
Abstract
Background and Purpose:
Postoperative recovery of intestinal function, ability to ambulate, and effective pain management are main features to establish an effective fast-track surgery model. We investigated pain scores, ambulation rate, and recovery of intestinal function in a cohort of patients who were undergoing laparoscopic radical prostatectomy (LRP).
Patients and Methods:
Fifty patients who underwent LRP in our institution were randomized to receive either conventional or fast-track postoperative care. Postoperative intestinal function was quantified by clinical signs of intestinal motility. Ambulation data were collected by means of step-count devices. Pain scores were measured by a visual analog scale. Overall satisfaction and additional measures to describe patient satisfaction with the clinical course were used as quality-of-life variables.
Results:
Fast-track patients had significantly earlier propulsive intestinal motility without increased intestinal complications. Enforced mobilization led to a significantly shorter period to first deflation/defecation. Despite significantly increased ambulation rates in the fast-track group, these patients reported significantly less pain sentience during a significantly shorter hospital stay. Overall satisfaction was significantly higher in the fast-track cohort during the hospital stay.
Conclusion:
With the implementation of fast-track concepts for LRP, patients can be discharged to home earlier with fewer complications, lower pain scores, and an overall higher satisfaction with life.
Introduction
Fast-track surgical concepts are a relatively new approach deviating from traditional surgical treatment plans that typically incorporate postoperative food restriction, prolonged volume therapy, placement of nasogastral tubes and intra-abdominal drains, and postoperative immobilization. 2,3 In a number of randomized trials from different surgical fields, a considerable reduction of postoperative complications and faster convalescence has been demonstrated, 2,4 –6 The main foundations of fast-track surgical management are modification of pain management, early mobilization, and perioperative stimulation of intestinal function with the goal to shorten the convalescence phase. 7,8 Previously, a fast-track concept for LRP has been proposed by our group incorporating modifications of anesthesiologic and surgical perioperative procedures, postoperative opioid-free pain management, and a special nutrition and mobilization pathway. 6
The aim of the current study was to focus on pain scores, mobilization, and recovery of intestinal function in a cohort of patients who were undergoing LRP and who were randomized to conventional perioperative management or our fast-track pathway. Furthermore, patient self-assessment with regard to qualitative attributes of the hospital stay was evaluated.
Patients and Methods
Fifty patients were randomized to receive either conventional perioperative management or a perioperative multimodal fast-track concept with changes in preoperative, intraoperative, and postoperative care as described previously. 6 Briefly, fast-track patients received an accelerated oral nutrition and mobilization management with an adapted opoid-free analgetic treatment that incorporated high-dose COX-2 inhibitors postoperatively. Furthermore, fast-track patients were subject to highly encouraged postoperative mobilization and early discharge from the hospital. Exclusion criteria for study participation were reduced renal function (creatinine levels preoperatively >1.6 mg/dL); American Society of anesthesiologists IV; use of cytotoxic drugs, immunosuppressants, or anticonvulsives; severe general or central nervous system diseases; and refusal to participate in the study. Patients in the fast-track cohort were discharged home on postoperative day 3 with an indwelling transurethral catheter. Patients in the conventional treatment group were briefed on a hospital stay of 6 to 8 days with removal of the transurethral catheter before discharge to home. All patients provided informed consent when indicated by the Institutional Review Board.
Measures
Mobilization
Patients in both groups were motivated to ambulate as soon and as much as possible postoperatively. Beyond that, patients in the fast-track group were asked to walk with any member of the medical, nursing, and physiotherapeutic staff whenever communicating with the staff, regardless of the communicative subject. Furthermore, patients in the fast-track group received a leaflet with ambulation rates to be achieved during the postoperative course. Ambulation of the two cohorts was measured by means of step-count devices attached to the patients' slippers.
Intestinal function
Postoperative recovery of intestinal function was assessed in both groups as the time of first deflation or defecation.
Pain
Patients were asked by a trained interviewer to give daily reports concerning their degree of resting pain and pain during ambulation. Patients indicated their levels of visual analog scale ranging from 0 (no pain) to 10 (excruciating pain). The average postsurgery retest stabilities were r=0.42 for resting pain and r=0.40 for pain during mobilization (all P<0.001).
Quality-of-life measures
Satisfaction with life
From day 1 preoperatively to day 3 postoperatively, patients in both groups were asked by a trained interviewer to rate their present-day general satisfaction with life (one item) on a 10-point Likert-type scale ranging from 0 (very bad) to 10 (excellent). Mean intermeasurement correlations ranged from r=0.51 to r=0.70 (all P<0.001), indicating a satisfactory retest reliability of the measure.
Additional measures included satisfaction with the length of the hospital stay (one item, interview; “too short,” “exactly right,” “too long”) and a one-item general satisfaction with the perioperative course (interview), rated as either “worse than expected,” “as expected,” or “better than expected.”
Statistics
Analyses of interval data were conducted using the one-way and repeated-measures analyses of variance (ANOVA). Ordinal and categorical data were analyzed using chi-square tests.
Missing: Six patients were not interviewed on the day of surgery. Item nonresponses within assessments led to further loss of data. Patients who failed to return full study materials were more likely to be in the conventional treatment group (chi-square (1)=4.35, P<0.05). Patients who were interviewed on the day of surgery did not differ systematically from patients who could not be interviewed on the variables under study.
We used regression-based imputation methods to account for the missing-data in interval-scaled self-reports and mobilization data as previously described. 9,10 Imputation and data analyses were conducted using SPSS 16.0 for Windows (SPSS, Chicago, IL).
Results
Patient characteristics
Table 1 demonstrates demographic and perioperative patient characteristics. Patients under the fast-track concept had a significantly shorter hospital stay (3.6 vs 6.7 days, P<0.001), while there were no differences for the remaining variables presented in this table.
Mann-Whitney U test for continuous and chi-square test for categorical data.
One patient exhibited 1500mL blood loss during the surgery. Deletion of this outlier results in a mean blood loss of 214.0mL (SD 147.3 mL) for fast-track patients.
ASA= American Society of Anesthesiologiests; PSA = prostatespecific antigen; SD= standard deviation.
Ambulation
Because of the fast-track pathway with discharge to home in the morning of postoperative day 3, ambulation data for this cohort were limited to 2 postoperative days. One multivariate outlier from the fast-track group with extremely high z-scores for ambulation at 1 and 2 days postsurgery was excluded from the analysis (Mahalonobis distance 17.69, P<0.001). This patient's step-count device indicated 9000 (first postoperative day; z=4.14) and 16,700 (second postoperative day; z=3.76) steps. For the remaining cases, results from a repeated measures ANOVA demonstrated a steeper increase in mobilization postoperatively for fast-track patients (TIME x treatment: Wilks' Lambda=0.674; F (2, 46)=11.15, P<0.001, η2=.33; Fig. 1). Furthermore, the average postoperative level of mobilization was higher for fast-track patients compared with patients in the conventional postoperative treatment group (treatment: F (1,47)=17.99, P<0.001, η2=.28; Fig. 1).
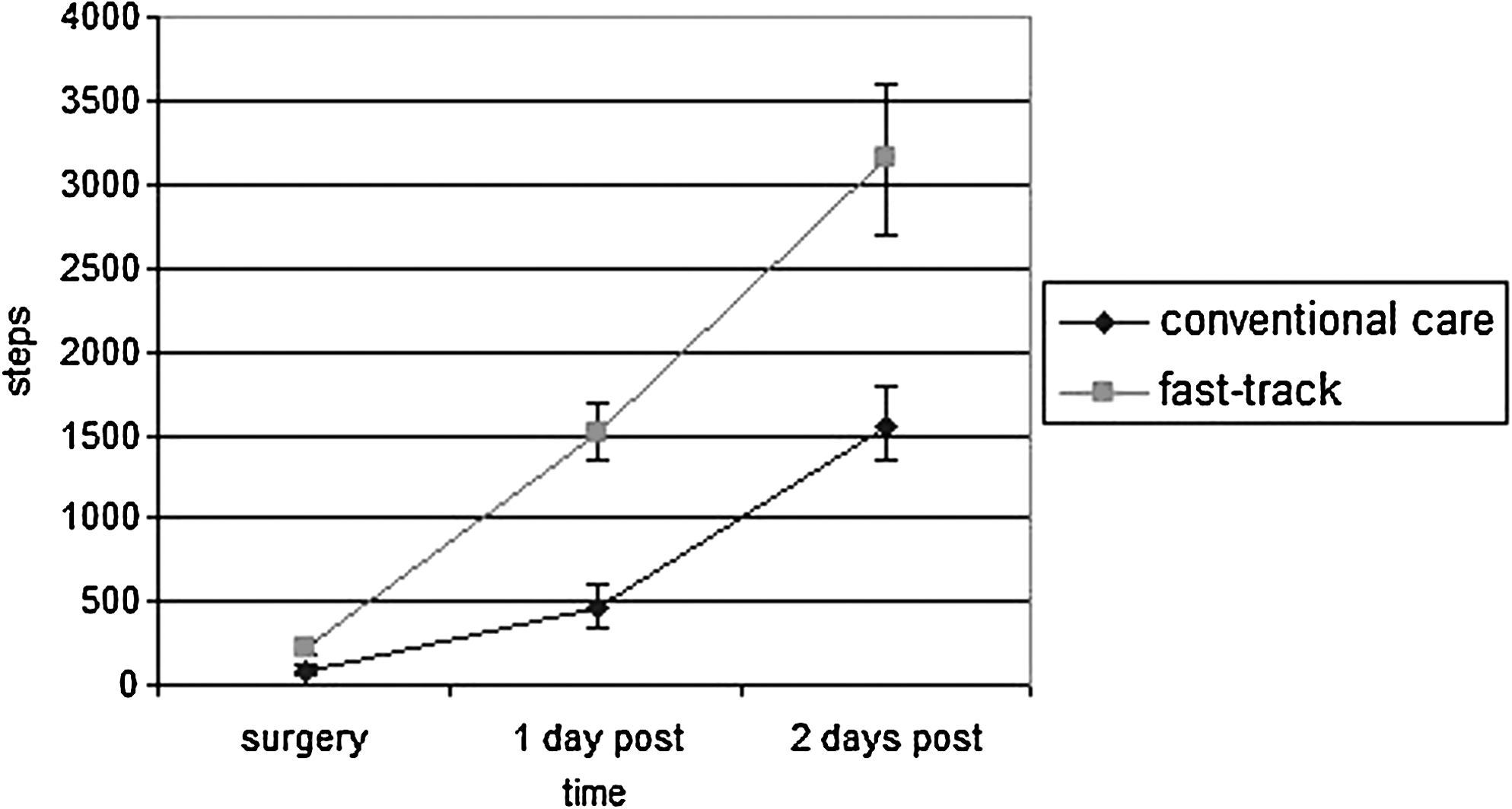
Mean (+standard error) numbers of steps from day of surgery until 2 days postsurgery for conventional-care patients (n=25) and fast-track patients (n=25, 1 outlier removed).
Intestinal function
Time to first deflation or defecation was significantly shorter in the fast-track cohort (0.76±0.66 days vs 1.16±0.62 days, P=0.034). Moreover, we demonstrated that patients with high ambulation frequencies (more than 130 steps on the day of surgery) had a significantly shorter time interval to first deflation/defecation than patients with lower ambulation frequency (0.62 days vs 1.12 days, P=0.014).
Pain
Presurgical pain levels of both treatment groups did not differ significantly (Fig. 2, fast track: 0.04±0.20, traditional group: 0.00±0.00; P=0.32). Postsurgery, patients from the fast-track cohort showed steeper decreases in resting pain (TIME x treatment: Wilks' Lambda=.832; F (3, 46)=3.09, P<0.05, η2=.17; Fig. 2). Moreover, fast-track patients reported lower overall levels of pain during mobilization/ambulation postoperatively (treatment: F (1, 48)=12.35, P=0.001, η2=.21; Fig. 2). There were no significant Time x treatment effects for pain during mobilization.

Mean (+standard error [SE]) resting pain (left) and mean (+SE) mobilization pain (right) from presurgery until 3 days postsurgery for conventional-care patients (n=25) and fast-track patients (n – 25).
Opioids (piritramid) were intended as a rescue medication for the fast-track cohort. Only one patient, however, requested additional pain medication (7.5 mg piritramid once subcutaneously) on postoperative day 1. In the conventional treatment cohort, patient-controlled analgesia (PCA) pumps with piritramid were offered routinely. Of these patients, 19/25 (76%) requested this option. All patients stopped using the PCA pump by postoperative day 2. On average, the PCA pump was used seven times on the day of surgery and four times on postoperative day 1.
Length of hospital stay
On average, patients in the conventional treatment group were discharged to home on postoperative day 6.72 (standard deviation [SD]=0.94), while patients receiving the fast-track concept left the hospital significantly earlier with a mean hospital stay of 3.60 days (SD=1.22; F (1, 48)=102.40, P<.001, η2=.68).
Satisfaction with life
Concerning daily interview assessments of satisfaction with life, patients from the fast-track group indicated steeper increases in satisfaction postoperatively (TIME x treatment: Wilks' Lambda=.742; F (3, 46)=5.33, P<0.01, η2=.26) and higher average postsurgery levels of satisfaction (treatment: F (1,48)=4.44, P<0.05, η2=.09). Preoperatively, there were no significant differences between the study cohorts documented on this measure.
Additional measures
There were no significant differences with regard to satisfaction with the length of the hospital stay and general satisfaction with the perioperative course between the two groups (Table 2).
Discussion
Surgical procedures represent a disturbance of the physical integrity and inevitably cause a postoperative stress response of variable degree depending on a number of factors, such as type of the surgical procedure, intraoperative complications, blood loss, length of procedure, and others. Because of the increasing number of surgical procedures that are performed in Germany each year and concurrent limited financial resources, one major challenge of the past years was to increase surgical quality performance by using centers of excellence, standardization of surgical training, and establishment of surgical pathways for standard procedures.
Previous studies have shown the beneficial effects of fast-track concepts, such as enhancing recovery and reducing morbidity and mortality, for major surgical procedures. For open radical prostatectomy, clinical pathways describe a length of hospital stay ranging from 1 to 6 days. 5,11 Because of fundamental distinctions of the health systems and postsurgical care, data on length of hospital stay from the United States are to be contemplated separately. To date, data on fast track LRP from Europe are sparse.
We demonstrated that the implementation of a fast-track concept reduced the hospital stay from on average 7.0 to 3.6 days with a concomitant significant decrease of the overall complication rate. 6 Beyond the favorable effects with regard to the complication rate, patients in the fast-track group reported an overall higher satisfaction with quality of life compared with the conventional pathway cohort.
Postoperative gastrointestinal dysfunction, such as PONV or intestinal paralysis is known to potentially cause intensified therapeutic effort and prolongation of the hospital stay. To overcome intestinal complications, we adapted a nutrition concept described previously. 6 In our study, the new nutritional concept caused few intestinal complications with no statistically significant differences between the study cohorts. Comparable data of other investigators on this subject are not available in the current literature. Our findings, however, concur with observations from Raue and associates 4 who undertook a similar study on patients undergoing laparoscopic sigmoidectomy. They did not find any statistically significant differences between the fast-track cohort and the cohort receiving conventional perioperative care with respect to the recovery of gastrointestinal function, although patients in the fast-tract cohort returned to a regular diet earlier.
Other investigators have demonstrated that besides anesthesiologic PONV prophylaxis, one of the most important factors affecting the incidence of PONV is preoperative hydration and high oral intake of carbohydrates until 2 hours preoperatively. 12,13 These findings lead to recent modifications of anesthesiologic guidelines that advocate preoperative intake of carbohydrates up to 2 hours before induction of anesthesia. 14 Bisgaard and colleagues, 15 however, did not find a reduction of PONV in patients receiving a carbohydrate-rich beverage before laparoscopic cholecystectomy. 15 An additional positive effect of preoperative carbohydrate intake, which has not been specifically investigated in the current study, is the reduction of postoperative insulin resistance and subjective postoperative well-being, contributing to a reduced complication rate. 16
In our study, ambulation measured in steps per day was significantly higher in the fast-track cohort. These findings demonstrate that the implementation of a fast-track concept significantly improved postoperative patient activity. Patients who had higher ambulation rates had significantly higher chances to report bowel motility on the day of surgery, and fast-track patients had an overall shorter time to first deflation or defecation compared with the cohort receiving standard care. Although the beneficial effects of fast-track concepts on patient recovery and return of bowel function have been shown in the past, to our knowledge we are the first to present the association of ambulation frequency and return of bowel motility. It is likely that our favorable results with respect to bowel function recovery are not caused by increased ambulation alone. Rather, the concomitant nutritional and analgetic regimes have cumulative significant beneficial effects on intestinal function. Other known midcomplications of prolonged immobilization, such as pneumonia, thrombembolic events, prolonged fatigue, or loss of muscle mass, 17 have not been investigated because of the low duration of mean hospital stay.
Patient cooperation and motivation can be achieved only if, preoperatively, sufficient information, particularly about the significance of postoperative ambulation, is provided. We created elaborate information leaflets with detailed description of postoperative requests for ambulation, which has been shown to increase the ambulation frequency significantly. Beyond that, on every personal contact, the entire medical, nursing, and physiotherapeutic staff was required to encourage the patient to ambulate. As discussed earlier, this simple means led to a significantly faster return of bowel function, potentially affecting patient overall satisfaction with the hospital stay.
Intensified early mobilization can only to be achieved with sufficient pain management. Opioids, the substances most commonly used for pain management after major abdominal procedures, constitute a highly potent class of analgetics. They might, however, compromise the postoperative intestinal motility when given in potent doses. 18 Moreover, higher doses of opioids are known to cause nausea and vomiting. That again might interfere with the need for early nutrition, along with an effective fast-track concept. Because LRP in general is a minimally invasive approach with documented fewer pain scores reported by the patients, 14 we abstained from opioids in the fast track whenever possible and chose the long-lasting Cox-2 inhibitor etoricoxib as an analgetic only. Interestingly, patients undergoing the fast-track regimen indicated lower pain scores even without the use of opioids under concomitant higher ambulation scores.
Overall, with the targeted adaptation of the mutually dependent perioperative main features—ie, pain management, mobilization, and nutrition—patients in the fast-track cohort reported significantly lower pain scores, a higher ambulation rate, and an earlier return of bowel function postoperatively. The length of hospital stay was abbreviated by approximately 50%. The implementation of our perioperative rehabilitation concept resulted in significantly higher rates of overall satisfaction with life. Satisfaction with the length of hospital stay and the overall approval with the clinical order of events did not differ significantly between the study cohorts. We demonstrated to gain high acceptance from the patients receiving the straight ahead fast-track concept, however.
Conclusion
With implementation of fast-track concepts for LRP, patients can be discharged to home earlier with fewer complications and an overall higher satisfaction with life. Future studies with larger patient cohorts are warranted to validate our initial findings.
Footnotes
Disclosure Statement
No competing financial interests exist.