.
Introduction
Natural orifice translumenal endoscopic surgery (NOTES) is regarded as the pinnacle of minimally invasive surgery. Intra-abdominal surgery can be performed without any transabdominal incision. Purposeful incisions are made in the body's hollow viscera (stomach, bladder, vagina, and rectum) to gain access to and perform surgery intraperitoneally. Even with the successful performance of the first human pure transvaginal NOTES nephrectomy, 2 however, this technique still remains largely experimental.
Laparoendoscopic single-site (LESS) surgery uses a single incision to perform intra-abdominal procedures. The incision is usually made at the umbilicus to maximize the cosmetic benefit. LESS has had wider acceptance than NOTES because of the familiarity with the surgical view, wider extracorporeal space to work with, and availability of newly developed tools to perform LESS. Because of the loss of triangulation and instrument clashing, however, difficulties persist in performing LESS surgery.
With its seven degrees of freedom of motion, its three-dimensional vision, and motion scaling, the da Vinci (Intuitive Surgical, Sunnyvale, CA) surgical robotic platform has been applied to LESS surgery in an attempt to offset the difficulties in performing the latter. We have previously reported the feasibility of robot-assisted LESS (R-LESS) using a homemade single port device 3,4 and now present an update on our experience.
Patients and Methods
Study design
Between May 2009 and April 2010, 68 consecutive R-LESS urologic operations were performed in our institution. Data were prospectively entered in an Institutional Review Board-approved LESS database and retrospectively reviewed. Any patient who was fit for conventional laparoscopic or robot-assisted surgery was offered R-LESS and thoroughly informed of the available options along with its risk and benefits.
Perioperative data, including preoperative diagnosis, surgical indication, operative time, estimated blood loss, intraoperative and postoperative complications, conversion to conventional laparoscopic or open surgery, and length of hospital stay, were recorded. The operative time was measured from the first skin incision to skin closure.
Port placement
The patient was placed in a 45-degree flank position and secured to the operating table (Fig. 1). The table was tilted to position the patient supine, and a 4 to 5 cm midline periumbilical incision was carried down through the peritoneum. The fascial incision was slightly larger at 5 to 6 cm. The homemade single port was constructed and applied similarly to that described by Jeon and colleagues. 3 An Alexis® wound retractor (Applied Medical, Rancho Santa Margarita, CA) was placed through the incision. A common size 7 surgical glove was then applied over the external side of the Alexis wound retractor, and four trocars, including two 12-mm trocars (the third and fourth fingers) and two 8-mm robotic trocars (the first and fifth fingers), were inserted and secured through incisions on the fingertips of the surgical glove (Fig. 2). With the patient in a 90-degree flank position, pneumoperitoneum was achieved through the 12-mm port inserted to the fourth finger of the glove for insufflation and as an assistant port. To maximize triangulation, a 30-degree upward viewing robotic laparoscope was inserted over a 12-mm trocar inserted through the third finger of the glove and fixed to the uppermost portion of the homemade port toward the same side as the lesion. Two 8-mm robotic ports were inserted through the first and fifth fingers of the glove and fixed inferolaterally on both sides to allow maximum distance between the ports.
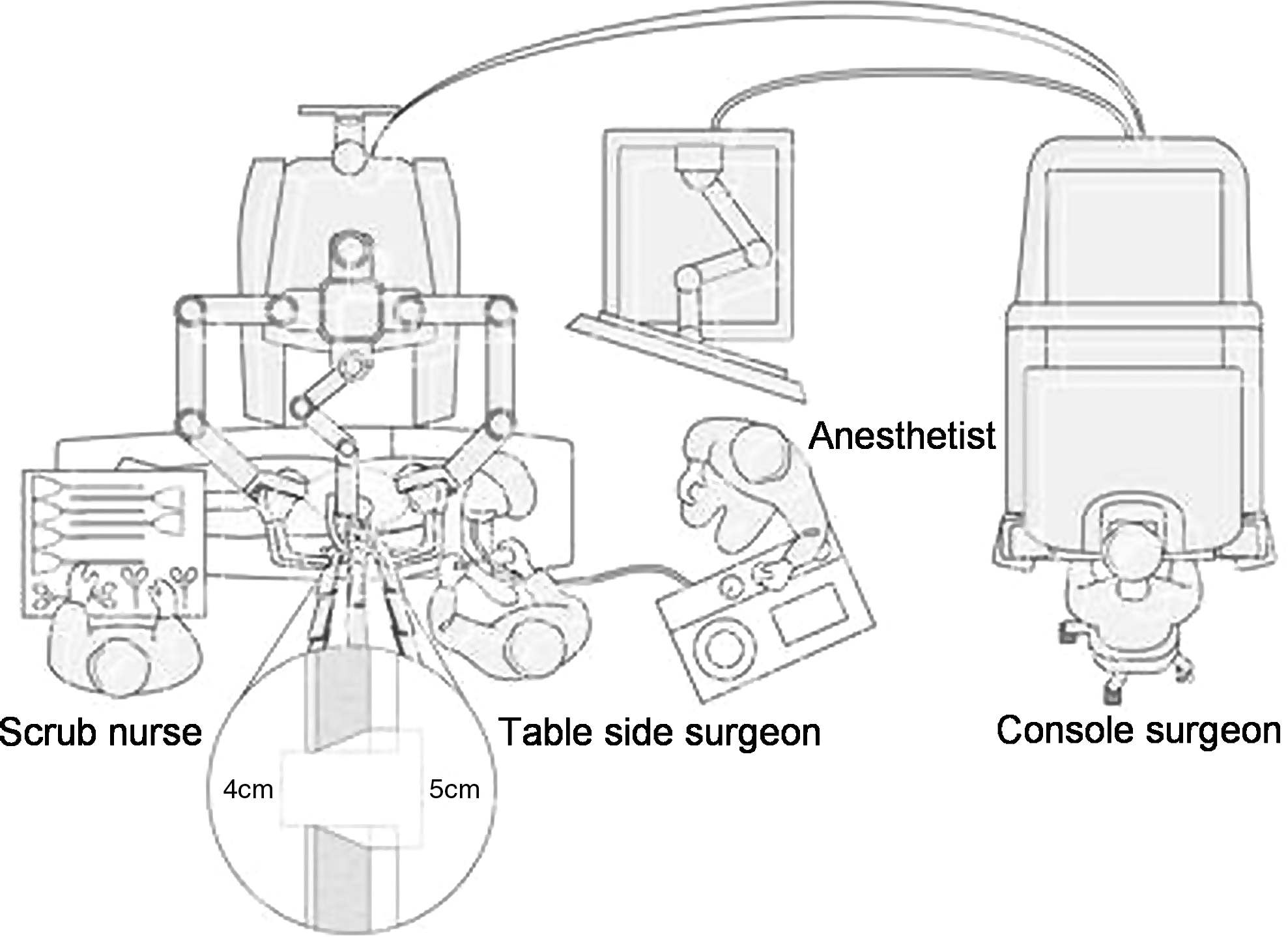
General operating room setting of robot-assisted laparoendoscopic single-site surgery for left-side pathology.
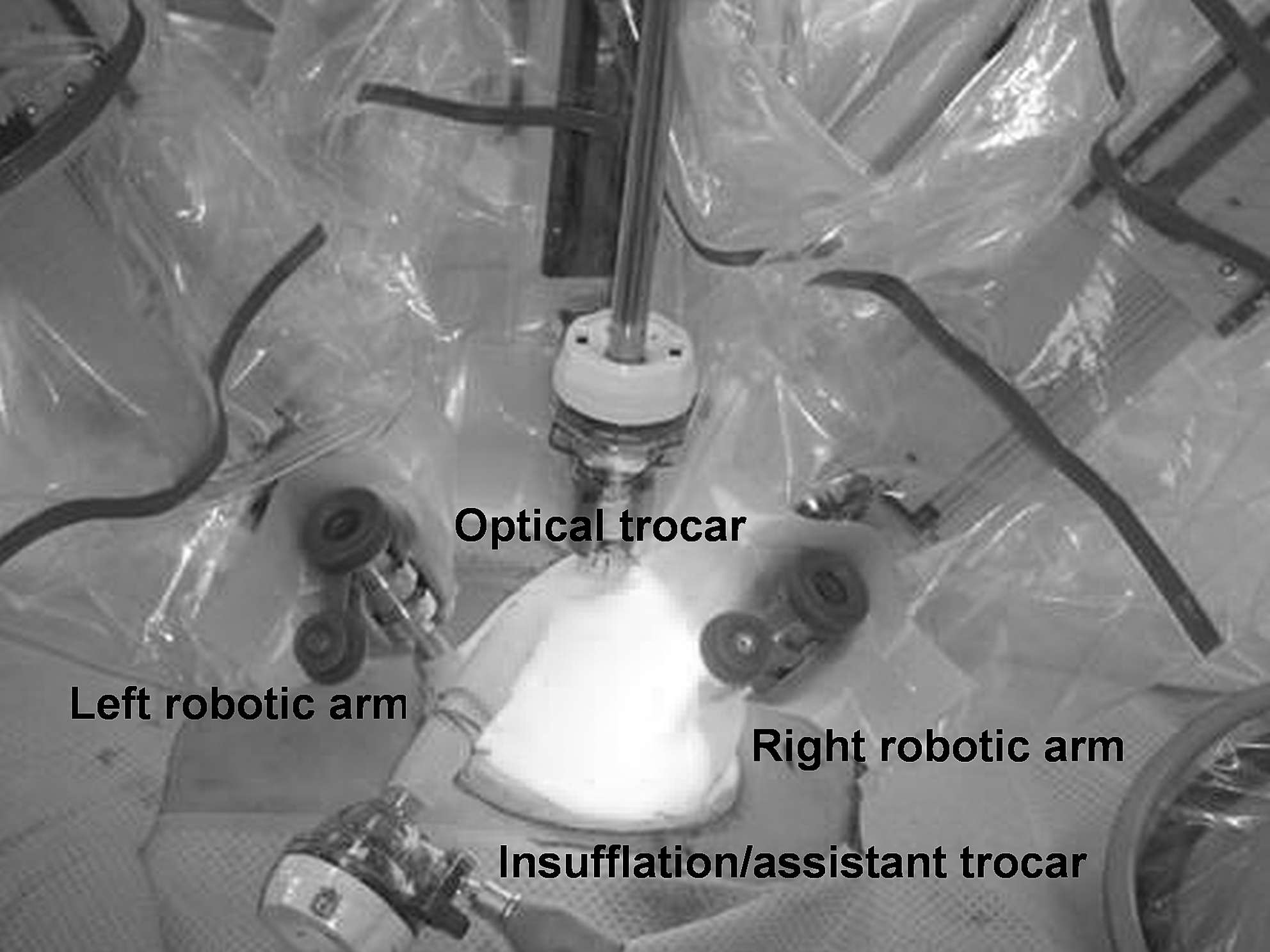
External view of homemade single port device after docking of the da Vinci surgical robotic system.
Surgical technique
The patients included in this study underwent R-LESS using the da Vinci surgical robotic platform. Standard robotic instruments were used. The surgical technique for R-LESS was the same as conventional robot-assisted surgery.
Renal dissection was conducted in the conventional laparoscopic technique. For simple and radical nephrectomy, the renal pedicles were dissected, and the renal artery and vein were controlled using Hem-o-lok® clips or a 12-mm endovascular GIA stapler. For partial nephrectomy, intraoperative ultrasonography was used to identify the size and margins of the tumor. The ultrasonoraphic images were projected onto the console screen to guide tumor resection. Temporary occlusion of the renal artery and vein was performed by placement of laparoscopic bulldog clamps. The tumor was then excised using the Endowrist® Hot Shears monopolar scissors (Intuitive Surgical, Sunnyvale, CA). Frozen section biopsy specimens of the tumor base were taken. Hemostasis was achieved with intracorporeal suturing, sliding clip renorrhaphy using Hem-o-lok clips. 5
For nephroureterectomy, the nephrectomy was performed as described previously. The ureter was then dissected down to the ureterovesical junction; 2–0 polyglactin stay sutures were placed on the 12 and 6 o'clock positions on the bladder side of the junction. The ureter was clipped close to the junction to prevent spillage, and a cuff of bladder mucosa was resected around the ureteral orifice. The bladder defect was then closed in two layers using the previously placed stay sutures. The integrity of the bladder closure was tested by filling the bladder with 150 to 200 mL of physiologic saline.
For adrenalectomy, the renal vein (or inferior vena cava) and adrenal vein were dissected free. The adrenal vein was dissected out and divided; 5-mm surgical metal clips were used to control the adrenal vein. Adrenal arterial supply and remaining attachment to the kidney is divided with the Endowrist Hot Shears monopolar scissors.
The specimens were extracted in an entrapment bag through the umbilical incision without extension.
Results
Sixty-eight patients underwent R-LESS, including partial nephrectomy in 51 (75%), nephroureterectomy in 12 (18%), radical nephrectomy and adrenalectomy in 2 (3%) each, and simple nephrectomy in 1 (1%). Table 1 shows the surgical indication and/or final pathologic diagnosis of R-LESS. Mean patient age was 56 years (range 16–81 y). Mean body mass index was 23.9 kg/m2 (range 17.2–32.9 kg/m2). The mean operative time was 219 minutes (range 109–382 min). Mean estimated blood loss was 319 mL (range 50–1550 mL), and change in hematocrit was 5.2% (range 0.0–14.8 %). Mean length of stay was 4.5 days (range 1–16 d).
Table 2 lists the intraoperative and early postoperative data. For partial nephrectomy, mean ischemia time was 27 minutes (range 12–65 min). Only two cases of partial nephrectomy were performed without hilar clamping. One case had a positive surgical margin. At 9 months postoperatively, there was no clinical evidence of cancer recurrence in this patient. Three intraoperative complications occurred. One renal vein injury and one ureteral injury occurred in partial nephrectomy. One bowel injury (serosal tearing) occurred during adhesiolysis in simple nephrectomy. Renal vein, ureter, and bowel serosal tearing were sutured via the single port. We had to convert three cases to minimal-incisional open access. After R-LESS for partial nephrectomy, one case was converted to open radical nephrectomy because of delayed bleeding in the hilar vessels. In another case of partial nephrectomy, the endophytic tumor was located in the right posterior upper pole. Because robot arms could not access with a sufficient degree of length, mini-incisional partial nephrectomy was performed accordingly. A case of radical nephrectomy of leiomyosarcoma was converted to mini-incisional open access because of severe perirenal adhesion. At a mean follow-up of 8 months, there were no postoperative hernias or delayed complications, and patient-reported cosmesis was excellent.
All cases were converted to mini-incisional open procedure.
Hct=hematocrit.
Discussion
With its seven degrees of freedom of motion, its three-dimensional vision, and motion scaling, the da Vinci surgical robotic platform has been applied to LESS surgery in an attempt to offset the ergonomic challenge. To our knowledge, our present experience constitutes the largest reported series of R-LESS for upper urinary tract surgery to date. Our results continue to prove that the da Vinci robot system can facilitate LESS surgery. It is worthwhile to note that compared with our previous report, 3 the greatest increase in the number of cases is in partial nephrectomy (11–51). This reflects the prevailing philosophy toward nephron-sparing surgery; that is, to perform partial nephrectomy whenever possible. 6 Whereas previously, partial nephrectomy was performed only for T1a tumors, at present, perhaps because of increased surgeon confidence drawn from the greater maneuverability afforded by the robot, availability of advanced hemostatic technology, and accumulated experience, larger, more complex renal tumors are also being managed by partial nephrectomy.
We made a 4 to 5 cm skin incision and a 5 to 6 cm fascial incision, and this may be a rather large incision size, particularly for partial nephrectomy. In a matched-pair analysis, we have compared our technique with standard trocar placement in robot-assisted partial nephrectomy and have found comparable operative outcomes. There were nonstatistically significant higher pain scores on the first postoperative day (4.5 vs 4.0, P=0.275) and in-hospital morphine requirements (130.5 vs 119.2 mg, P=0.415) in the R-LESS group (unpublished data).
As shown by our results, mean estimated blood loss was 319 mL (range 50–1550 mL), and change in hematocrit was 5.2% (range 0.0–14.8%). Seven (14%) patients from the partial nephrectomy group needed a blood transfusion. This resulted mainly from heavy bleeding noted during tumor excision from inadequate vascular control. In a case of partial nephrectomy, estimated blood loss was up to 1550 mL because of renal vein injury, and the patient needed a blood transfusion of 4 units. This made the partial nephrectomy and parenchymal suturing more challenging and time consuming. This highlights the importance of meticulous hilar dissection and accurate placement of the vascular clamps.
In our study, the mean length of hospital stay after R-LESS was much longer than that reported in the literature and similar to our non-LESS cases. This is because of the characteristics of medical insurance in Korea. Korean public medical insurance covers most of the medical expenses for a ward. For example, in cases of a five-patient ward to which the insurance cost is applied, the daily medical expenses per person for a ward would be $11. Accordingly, most patients do not leave the hospital until they can return to normal activity. Also, we wanted to observe the patients to ensure the safety and efficacy of this new technique.
Even though the feasibility of conventional umbilical LESS adrenalectomy has been demonstrated, 7,8 the distance between the umbilicus and the adrenal gland makes it difficult to perform delicate dissection in the area of the adrenal gland. As such, cases of retroperitoneal LESS have been reported because of the shorter distance between the single port and the adrenal gland. 9 In the present series, we were able to perform two cases of adrenalectomy. To our knowledge, this is the first time that robot-assisted adrenalectomy performed through a single port has been reported in the literature. From our experience, the length of the robot instruments and the increased dexterity afforded by the Endowrist® (Intuitive Surgical, Sunnyvale, CA) make it possible to comfortably perform robot-assisted adrenalectomy through the umbilicus. Because the added cost of using the robot remains prohibitive, however, the benefit of robot-assistance in single-port adrenalectomy must be studied further.
Throughout our R-LESS experience, we have used the homemade single-port device. One of its disadvantages in conventional LESS is the lack of a fixed fulcrum through which the instruments can be maneuvered. In R-LESS, this is less of a problem, because the system maintains a fulcrum at a fixed point in the robotic trocar once the system is docked. Another disadvantage of the homemade single-port device is its fragility because of the use of a standard glove. We have experienced accidental tears when inserting/reinserting the robot instruments and ballooning at high insufflation pressures (20 mm Hg). Accidental tears occur when the inner edge of the robotic trocar is partially or wholly occluded by the glove. To prevent this from occurring, during construction of the homemade-single port device, the robotic trocar should be fixed in such a way that its inner edge is well beyond the base of the finger of the glove. During docking, it must be ensured that the robotic port be positioned so that the fixed point approximates the level of the abdominal wall and that no part of the inner edge of the port is in contact with any part of the homemade single-port device. Ballooning can be prevented by avoiding use of high insufflation pressures as an adjunct for achieving hemostasis. Overall, the homemade single-port device is a safe, effective, low-cost alternative to commercial single-port devices.
The current da Vinci surgical system was not designed for LESS. As such, difficulties are still commonly encountered in R-LESS. Some of the suggestions to reduce collisions are: Using the daVinci S with its improved range of motion, setting the system to fine-tuning mode to reduce external movement of the robot arms, use of a 30-degree upward configuration of the robotic scope, and the use of 5-mm pediatric robotic instruments. Even with the numerous ingenious modifications made, however, inherent limitations make the system less than ideal for LESS. We have kept these occurrences at a minimum by making more than a 4-cm incision and placing the laparoscope port and the two robotic ports as far away from each other as possible on the homemade single-port device.
Recently, the Cleveland Clinic reported on the use of newly developed instruments designed for single-site surgery using the da Vinci Si system. 10 The VeSPA surgical instruments (Intuitive Surgical, Sunnyvale, CA) have a semirigid shaft that allows it to be deployed through two curved crossing cannulae on a prototype multichannel port (Intuitive Surgical, Sunnyvale, CA), providing triangulation intraperitoneally. Compared with the EndoWrist instruments, however, these new instruments are not equipped with an articulating tip, effectively reducing the range of motion. In spite of this, they were used to successfully performed 16 R-LESS (4 pyeloplasties, 4 partial nephrectomies, and 8 nephrectomies) in four female farm pigs. There were no additional ports inserted, and no conversion needed. The warm ischemia time for partial nephrectomy was 14.8 minutes while the total operative time for all procedures averaged 110 minutes. The mean blood loss was only 20 mL, and there were no intraoperative complications. Only minimal instrument clashing was experienced. Further improvements should be made, because several limitations were noted, such as significant gas leak, tearing of the multichannel port, and limited space for movement for the tableside surgeon.
The efficacy, safety, and benefit of R-LESS surgery should be proven by larger studies before fully embracing this technique. Validated outcome measurement tools for quality of life, postoperative morbidity, and aesthetic issues specific for LESS robot-assisted surgery should be developed to determine its advantages over conventional techniques. 11
Conclusions
R-LESS is feasible and can be safely applied to a variety of urologic operations, considering the low intraoperative complication rate. Our homemade single-port device provides adequate range of motion and is more flexible in port placement for R-LESS than the current multichannel port. The homemade single-port device's flexibility and 30-degree upward viewing robotic laparoscope may help to reduce robotic arm collisions.
Footnotes
Disclosure Statement
No competing financial interests exist.