
Abstract
Background and Purpose:
The da Vinci® surgical system requires the use of electrosurgical instruments. The re-use of such instruments creates the potential for stray electrical currents from capacitive coupling and/or insulation failure. We used objective measures to report the prevalence and magnitude of such stray currents.
Materials and Methods:
Thirty-seven robotic instruments were tested using an electrosurgical unit (ESU) at pure coagulation and cut waveforms at four different settings. Conductive gel-coated instruments were tested at 40W, 80W, and maximum ESU output (coagulation 120W, cut 300W). The magnitude of stray currents was measured by an electrosurgical analyzer.
Results:
At coagulation waveform in open air, 86% of instruments leaked a mean of 0.4W. In the presence of gel-coated instruments, stray currents were detected in all instruments with means (and standard deviation) of 3.4W (±2), 4.1W (±2.3), and 4.1W (±2.3) at 40W, 80W, and 120W, respectively. At cut waveform in open air, none of the instruments leaked current, while gel-coated instruments leaked a mean of 2.2W (±1.3), 2.2W (±1.9) and 3.2W (±1.9) at 40W, 80W, and 300W, respectively.
Conclusions:
All tested instruments in our study demonstrated energy leakage. Stray currents were higher during coagulation (high voltage) waveforms, and the magnitude was not always proportionate to the ESU settings. Stray currents have the potential to cause electrical burns. We support the programmed end of life of da Vinci instruments on the basis of safety. Consideration should be given to alternate energy sources or the adoption of active electrode monitoring technology to all monopolar instruments.
Introduction
An electrosurgical unit (ESU) can be set to deliver power waveforms in watts (W) (power=voltage×current) and the energy delivered is expressed in joules where 1 joule=1W×1 second. ESUs can deliver a continuous waveform with a low peak to peak voltage to cut and an intermittent, modulated (damped) waveform to coagulate. Power density (PD) is power delivered in watts divided by the surface area of the active electrode-tissue interface (PD=W/cm2).
As with any medical device that involves energy delivery, ESUs have the potential to cause patient complications, with a reported injury rate from unintended monopolar ESU at 1 to 2 episodes per 1000 procedures. 5 During laparoscopic surgery, thermal injuries are likely under-reported, because they are frequently unrecognized at the time of the procedure and only manifest later in the form of catastrophic and potentially lethal complications. 6 Under these circumstances, the associated significant morbidity and mortality may lead to medico-legal consequences. 7 –11
Previous work has identified at least four possible scenarios in which electrosurgical injury (ESI) can occur including: (1) inadvertent touching of nontargeted tissue; (2) inadvertent direct coupling to another instrument; (3) capacitive coupling; and (4) insulation failure of the instrument. Insulation failure has been demonstrated to occur in up to 19% of standard laparoscopic instruments 12 ; however, little information exists to ascertain whether this problem occurs in robotic laparoscopic instruments that require use of monopolar electrosurgery and a finite reuse of electrosurgical instruments, both of which provide opportunities for stray electrical currents from capacitive coupling and/or insulation failure.
In this study, we report the prevalence and magnitude of such stray currents measured in da Vinci® (Intuitive Surgical, Sunnyvale, CA) instruments that had reached the end of their duty cycle.
Materials and Methods
All da Vinci robotic laparoscopic instruments that reached the end of their service cycle at our institution during the study period were collected (January 2009–October 2010). Before any testing, instruments were visually inspected for macroscopic insulation defects. The instruments were then tested in open air with a Force 2 (Valleylab, Boulder, Colorado) electrosurgical generator at pure coagulation and cut waveforms in open circuit at four different settings. To simulate the wet intra-abdominal environment, the instrument was then thinly coated with conductive gel (Sigma gel, Parker, Fairfield, NJ) throughout the length of the instrument with the exception of a 1-cm gap adjacent to the instrument tip to avoid current flow from the tip of the instrument and the arm interface box. It was then sequentially tested at 40W, 80W, and maximum ESU output (coag 120W, cut 300W). The magnitude of stray currents was measured by an electrosurgical analyzer (454A Dynatec Nevada).
Statistical analysis was performed using Graph Pad Prism 4 software (GraphPad Software Inc, San Diego, CA). Data were analyzed using one-way analysis of variance with the Bonferroni multiple comparison test.
Results
During the study period (January to October 2010), 37 da Vinci robotic instruments were tested including 9 monopolar scissors (MCS), 1 Maryland bipolar forceps (MBF), 1 monopolar hook (MH), 6 plasma kinetic dissecting forceps (PKDF), eight ProGrasp forceps (PF), and 12 large needle drivers (LND). In this experiment, all available instruments were tested, although some are not designed to deliver energy. On visual inspection, none of the instrument insulation covers demonstrated evidence of cracks or loss of insulator integrity.
Testing using the coagulation waveform (Table 1) in open air showed that 70% of instruments leaked a mean of 0.38W. The maximum leakage (0.7W) was encountered in the ProGrasp forceps. In the presence of gel-coated instruments, stray currents in the form of electrical arcing (Fig. 1) were detected in 81% of the instruments at 40W. The mean energy detected was 3.4W; the minimum energy was 1.5W in a PF, and the maximum 7.7W occurred in a PKDF at 80W. Stray currents were detected in 100% of the instruments, and the mean leaked current was 4.1W. Using full coagulation power (120W), the mean leak was 4.1W. The minimum leakage of 1.9W was found in a MCS and maximum of 10.5W in a PKDF. When comparing the intensity of the leaked energy between the dry state and the wet tests, there was a statistically significant difference (P=0.001). This difference was not significant when comparing between the 40W, 80W and maximum coagulation.
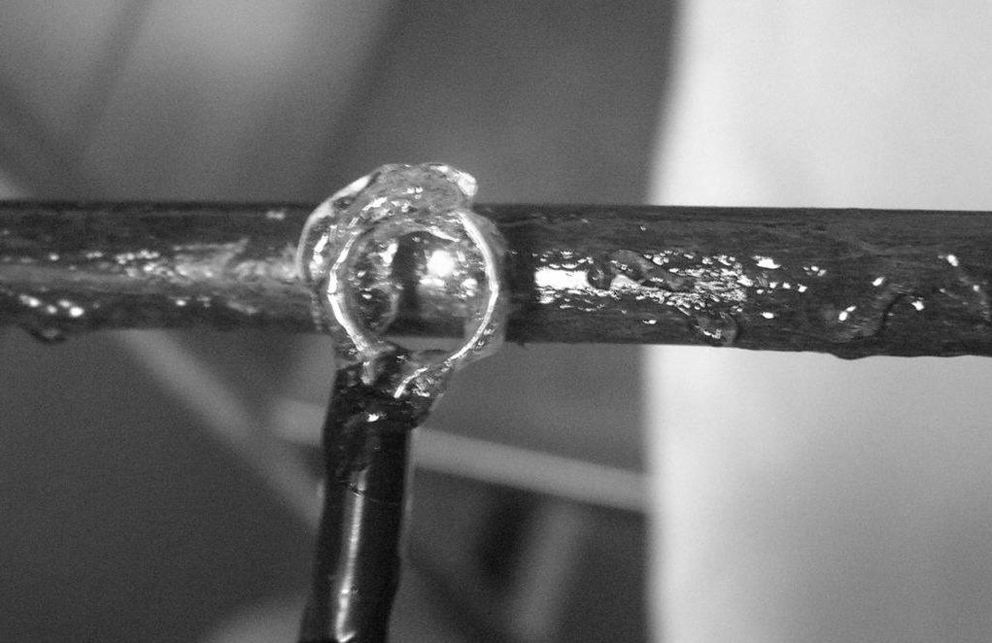
Stray current with electric arcing.
SD=standard deviation; CI=confidence interval.
At cut waveform (Table 2) in open air, none of the instruments leaked current. When coated with gel, arcing occurred at 40W, the mean leaked energy was 2.2W, with the minimum recorded energy of 0.6W in a MH and maximum of 4.3W in a LND. At 80W, the mean energy leak was 2.2W, with the minimum of 0.8 W in a MH and maximum of 8.2 W in a PKDF. When using the maximum output (300W), the mean leaked energy was 3.2W—a minimum of 1.6W, a maximum of 8.2W—again in the MH and PKDF instruments, respectively. There was a statistically significant difference in the energy leaked when comparing the dry test vs the wet tests (P=0.001), but not between the different current settings in the wet group.
SD=standard deviation; CI=confidence interval.
When comparing the coagulation and cut waveform groups, we found no significant difference at 40W. A significantly higher energy leak, however, was found in 80W coagulation vs dry, 40W and 80W cut (P=0.001). This difference persisted when comparing the maximum coagulation vs the dry, 40W and 80W cut (P=0.001). No difference was found in either group when comparing against maximum cut.
Compared by instrument group, the highest mean leakage was in the PKDF (mean 3.6W, one >8W), followed by LND (2.8W), PF (2.4W), MBF (2.4W, single instrument), MCS (1.5W), and MH (1.1W, single instrument).
Discussion
Electrosurgical devices were pioneered by Cushing during the 1920s. Since then, the technology has evolved and become the most commonly used surgical energy device worldwide. 13 Monopolar electrosurgery during endoscopic surgery, including laparoscopic procedures, is associated with unique inherent risks and complications from inadvertent direct and/or capacitative coupling or insulation failure of the instruments.
A capacitor is defined as two conductors separated by an insulator. 14 Because of the high frequency, radiofrequency (RF) currents necessary for electrosurgery, the active electrode (scissors, forceps, hook, etc.) broadcasts energy outside intact insulation, just like a radio transmitter. Any nearby conductor (tissue, metal trocar cannula, telescope, suction-irrigation cannula) may behave as an antenna and pick up broadcasted stray energy.
During laparoscopic surgery, multiple instruments are inserted through abdominal wall ports. When monopolar current is conducted through one of these instruments, capacitively coupled currents are invariably generated to all nearby conductors and, in particular, to patient tissue and organs. Capacitance then allows currents to pass to nontargeted tissue through intact insulation. Capacitors and their associated capacitative coupled stray current pathways are always present during endoscopic surgery. 14 –18 As a rule, these stray currents are dissipated safely back to the ESU through the patient's abdominal wall when metal cannulae are used as ports, but may cause visceral burns in the presence of plastic or hybrid cannulae. 14 When stray currents flow through a small tissue area, the current density can become extremely high and severe burns may result. It has been estimated that power densities of 7.5W/cm2 have the potential to burn. 14 These capacitance currents can be demonstrated by various techniques and can even be visualized in a darkened environment as a bluish line along the interface of the insulated active electrode and nearby conductors. This visible effect is referred to as a corona discharge.
Within a short period (<10 seconds), sufficient heat from capacitance may build up from the corona discharge at the interface of the active electrode and nearby conductor to burn the insulation of the electrode, resulting in direct contact (arcing, sparking, shorting) of the electrode to the adjacent conductor. Each spark reaches temperatures of 700°C to 1000°C, and sparks are delivered at 30,000 per second in the coagulation mode. Under sparking conditions, thermal injury to tissue is instantaneous, inevitable, and severe. This is especially true in hollow organs, such as bowel, where a single spark can destroy the mucosa, which may lead to delayed perforation 3 to 15 days postoperatively.
Our experimental data show that 100% of the reusable robotic laparoscopic instruments used with the da Vinci platform leak electric energy at the end of their life cycle. Previous studies have reported prevalence of insulation defects in laparoscopic instruments at a lower rate of 19% to 39%. 12,18 These series, however, did not test robotic instruments. Espada and associates 19 reported on 81 robotic and 299 laparoscopic instruments that were visually and electrically tested. Insulation failures were detected in 72.8% and 35.1% of robotic and laparoscopic instruments, respectively. The same group also reported two complications potentially associated with stray current in robotic instruments. 20
Our series is novel in that it presents not only a qualitative test of stray current, but also an attempt to quantitate the amount of energy leaked. The threshold for tissue burn injury from ESI has been reported at 7.5W/cm, 2 and a full thickness transmural burn to bowel occurs at approximately 8W. 14
The higher stray currents measured in our in vitro experimental model are likely accounted for by microscopic defects in the instrument's insulation. This is supported by previous publications in which the majority of defects were invisible to the naked eye. 18 With a sensitivity of only 10%, visually screening instruments to predict insulation failure has a limited role. This finding mandates other forms of testing, because these smaller defects are actually the most hazardous; the energy leaking because of its higher current density may cause sparks of up to 1000°C and fires in the presence of flammable gases. 13
Insulation failure most likely occurs intraoperatively, during instrument handling and reprocessing, 21 and/or repetitive and prolonged use of coagulation current. 22 Other risk factors for insulation damage include the use of 5-mm instruments through 10-mm ports and the reuse of disposable instruments. 23 Because our testing involved only full life cycle robotic instruments, we cannot identify at which point the insulation damage may have occurred. Fortunately, the finding of stray current from the used instruments at our institution has not translated into any recognized complications. There are several possible explanations for this, including the insulation may have failed only at testing and not during active life use, the insulation failed during active use but because of safety measures, no complications occurred, and finally, because of the low amount of leaked energy (highest mean 4.1W), there was a subclinical burn injury only. It is unlikely that the instruments had de novo insulation defects, although only similar testing of randomly selected newly minted instruments would exclude this possibility.
Nonetheless, we believe that these findings are clinically relevant. The fact that these instruments were at the end of their life cycle and leaked energy supports the concept of disposal of the instruments at this point to avoid unsafe ESU use, as per the manufacturer's recommendation. Secondly, surgeons must be aware that ESI can occur with robotic instruments and vigilance for intraoperative and postoperative complications is paramount. Although large series evaluating outcomes after robot-assisted laparoscopic surgery have demonstrated extremely low rates of ESI, we propose that such injuries are likely to be both under-recognized and under-reported. Review of the United States Food and Drug Administration Manufacturer and User Facility Device Experience and Medical Product Safety Network databases revealed 24 such cases. 24 ESI does not universally result in perforation and may account to some extent for more commonly seen complications such as ileus after robot-assisted surgery.
Although static testing may be useful in detecting faulty instruments between use cycles, damage can always occur after sterilization or during active use. The extrapolation of our data in the context of active use instruments advocates for the adoption of other safety features, such as the use of alternate energy sources (bipolar RF, ultrasonic, lasers, etc.) or application of active electrode monitoring system, which prevents capacitive coupling and dynamically monitors current flowing through the circuit ; it automatically deactivates the ESU when an insulation failure occurs or excessive capacitive coupling occurs.
A limitation of this current study is the relatively small number of instruments and instrument types tested in an in vitro setting. We were limited by the availability of instruments. We have included all robotic instruments in our analysis, despite the fact that some of the instruments (PF and LND) are not routinely used to deliver energy during surgery. A comparative group of new instruments is lacking, however. We propose that leakage from such instruments remains clinically relevant, given the recognized potential for capacitive coupling. A future phase of testing is planned to include newly minted robotic instruments and at various life points in an effort to document the chronology of damage and to further our understanding of which procedures and instruments increase insulation damage and may need premature replacement independent of their recommended number of uses.
Conclusions
The finding of stray current in robotic laparoscopic instruments at the end of their life cycle appears universal. In some cases, these currents exceed the energy threshold needed to cause thermal damage. Stray currents were higher during coagulation waveforms, and the magnitude was not always proportionally related to ESU settings. Such stray currents can cause electrical burns to patients and/or operating room personnel. Static testing of each instrument should be performed before patient use, and the use of alternate energy sources or active electrode monitoring devices is recommended to prevent patient injury in the event of insulation failure. Further research is needed to determine possible risk factors and time points for insulation damage.
Footnotes
Disclosure Statement
No competing financial interests exist.