
Abstract
Background and Purpose:
Typical lengths of stay after open cystectomy are 5 to 7 days, without dramatic differences reported for laparoscopic or robot-assisted cystectomy. We developed a clinical pathway for early discharge after robot-assisted cystectomy, attempting to take advantage of potentially decreased morbidity with this minimally invasive procedure and analyzed our initial outcomes.
Patients and Methods:
The initial 30 consecutive patients undergoing robot-assisted cystectomy who were treated on a clinical pathway developed at our institution were reviewed. This included an extraction incision of ≤3 inches also used for urinary diversion, no intensive care unit stay, no nasogastric tube, and avoidance of intravenous narcotics. Ambulation is begun on postoperative day (POD) zero, with clear liquids uniformly on POD 1, then regular diet on passing flatus. Patients are discharged when tolerating diet, with a target of POD 3.
Results:
Mean age was 67 years (45–87 y), and mean operative time was 411 minutes. All ambulated by POD 1. Only 4 of 30 needed any intravenous narcotics. Twenty-one patients were discharged on POD 3 and 8 on POD 4 for an overall mean of 3.3 days, including 2 who were discharged on POD 2 and 1 on POD 7. One was seen in the emergency department on POD 6 for emesis, and one was readmitted on POD 7 for candidal infection. No others returned to the clinic or hospital within a week after discharge (POD 10).
Conclusion:
Our clinical pathway after robot-assisted cystectomy allows shorter hospital stays than typical and is, to our knowledge, the shortest reported after cystectomy by any technique. Only two unplanned visits occurred during the first 10 days. Further experience will be necessary to confirm the initial success.
Introduction
If this procedure offers the typical benefits of minimally invasive surgery and is found to have advantages over open cystectomy, it might be expected that the postoperative hospitalization time could be reduced, as has been seen with many laparoscopic and robot-assisted surgeries. As yet, postoperative hospital length of stay for both laparoscopic and robot-assisted cystectomy in most series has not been dramatically improved over that reported by many centers of excellence with open cystectomy. 6
We hypothesized after our early experience with robot-assisted cystectomy that the use of intravenous narcotics could be avoided and early ambulation could be encouraged because of less pain. We further hypothesized that less bowel exposure and retraction or packing with the robotic approach might additionally reduce ileus and allow earlier diet. Because ileus is a major cause of prolonged hospitalization after cystectomy, occurring in up to 32% of patients with many contributing factors, 2,3,7,8 we believed that the robotic approach may allow shorter hospitalization if these hypotheses were true.
Given diverse reports in the literature of success with clinical pathways for other surgical procedures, 4,9 –12 we developed the first reported clinical pathway for robot-assisted cystectomy that was designed to take advantage of the potential reduction in morbidity of this minimally invasive procedure. We present our initial experience uniformly applying this pathway with the intention of evaluating whether the potential benefits of the procedure can be successfully translated into a reduced hospital stay.
Patients and Methods
Beginning in April 2008, we instituted a clinical pathway for postoperative care of all patients without exception who were undergoing robot-assisted laparoscopic cystectomy by a single surgeon (RA). Patients who were undergoing surgery in the subsequent 2 years through March 2010 were included in the study. All patients with an indication for cystectomy who presented to the surgeon during this period were treated with robot-assisted surgery, except for one patient who chose open surgery after a discussion of both options, such that the patient population included in the study was an unselected group. Intent-to-treat analysis was used to determine ability to adhere to the pathway and subsequent outcome. The data were collected prospectively and evaluated retrospectively with Institutional Review Board approval.
Preoperatively, a mechanical bowel preparation was taken at home by all patients consisting of 4 L of polyethylene glycol electrolyte solution (GoLYTELY®) and oral antibiotic preparation with neomycin and erythromycin. Two days before surgery, patients were instructed to take only clear liquids with no oral intake after midnight the day before surgery, and patients then presented to the hospital on the morning of surgery. An orogastric tube was placed intraoperatively and removed at the time of extubation.
Elements of the pathway consist of the following (Table 1): After the robot-assisted cystectomy (with extended lymph node dissection in cancer patients) is completed, an incision limited to 2 to 3 inches as measured by the ruler is made for specimen extraction and creation of the urinary diversion (Fig. 1). All bowel anastomoses were performed using a standard side-to-side technique with a GIA 60 and TA 60 metal stapling device (Autosuture, North Haven, CT). A pelvic drain is left in place in the form of a Foley catheter per urethra, which is removed just before discharge or when drainage ceases, if earlier, with no drains exiting from the skin. No drains were left in female cancer patients in whom the urethra was completely excised, with only vaginal gauze packing to collect drainage from the reconstructed vagina. Postoperatively, patients are preferentially admitted to a nursing care unit experienced in caring for robot-assisted surgery patients.
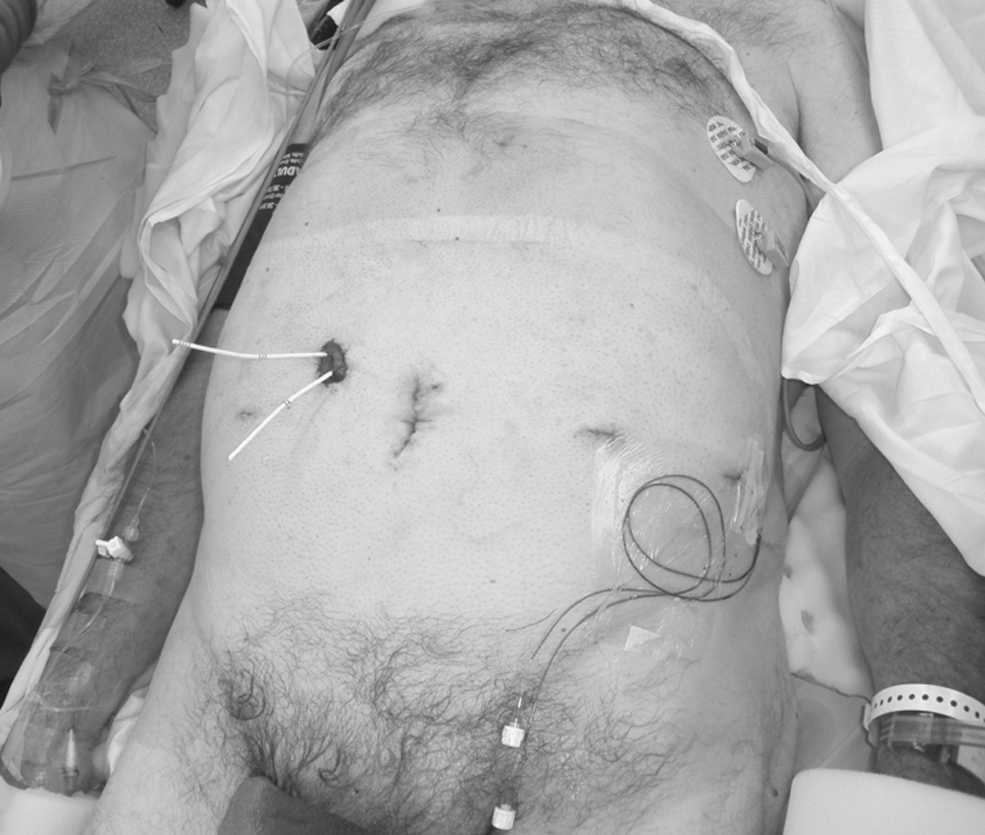
Postoperative appearance of a patient who underwent robot-assisted cystectomy with minimized extraction incision also used for creation of urinary diversion and subcutaneous analgesic catheter tunneled from left port site.
Postoperatively, intravenous narcotics are avoided and are purposely excluded from the postoperative nursing orders. Nurses are instructed to call for such orders if pain is not sufficiently controlled with intravenous ketorolac given every 6 hours and oral narcotics as needed (maximum of two tablets of oxycodone/acetaminophen 5 mg/325 mg every 4 hours). A continuous local anesthetic infusion catheter (ON-Q®, I-Flow, Lake Forest, CA) placed subcutaneously at the extraction site incision intraoperatively delivers 20 mg of bupivicaine hydrochloride per hour for 3 days, after which it is removed before discharge or by the patient at home if discharged earlier (Fig. 1).
All patients are required to ambulate the night of surgery or the following morning with assistance from nursing staff, if needed. Diet is begun on postoperative day (POD) 1 with clear liquids in all patients regardless of abdominal examination or passage of flatus. Regular diet is then begun on POD 2 or 3 based on the physical examination of the abdomen (eg, distention, bowel sounds) and passage of flatus. Diet is delayed if the patient experiences nausea, emesis, or has abnormal abdominal examination findings. Patients are discharged when tolerating a regular diet and passing flatus with a target discharge day of POD 3 with all catheters and drains removed except for ureteral stents left in place until office follow-up at approximately 2 weeks and then 6 weeks after surgery. All 30-day readmissions or unscheduled emergency department (ED) or clinic visits were recorded at these visits even if they occurred at outside facilities. Routine follow-up included 3-month visits followed by imaging for cancer surveillance begun at 6 months postoperatively.
Results
A total of 30 patients underwent robot-assisted cystectomy during the study period with all placed on the clinical pathway and no patients excluded from analysis and no other patients undergoing robot-assisted cystectomy during the study period by the surgeon. Twenty-six were treated for bladder cancer and 4 for complications of previous bladder surgeries or radiation. One bladder cancer patient had remotely undergone external beam radiation for prostate cancer, and two of the four benign cystectomy patients had previously undergone radiation for prostate and cervical cancer. No patient had clinical symptoms of radiation enteritis preoperatively.
While all patients were offered continent or incontinent diversions, only two patients chose continent catheterizable pouch diversions, and none chose neobladders with diversions performed extracorporeally. Twenty-five patients were men and 5 were women. Mean follow-up was 361 days (range 90–611 d). Mean patient age was 67 years (range 45–87 y) with mean body mass index of 28 kg/m2 (range 20–43 kg/m2). Seven patients had received neoadjuvant chemotherapy for bladder cancer, including one who had a biopsy-confirmed nodal metastasis that resolved after chemotherapy.
The mean and median Adult Comorbidity Evaluation-27 scores were 1.5 and 2 of 3, respectively. Twelve (40%) patients had a history of one or more previous abdominal operations ranging from simple hernia repairs to laparotomy for major surgery, including one with aortic aneurysm repair. Pathologic stage in bladder cancer patients included pT0 in five, pTis in one, pT1 in three, pT2 in eight, pT3 in four, and pT4 in five patients, with nine (30%) patients having nodal disease. Positive surgical margin occurred in only two (6.6%) patients, both of whom had T4N2 disease.
Mean operative time from incision to dressing was 411 minutes (range 308–496 min) in part because of the typical 1.5 to 2 hours spent on extended lymphadenectomy alone. 13 Mean estimated blood loss was 170 mL (range 50–550 mL) with only one blood transfusion (3%). All extraction incisions were successfully limited to a maximum of 3 inches even when used for pouch creation and in obese patients. Despite the ability to perform diversions through these small incisions, only two patients experienced ureteroileal anastomotic strictures (7%), both of the left ureter, during the follow-up period (mean 361 d). The average length of the extraction incision as measured by ruler was 2.1 inches (range 2–3 in) where the continuous local anesthetic infusion catheter was placed in all patients. A closed-suction drain was avoided in all but three patients, including one of the patients with a continent diversion, one patient with radiation-induced pelvic tissue necrosis to help close the space, and one woman with vaginal invasion by tumor where the vagina was by necessity surgically obliterated.
Postoperatively, all patients ambulated and began a liquid diet by POD 1. Nine of 30 patients started a regular diet on POD 2, 12 started on POD 3, and 9 patients did not start a regular diet until POD 4 because of abdominal distention and absence of flatus until then. Symptoms of ileus developed in one patient thereafter such that diet was discontinued until day 6 with discharge on day 7.
Pain was managed successfully with only intravenous ketorolac and oral narcotics in all but four (87%) patients. Four (13%) patients received some dose of intravenous narcotics in the postoperative period. One patient was chronically dependent on narcotics, including methadone and oxycodone, before surgery and was unable to be managed without intravenous narcotics immediately after surgery. A second patient was unable to receive ketorolac because of a history of chronic renal insufficiency and therefore needed intravenous narcotics until his pain could be controlled with oral analgesia alone. The remaining two were the first patients placed on the clinical pathway at our institution and before the house staff and nurses were acclimated to it, such that intravenous narcotics were allowed before the other analgesics were exhausted; after these, an explicit order regarding avoidance of intravenous narcotics unless necessary was added.
Twenty-one of 30 (70%) patients were discharged by POD 3, including 2 patients who were discharged on POD 2. Eight patients were discharged on POD 4 and one on POD 7. One patient without family or others to provide supervision was discharged to a nursing facility on POD 4, but all other patients were discharged to their homes and not nursing or other assisted care facilities or nearby hotels. Mean length of stay overall was 3.3 days (median 3 d).
The patient with chronic narcotic dependence presented to the ED on POD 6 for an episode of emesis that resolved with a single dose of promethazine and returned home with no further events. Another patient was readmitted on POD 7 with candidal urinary tract infection and wound infection. No other patient was readmitted, visited the ED, or returned for an unscheduled clinic visit within the first 8 days after discharge (through POD 10). Therefore, a 10-day postoperative hospitalization in all 30 patients would only have prevented one readmission and one ED visit.
Thereafter, there were six patients who had unscheduled visits within 30 days of surgery but after POD 10. These included a patient who was transferred from a distant ED on POD 11 for concern over fat protruding alongside the stoma that was found to be insignificant with discharge the following day, one readmission for pelvic abscess on POD 13, one readmission for vertebral compression fracture on POD 14, one readmission on POD 17 for urinary tract infection and deep venous thrombosis, and one admission at an outside facility for hernia repair 4 weeks postoperatively. One patient with early Alzheimer's disease was readmitted for 3 days according to Medicare rules to allow for coverage of a nursing facility stay once it became apparent that her husband's health issues limited his ability to continue to care for her at home.
Discussion
Clinical pathways after major surgery have demonstrated benefit in reducing lengths of stay without unacceptable readmission rates. 10,14 –16 Chang and colleagues 17 found that institution of a clinical pathway after open radical cystectomy reduced median hospital stay to 7 days from a previously reported 10- to 17-day length of stay. Pruthi and coworkers 18 achieved a mean length of stay of 5 days with 79% discharged by POD 5 in their most recent 100 patients on a fast-track program after cystectomy at an institution performing both open and robot-assisted surgery.
Because we hypothesized that robot-assisted surgery would have less morbidity than open surgery, we instituted a clinical pathway for robot-assisted surgery attempting to take advantage of this potential benefit and thereby reduce postoperative stays. While we cannot be certain that the ability to reduce hospital stay was because of reduced morbidity with the robotic procedure and not simply from use of a clinical pathway, we believe that the combination of the two was responsible for our shorter length of stay than previously reported with either open or minimally invasive cystectomy whether with or without a pathway. 17 –23
With a widespread focus on the current state of health care and its financial constraints, reducing costs has become an important goal. Operating room time and length of hospital stay are two major contributors to the overall costs of surgical care. Minimally invasive surgical techniques can reduce hospitalization time after major urologic surgery and may reduce complications, but operative times are initially longer as surgeons become facile with the techniques. Our operative times were long but comparable with the equivalent open surgery at our institution primarily because of the extent of lymphadenectomy we perform that extends above the aortic bifurcation and yields a mean of approximately 40 nodes in both types of surgery. 13 Such an extensive dissection adds at least an hour compared with less-extensive lymphadenectomies typically performed, if not even longer as reported by others also performing such dissections robotically. 24,25
Besides our expectation that operative times will be reduced with further experience, unless the purported reduction in morbidity with robot-assisted cystectomy can be confirmed by allowing shorter hospitalization, the additional cost will be difficult to justify. Therefore, institutions already performing robot-assisted cystectomy or exploring the possibility should consider use of a clinical pathway to reduce length of stay, thereby capitalizing on the potentially reduced morbidity of robot-assisted vs open surgery.
Our clinical pathway after robot-assisted cystectomy aimed at early return of bowel function to allow early resumption of diet and discharge. This strategy depends on the expectation of reduced pain by making only small incisions, allowing for reduced narcotic requirements and early ambulation. It is also possible that a closed abdomen with bowel manipulation only during the urinary diversion is also beneficial in early return of bowel function, but this as well as the theory that the closed abdomen leads to less fluid shifts and bowel edema has not been proven. Also, even further advantage may have been gained had we used a less rigorous preoperative bowel preparation. While the need for a bowel preparation has been questioned in the colorectal surgery literature and the need for antibiotic preparation in cystectomy challenged, 18,26 we continue to use a possibly excessive regimen more for the purposes of decompressing the bowel to allow surgical working space in the robotic environment and continue to use antibiotic preparation because of the inherently higher risk of inadvertent bowel injury with minimally invasive surgery over open surgery.
While ileus was not avoided in all patients, the 1 of 30 (3%) patients in our series in whom an ileus developed was well below the expected rate observed in open surgical series. 17 One criticism of using such small incisions for urinary diversion is the potential for an increase in ureteroileal anastomotic strictures from overmobilization of the ureters to reach the skin level or from tension on the anastomosis. We take care to avoid these pitfalls and therefore had only two such strictures occur (7%), which is within the expected rate with open surgery of 4% to 8%. 27
None of the elements of our clinical pathway alone is novel, but the combination takes advantage of an expectation of reduced morbidity with minimally invasive surgery. Early removal of nasogastric tubes after open surgery has not been found to be associated with an increase in complications, 28 and we eliminated its use as practiced by many open surgeons as well. Early resumption of an oral diet has demonstrated benefit, 29 and we found that early institution of a diet in our patients did not lead to an increase in gastrointestinal complications or associated readmissions. We found that limited use of intravenous narcotic after robot-assisted cystectomy is feasible in most patients and were able to limit narcotics by using local anesthesia, with proven pain-control benefit in other surgical procedures and potential cost-savings, 30 –34 and ketorolac, which has been shown to speed bowel myoelectric activity. 35 While our retrospective study was limited in this regard, given that we did not document patient perceptions of pain control, our judicious use of intravenous narcotics in some patients when pain control was otherwise inadequate reflects that we did not intentionally subject our patients to an unreasonable pain to force narcotic avoidance, which would have been against our institutional mandate of pain control and unacceptable to nursing staff.
We also believe, though, that setting patient expectations preoperatively is important, as is minimizing the psychological impact of major surgery on patients by eliminating an intensive care unit stay, a nasogastric tube, and closed-suction drain used by many surgeons. Whether these measures reduce patient anxiety and contribute to earlier convalescence cannot be proven or disproven from our data, but our strategy in general is to promote “normalcy” as much as medically possible and to be sensitive to medical devices and procedures (such as drain removal) that are taken for granted by us as surgeons but not so by patients who are unfamiliar with such medical routines.
Our report of a limited patient series represents the initial experience at our institution using our pathway but by a surgeon having performed robot-assisted cystectomy previously at another institution where hospitalization was typically 4 to 5 days without a pathway. If the goal had been to demonstrate a benefit of robotic over open cystectomy, the pathway would have to be applied to all cystectomy patients and the ability to adhere to it analyzed thereafter. Because our goal was not to support one approach over another, we simply aimed to determine whether we could capitalize on our perception of how well our patients seemed to recover after robot-assisted surgery by accelerating their postoperative care plan. Regardless of whether robot-assisted cystectomy truly reduces patient morbidity compared with open surgery, we encourage those already performing the robotic procedure to consider our findings and apply a clinical pathway.
Some may be uncomfortable discharging patients who have undergone cystectomy after only 3 days, but we would encourage such surgeons to consider whether their patients commonly experience complications between day 3 and 7 that would necessitate continued hospitalization. In our experience, complications during the first week are unusual and do not justify keeping all patients beyond day 3 or 4. Based on the 30 patients who were treated on our pathway so far, all patients would have needed 10 days of hospitalization to avoid one readmission and one brief visit to the ED. Clearly, cystectomy remains a complex procedure with potential complications unrelated to the early postoperative recovery as seen among the six (20%) patients in our series who needed readmission within 30 days. These readmissions were not thought to be a result of early discharge, and our rate of 30-day readmission was not unreasonable, given the more than 20% rate observed at high-volume cystectomy centers according to national Medicare data. 36
Significant limitations to the study of clinical pathways such as ours include the inherent difficulty of creating a control group because of the bias involved in deciding on discharge readiness of an individual patient. The most effective way to eliminate such bias would be to blind the discharge decision-maker to the postoperative care of the patient, but this would be difficult and potentially a disservice to the patient. Also, our clinical pathway has only been applied to a small number of patients, given the relative novelty of robot-assisted cystectomy, with single-surgeon experiences greater than this number still relatively rare. We therefore would caution against overly optimistic conclusions because we do not anticipate uniform success with this approach and expect that some patients will still experience ileus or other complications necessitating lengthy admissions or, more likely, later readmission given the inherent complexity of cystectomy. Nevertheless, we expect that the mean hospitalization with this pathway will remain favorable, given even our limited experience with it to date.
Conclusion
Our clinical pathway after robot-assisted cystectomy facilitates shorter hospital stays than are typical after open cystectomy and is, to our knowledge, the shortest hospitalization time reported after cystectomy by any technique. Further experience will be necessary to confirm the initial success.
Footnotes
Acknowledgment
The authors wish to acknowledge Laura Kirk-Fetsko, RN, for data collection and management.
Disclosure Statement
No competing financial interests exist.