
Abstract
Background and Purpose:
Calculi from patients with musculoskeletal (MS) anomalies who are largely immobile and prone to urinary infections have been traditionally composed primarily of struvite and carbonate apatite. Because of substantial improvements in the care of these patients in recent decades, stone etiology may have shifted from infectious to metabolic. We assessed the composition of renal calculi and metabolic characteristics in a contemporary cohort of patients with MS anomalies who underwent percutaneous nephrolithotomy (PCNL).
Patients and Methods:
Retrospective analysis of patients who underwent PCNL between April 1999 and June 2009 and had follow-up 24-hour urine studies was performed. Patients with MS anomalies included spinal cord injury, myelomeningocele, muscular dystrophy, multiple sclerosis, cerebral palsy, or other clinical syndromes causing kyphoscoliosis and contractures.
Results:
Our cohort included 33 patients with MS anomalies and 334 consecutive patients as a control group who underwent PCNL and had metabolic workup. Stones were infectious in etiology in 18.4% and 6.2% in MS and control groups, respectively. Thus, most patients harbored stones of metabolic origin. Metabolic stones in the MS group were composed of 52.7% hydroxyapatite, 10.5% calcium oxalate, 7.9% brushite, 2.6% uric acid, 0% cystine, and 7.9% other. Metabolic stones in the control group were 50.5% calcium oxalate, 16.4% hydroxyapatite, 11.5% brushite, 10.8% uric acid, 4.3% cystine, and 0.3% other. Mean 24-hour urine values for patients with metabolic stones in MS/control groups were volume 2.18/1.87 L/d, pH 6.78/6.05, calcium to creatinine ratio 220/151 mg/g, and oxalate 44.8/39.5 mg/d.
Conclusions:
Although patients with MS anomalies are traditionally thought to harbor infection-related calculi, most will be found to have calculi of metabolic etiology. The incidence of calcium phosphate stones is high in this group of patients, perhaps reflecting their high urinary pH.
Introduction
Stones from patients with musculoskeletal (MS) anomalies have traditionally been composed primarily of struvite and carbonate apatite, presumably as a result of chronic bacteriuria with urea-splitting organisms. 2,3 Most reports dealing with stone composition in these patients are at least 25 years old and, since the time of their publication, there has been a substantial improvement in the care of these patients. 4 Several more contemporary reports 1,5 have suggested that many patients with MS anomalies will be found to have stones of metabolic origin.
Our goal was to evaluate the stone composition in patients with MS anomalies and to seek a possible metabolic explanation for their persistently high incidence of stones.
Patients and Methods
Our database approved by the Institutional Review Board (IRB# 03-096) was used to identify all patients who were undergoing percutaneous nephrolithotomy (PCNL) for renal calculi at Indiana University Health Methodist Hospital. Between April 1999 and June 2009, 991 patients underwent PCNL and were included in the database. Among these, 367 (37%) patients had at least two 24-urine collections and were used for our analysis.
We identified subjects with MS anomalies. These included patients with myelomeningocele (MM), SCI, multiple sclerosis, cerebral palsy, or other clinical syndromes causing significant kyphoscoliosis and contractures. Patients with no history of MS anomalies were used as controls.
All patients underwent urine culture testing and received at least 1 week of tailored antibiotic therapy before undergoing PCNL. Any degree of urinary colonization was considered clinically significant, and patients were treated according to the urine culture sensitivity reports for at least 1 week before surgery.
Percutaneous access was obtained using a triangulation technique, which we have described previously. 6 After cystoscopic placement of a ureteral catheter, percutaneous access was performed by the urologist as part of a single-stage procedure. Access was performed using an 18-gauge needle and biplanar fluoroscopy. The nephrostomy tract was dilated to 30F in all cases with a NephroMax™ balloon (Boston Scientific Corp, Natick, MA). An Amplatz sheath was used in all cases. Rigid and flexible nephroscopy were performed in all cases, and the intrarenal collecting system was mapped in an effort to render the patient stone free at the time of the initial procedure, if possible.
Stone fragments for stone culture were collected using sterile graspers. Stone fragments were then immersed in a cup containing sterile saline, crushed with a sterile needle holder, and sent for culture. In most cases, a 10F cope loop nephrostomy tube (Cook Urological, Spencer, IN) was used after PCNL. Patients in whom residual fragments were identified on post-PCNL CT underwent second-look nephroscopy typically within 48 hours after the initial procedure.
Stone analysis was performed in all cases by Fourier transform infrared microspectroscopy (Beck Analytical Services, Indianapolis, IN). Stone composition groups were assigned by the most prominent crystal identified within the stone. When any amount of struvite was present, the patient was assigned to the infectious stone group. Serum studies and 24-hour urine collections were performed by a commercial laboratory (Litholink Corp., Chicago, IL). Two to 14 collections (average 5.2) were performed for each patient, and the collection closest to the date of surgery was chosen for our analysis.
A two-tailed Student t test, chi-square test, or Fisher exact test was used as appropriate. A P value < 0.05 was considered statistically significant.
Results
A cohort of 33 patients (20 male and 13 female) with MS anomalies was identified. Mean patient age was 41 years (range 13 to 78 y). Two patients in the MS group and one in the control group were younger than 18 years. Etiology for MS anomalies in the study group is presented in Table 1. The majority of patients had previous SCI. The mean time from SCI to the time of PCNL was 21 years (range 4 to 34 y). MM accounted for the neurologic lesion in seven patients. Patients in the control group were older and had a larger body mass index, as depicted in Table 2. Stone burden, however, did not differ between the groups.
Mean values are presented.
MS=musculoskeletal; BMI=body mass index; N/S=nonsignificant.
Infection data
Stones were sent for analysis in all patients in the MS group and in 96.5% of patients in the control group. In the MS group, there were six (18.7%) patients who harbored infection-related calculi, defined as pure struvite, a mixture of struvite and apatite, or pure carbonate apatite. Seventeen (5.0%) patients in the control group had infection stones. Thus, the majority of patients in both groups had noninfectious calculi (Fig. 1). Preoperative urine culture was positive in most patients in the MS group, with more than 80% harboring infection in their urine. In contrast, only about a third of patients in the control group had preoperative positive urine culture (Table 2).
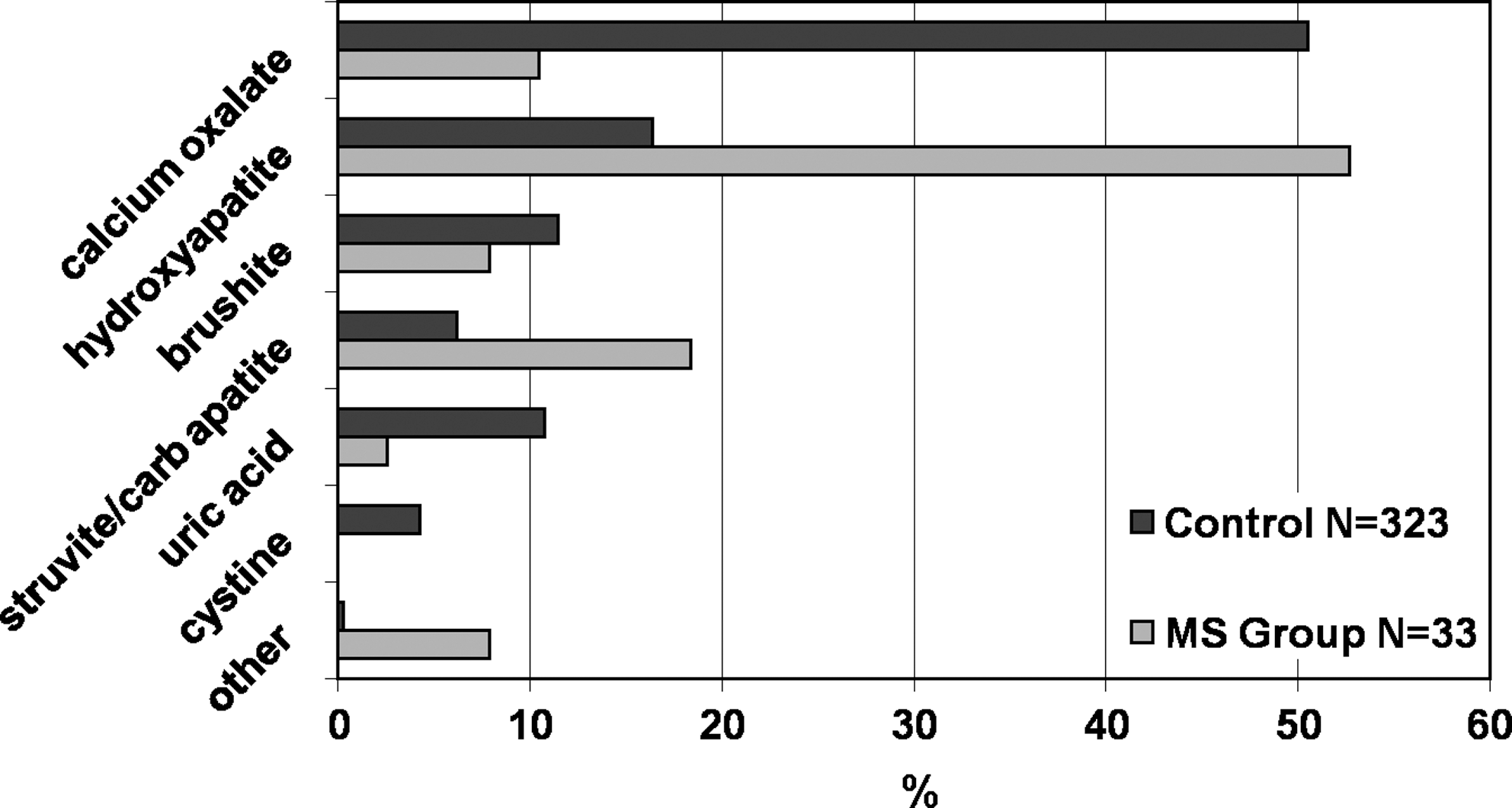
Stone composition in musculoskeletal and control groups.
Stone culture was sent for analysis intraoperatively in 64% of patients. A larger percentage of patients in the MS group had positive stone culture, and the difference was statistically significant (Table 2). All seven patients in the MS group who harbored infection-related calculi had both their urine and stone cultures positive. In the control group, patients with infection stones had positive urine and stone culture in 72% and 64% of cases, respectively.
Metabolic data
Metabolic stones in the MS group were composed of 52.7% hydroxyapatite, 10.5% calcium oxalate, and 7.9% brushite. In contrast, metabolic stones in the control group were composed of 50.5% calcium oxalate, 16.4% hydroxyapatite, and 11.5% brushite (Fig. 1). As expected, the incidence of uric acid stones was lower in MS patients. None of the patients in the MS group harbored cystine stones (Fig. 1).
Serum and 24-hour urine studies in the MS and control groups are presented in Table 3. Patients with infection stones were excluded from this analysis. Patients in the MS group had lower creatinine levels and higher 24-hour urine volume, as well as lower urinary calcium levels. Patients in the MS group had comparable serum CO2 and lower urinary citrate values. Urinary pH was significantly higher in the MS group.
Patients with infection stones were excluded. Mean values are presented.
Cr=creatinine; Ca=calcium; Mg=magnesium; CO2=carbon dioxide; Vol=volume; Ox=oxalate; Na=sodium; Phos=phosphorous; SSCaOx=calcium oxalate supersaturation; SSCaPhos=calcium phosphate supersaturation; MS=musculoskeletal; N/S=nonsignificant.
Discussion
Renal stones are an important cause of morbidity in patients with MS anomalies. It has been suggested that stone formation is usually a result of infected urine, secondary to incomplete bladder emptying, vesicoureteral reflux, catheterization, neurogenic bladder, or foreign bodies. 7 In one study, renal stones developed in 73 of 150 catheterized (49%) patients with SCI. 8 Another study has shown a higher incidence of renal stones, in 18 of 56 catheterized (32%) patients with SCI, vs 6 of 86 uncatheterized (7%) patients. 9 These studies, however, did not report the stone composition.
Matlaga and associates 5 published an observational study on 32 patients with neurogenic bladders from MM or SCI. Only 37.5% of patients harbored infection calculi. In their series, all patients with chronic indwelling suprapubic or urethral catheterization had harbored struvite stones. Clean intermittent catheterization or urinary diversion via ileal conduit appeared to be less associated with this stone type.
In evaluating stone composition reported in our current series, we have noted that only six (18.7%) patients of the MS group harbored infection-related calculi. This may be attributed to improved bladder management techniques during recent decades. We can hypothesize that significant advancement in urologic care of these patients has contributed to the change in stone composition. Modern urodynamic testing allows rapid assessment of the urinary tract. The greater use of clean intermittent catheterization and bladder augmentation techniques has allowed many patients who were formerly at risk for upper tract deterioration now to be maintained with low pressure urinary tracts. Indeed, the frequency of death from renal failure in patients with SCI has decreased in recent years. 10
More than 50% of patients in the MS group harbored calcium phosphate stones. It has been reported that during the immobilization period after SCI, there is evidence of “immobilization hypercalciuria” that contributes to nonoxalate calcium stone formation. 11 Typically, calcium phosphate stones predominate in this period. It should be noted, however, that no patient with SCI in our series was treated within the first year postinjury and, in fact, the shortest interval from injury to PCNL was 4 years, with an average of 21 years. This predominance greatly differs from our control group, in which only 16.4% had calcium phosphate stones.
Other studies 12,13 have reported, similar to the findings in our control group, that calcium oxalate calculi are the most common stone composition in the overall population. Parks and colleagues 13 have studied the stone composition of 1201 patients who have been followed for kidney stones. Calcium oxalate was the most common composition. They did note, however, that there has been increasing incidence of calcium phosphate stones during the last three decades. This fact may contribute to the high incidence of calcium phosphate stones in the current series but cannot explain the unusually high preponderance.
Serum studies and urine collection from our cohort provides us with new insights about stone pathogenesis in this patient population. For the 24-hour urine analyses, we have included only patients with metabolic (noninfectious) stones. Including urine data from patients with infection stones would have potentially skewed our results with regard to urinary pH. Because many MS patients have recurrent infections and are often treated with multiple courses of antibiotics, it was necessary to rule out any preexisting colonization with urea-splitting bacteria. To prove the absence of current urinary infection, we have evaluated 24-hour urine collection with regard to ammonium, which is invariably in high levels when infection with a urea-splitting organism is present.
The most striking difference between the groups is the significant difference in urinary pH. Patients with MS anomalies had exceedingly high urinary pH, and this was identified in all subjects within this cohort. This may account for the high incidence of calcium phosphate stones observed in these patients. One possible explanation for the high urinary pH is the presence of resorptive bone disease that is commonly seen in immobile patients. This finding is known to be associated with high urinary pH and active stone formation. 14,15 Despite the overt hypercalciuria, elevated urinary oxalate, and high supersaturation for calcium oxalate identified in patients with MS anomalies, calcium phosphate rather than calcium oxalate stones develop in most patients in this cohort. This is perhaps driven by the exceedingly high urinary pH in these patients (Table 3).
Our study may be limited by several factors. Many MS patients have indwelling catheters or use intermittent self-catheterization techniques. Therefore, their ability to collect 24-hour urine samples may have been different from the patients in the control group. Namely, it would be easier to obtain a complete collection and accurately determine 24-hour urine volume with a catheter. This may account for the higher volumes noted in the MS cohort. Our study group does consist of patients with a variety of conditions and diseases that affect the MS system. While the various diseases may have differential severity and lead to varying degrees of disability, all patients in our MS cohort were bedbound and needed assistance with all activities of daily living.
Recently, we have reported 16,17 on variability in stone composition reporting by commercial laboratories. Specifically, there has been discordance with infection-related calculi, with a 24% disagreement rate between different commercial laboratories. We have chosen to have any amount of struvite inside stone lead to its assignment as an infection-related calculi to decrease the possibility of classifying an infection stone as a metabolic stone. The commercial laboratory that was used in our study uses Fourier transform infrared microspectroscopy, which is considered the best commonly available method for accurately assessing crystalline composition of calculi. 18 Although there are some limitations in using a commercial laboratory for stone composition analysis, the significant difference in stone composition between the MS group and the control group likely cannot be attributed to a laboratory error alone.
Conclusions
Patients with MS anomalies have been traditionally thought to form stones secondary to infected urine with urea-splitting bacteria. Because of significant advancements in the urologic care of these patients, there have been reports of a decreasing rate of urinary infections. Most patients with MS anomalies will harbor metabolically derived stones rather than calculi secondary to infection. We have found a high incidence of calcium phosphate stones in this patient population. This may be attributed to their high urinary pH. Identifying metabolic risk factors for upper tract calculi formation and focusing on prevention may maximize the efficacy and minimize morbidity for patients with MS anomalies.
Footnotes
Disclosure Statement
Dr Lingeman has a financial interest in Beck Analytical Services. For the other authors, no competing financial interests exist.