
Abstract
Background and Purpose:
Percutaneous nephrolithotripsy (PCNL) is the treatment of choice for patients with large renal stones. The StoneBreaker™ (SB) is a novel handheld pneumatic lithotriptor, powered by a compressed carbon dioxide cartridge. The purpose of this study was to compare the efficiency of the SB to a standard pneumatic lithotriptor, the Swiss LithoClast® (LC).
Patients and Methods:
From January 2008 to December 2009, patients undergoing PCNL were randomized to either the SB or the Swiss LC. Primary outcomes included time to fragment the stone, retrieve the fragments, and remove debris using ultrasonic lithotripsy. Secondary end points were stone-free rate, lithotriptor setup time, ease of use, operator fatigue, endoscopic visualization, damage to mucosa, and device-related complications.
Results:
Of the initial 115 patients recruited, 77 were enrolled and 38 were excluded. The SB had significantly faster stone fragmentation time, total lithotripsy time, and setup time than the Swiss LC (P≤0.05). A significant difference was also noted in the ease of use and operator fatigue in favor of the SB. There were no device-related complications.
Conclusion:
The SB pneumatic lithotriptor is easier to set up and use, and it provides faster stone fragmentation than the Swiss LC.
Introduction
The Swiss LithoClast® (LC) (Electro Medical Systems [EMS], Switzerland), was the first pneumatic lithotriptor and is still used in many institutions. It is powered by compressed medical air, which necessitates attachment to a compressed air source and is activated by a foot switch. 2,3
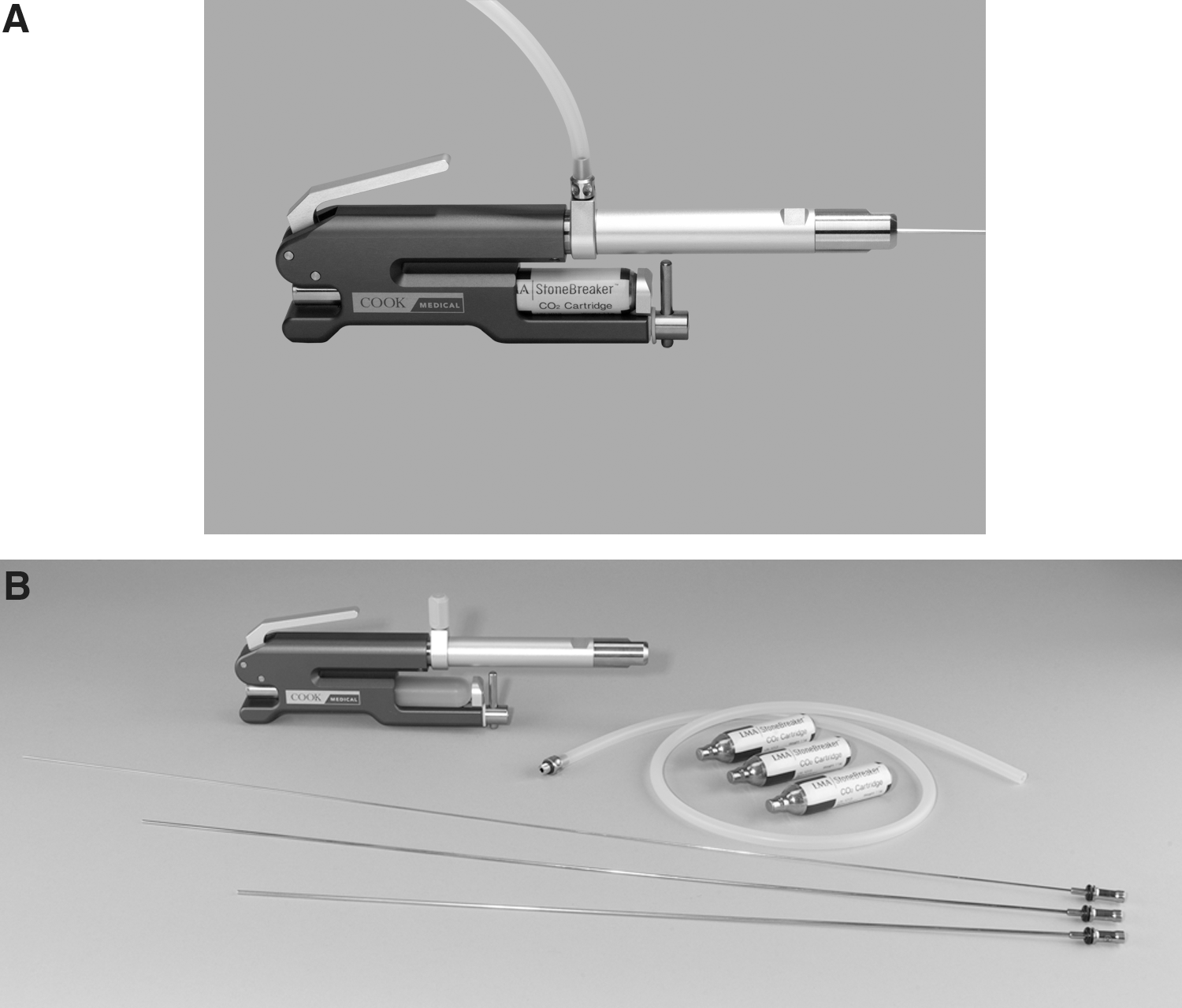
The StoneBreaker™ (SB) (Laryngeal Mask Airway [LMA] Company, Switzerland; distributed by Cook Medical, Bloomington, IN), is a novel, cordless, handheld pneumatic lithotriptor (Fig. 1). This device is powered by a self-contained compressed carbon dioxide cartridge, similar to those used in air/pellet guns. The device is also activated by a hand switch rather than a foot switch, which further eliminates cords in the operating theater. The SB delivers 31 bar of pressure to the stone via the treatment probe, compared with 3 bar by current generation pneumatic lithotriptors. 1,4,5
Previous studies that evaluated the SB and the LC have deemed these devices as highly effective and safe to use for intracorporeal lithotripsy. We took the next step to prospectively randomize and compare the efficacy of the SB with the current pneumatic lithotriptor, the LC, during PCNL at three Canadian centers.
Patients and Methods
Ethics approvals were obtained by the clinical research ethics boards at each of the participating Canadian centers (Vancouver General Hospital, St. Michael's Hospital in Toronto, and Kingston General Hospital). Patients were recruited to the study from the clinical population who presented for stone management at these centers.
Complete inclusion and exclusion criteria are shown in Table 1. All patients who undergo PCNL have a noncontrast CT scan or nephrostography and plain radiography of the kidneys, ureters, and bladder (KUB) before the procedure. Patients with stone sizes of more than 100 mm2 (10 mm×10 mm) on CT KUB were included in the study. A randomization schedule was performed in blocks of 20 to either the SB group or the LC group (at a ratio of 1:1), at the participating centers, using randomization envelopes. Consent was obtained from patients who agreed to participate in the study, according to the particular institution guidelines. Once consent was obtained, medical history, patient characteristics, stone sizes, and stone location were recorded. All patients were treated with preoperative antibiotics, and all procedures were performed in our usual fashion under general anesthesia.
Tracts were dilated to 30F using a balloon dilation method. Patients were blinded and randomized at the time of surgery. If stone fragments were too large to fit in the sheath, then the lithotriptor was reintroduced. The surgeon was timed from the moment the device was first fired against the stone until the surgeon stated the stones had been fragmented to pieces small enough to be removed. If the pneumatic lithotriptor needed to be reintroduced, this was also recorded along with the time for which it was used. Timing of how long the lithotriptor was in the nephroscope was measured as was the time needed to retrieve fragments. Once the surgeon believed all graspable fragments were removed, an ultrasonic lithotriptor (Olympus LUS-2) was inserted to suction small fragments or dust that would be difficult to remove with graspers. This time was also recorded. Total stone fragmentation time was recorded as the total time to fragment the stone, pluck the fragments, and remove debris using ultrasonic (US) lithotripsy. Finally, flexible nephroscopy and concurrent fluoroscopy was performed to ensure there were no residual fragments, and a nephrostomy or nephroureterostomy tube was placed for between 1 and 7 days.
The following was also recorded: Operator fatigue (the level of exhaustion of the surgeons during the procedure, recorded on a scale of 1 to 10, with 10 being none), ease of use (the level of usability of the device, on a scale of 1 to 10, with 10 being simple), endoscopic visualization (the level of visibility on a scale from 1 to 10, with 10 being excellent visualization), damage to the mucosa (the level of damage to the renal epithelium during the procedure on a scale of 1 to 10, with 10 being no damage), as well as any complications that occurred during or immediately postprocedure.
Patients were assessed with a noncontrast CT scan within 1 week after PCNL. Stone free was status defined as no visible fragments of any size on CT KUB.
A parametric t test was performed for independent measures (nonpaired). In addition, a nonparametric test was performed, Mann-Whitney. Statistical significance was set at P≤0.05.
Results
From January 2008 to December 2009, patients were randomized to either the SB or the LC. Of the initial 115 patients recruited, 77 were enrolled (46 were randomized to SB and 31 to the LC arm), and 38 were excluded because of stones being too small (ie, removed intact) or too soft, thus necessitating US lithotripsy and suction removal (16 from the SB arm and 22 from the LC arm). Patients in both arms who were excluded intraoperatively were then treated using the US lithotriptor.
Patient characteristics are outlined in Table 2. The rate of stone fragmentation was significantly faster for the SB 6.46*±4.16 mm2/sec, than the LC 3.59±2.87 mm2/sec (difference of 95%: 2.87 [2.68–3.05]; P<0.0010).
CI=confidence interval; SD=standard deviation; BMI=body mass index.
A subgroup analysis of only calcium oxalate stones was performed to compare fragmentation efficiency of only one stone type and eliminate potential differences between the various stone compositions. There was no difference in stone sizes between the two groups (P=0.1279). In this subgroup analysis, the SB was still significantly faster at stone fragmentation: 6.30*±4.18 mm2/sec compared with 3.87±2.86 mm2/sec for the LC (difference of 95%: 2.43 [0.427–4.43]; P=0.0185).
Total lithotripsy time included the time to fragment the stone with one of the pneumatic lithotripters, time to retrieve fragments, and the time to remove debris with US lithotripsy. Faster total lithotripsy time was observed for the SB 671.3*±489.6 seconds, compared with the LC 1012.5±629.1 seconds (difference of 95%: 341.2 [72.26–610.1]; P=0.0139; Fig. 2).

Total lithotripsy time (seconds).
The setup time for the device was significantly shorter for the SB 67.6*±51.4 seconds, than the LC 101.9±39.6 seconds (difference of 95%: 34.3 [12.712–55.956]; P=0.0023).
A significant difference was also noted in favor of the SB, on a scale of 1 to 10, in the ease of use (10=easy; 9.33*±1.43 for the SB, vs 7.35±3.25 for the LC; difference of 95%: 1.98 [1.23–2.74]; P<0.0010), and operator fatigue (10=no fatigue; 9.51*±1.46 for the SB, vs 7.52±2.87 for the LC; difference of 95%: 1.99 [1.38–2.61]; P<0.0010). Endoscopic visualization (10=adequate visibility; 9.16±1.59 for the SB, vs 8.39±2.12 for the LC; difference of 95%: 0.77 [0.47–1.07]; P=0.0849) and epithelial damage (10=no damage; 8.75±2.37 for the SB, vs 8.19±2.80 for the LC; difference of 95%: 0.56 [0.25–0.81]; P=0.4601) were not statistically significantly different.
There were no significant differences in stone-free rate or stone composition in either group (Tables 3 and 4). All 77 patients were evaluated with a postoperative CT scan. The percentage of patients who were stone free or had fragments smaller than 4 mm were almost identical in both groups (87% for the SB and 90% for the LC, P=0.1152). There were no device-related complications in either group.
Discussion
PCNL is an established procedure for large renal calculi with success rates that range from 85% to 90%. 6,7 This procedure has evolved since it was first reported 30 years ago, and its safety has been well established. 8 Rigid lithotriptor devices form the mainstay of intracorporeal lithotripsy during PCNL because of their ability to fragment and remove large stones efficiently. The LC was the first lithotripter introduced in the early 1990s and is considered the standard in pneumatic lithotripsy. 2 It is powered by compressed medical air, which necessitates attachment to a compressed air source. The unit also needs a foot switch to activate the device.
The SB is portable and is the only commercially handheld pneumatic lithotriptor available without needing the use of foot pedals or attachment to external compressed air. The SB is relatively lightweight, weighing 515 g (with the probe and the small carbon dioxide cartridge attached), and is significantly more powerful than the original LC, delivering 31 bar of pressure at the tip of its treatment probe compared with 3 bar. 1,4,9 The SB device is powered by a self-contained compressed carbon dioxide cartridge, similar to those used in air/pellet guns. In theory, this simplifies its use in the operating theater because the operator's hand piece is not tethered by a cord to an external generator. The device is also activated by a hand switch rather than a pedal, which eliminates further cords. It is single fire with each release of the hand-activated trigger as opposed to the option for multiple pulses using the pedal activated LC. Because the SB provides much more power with each shock, it is better to position the probe in the middle of the stone where maximal fragmentation can occur before firing it. The SB device releases no thermal energy and therefore presents no risk of thermal injury to surrounding tissue; it has been used safely and effectively across the world. 1,4,5,9
In our study, the SB was statistically significantly faster at fragmenting stones than the LC. In addition, the SB had faster total lithotripsy time—results that were also confirmed when only calcium oxalate stones were analyzed. This brings us to the main limitation we found in this study—not only for the SB but for all pneumatic-only lithotriptors—that soft, crumbly stones are not easily managed by this type of pneumatic modality. Using ballistic lithotriptors for such soft stones often results in making many small fragments that are time consuming or difficult to remove with graspers. This often results in small fragments travelling throughout the collecting system and leads to failure of the operation, because many of these fragments will not pass, particularly if there is migration into a lower pole calix.
The authors of this study routinely used a modality that also included suction lithotripsy, such as US ithotripsy. Using only pneumatic energy and graspers to remove fragments proved very difficult in these soft stones without the use of US lithotripsy. In cases with these soft stones, the majority of which were struvite, the ideal method is to use US lithotripsy to grind and concurrently remove stone fragments. Conversely, when stones are particularly hard, such as calcium oxalate monohydrate or calcium phosphate, US lithotripsy can be tedious and slow. In these cases, we have found it more efficient to fracture the stone into large fragments and remove them with graspers. These harder stones are more amenable to breaking into larger pieces with pneumatic lithotripsy than are soft stones.
We recommend that soft, crumbly stones are better treated using a device that possesses suction capability because of the small fragments generated during fragmentation that are difficult to remove with graspers. The pneumatic lithotriptors used in this study are better for fragmenting hard stones.
We suspect that the differences observed in this study for the performance and stone clearance between the SB and LC were likely because of the advantages of the SB, particularly the increased power generated by the SB, which made it more efficient at stone fragmentation. Furthermore, because of the additional advantages—lightweight, cordless, ergonomic handle, and hand switch, as well as self-contained CO2 cartridge—the SB caused less operator fatigue than the LC to the surgeon. Although a subjective observation, surgeons in this study noted less fatigue, which may have been because the SB was faster and more efficient at fragmenting stones. A longer time would be needed using the LC, which could result in more fatigue.
One limitation to our study worth consideration was that the LC is representative of older technology; however, the device was the only true comparator and was also available at the participating centers. In addition, cases in which the surgeons experienced device malfunction with the LC were excluded from the study, and data were not recorded; therefore, we have fewer cases in the LC arm. For these cases, pneumatic lithotripsy was abandoned, and US lithotripsy only was used instead to fragment and remove the stone.
Another limitation of our study was that we only looked at two different types of pneumatic-energy–based lithotriptors, despite the availability of a multitude of combination lithotriptors. Two other novel dual-probe intracorporeal lithotriptors, Cyberwand (Olympus-ACMI) 10 and LC Ultra/Select (EMS/Boston Scientific) 11 have been shown to be effective. The LC Ultra/Select combines a US lithotriptor with an inner pneumatic probe. 11 One clinical study compared the efficacy of stone fragmentation of the LC Ultra with the US lithotriptor (LUS-1) in 30 patients. 12 The authors reported no difference in stone-free rate or fragmentation efficiency between the two different types of lithotriptors. They also confirmed the findings in our study that the combined pneumatic/US lithotriptor was better suited for harder stones and that softer stones were better managed with US lithotripsy only.
A North-American multi-institutional prospective randomized study is currently under way to evaluate the Cyberwand, LC Ultra, and the SB (combined with the Olympus LUS-2 to provide suction of small fragments), which represents a follow-up to our current study. This study is necessary to help determine if there are any advantages to one lithotriptor in particular.
Conclusion
The SB is an effective tool for intracorporeal lithotripsy during PCNL, particularly for hard stones. This prospective randomized multicenter trial showed that the SB is easier to set up and use and provides significantly faster stone fragmentation than the LC. We recommend routine use of the SB for all PCNL cases that involve hard stones.
Footnotes
Disclosure Statement
No competing financial interests exist. The main author, Ben H. Chew, has a nonfinancial relationship with Cook Medical, Inc. (distributor for the LMA StoneBreaker device), as their respective consultant; however, he did not receive any consultant or other fees related to the work presented in this article. The main author, and anybody connected to him in any way, did not receive any personal benefits for doing this research. LMA Switzerland funded administrative costs for the study and provided equipment and disposables in kind for the study. None of the authors directly received any funds from the study.