
Abstract
Purpose:
To determine the effectiveness of postgraduate training for learning extraperitoneal robot-assisted radical prostatectomy (EP-RARP) and to identify any unmet training needs.
Materials and Methods:
The training resources used were live surgery observations, digital video disc instruction, postgraduate courses, and literature review. Modifications to the transperitoneal (TP) setup in equipment, patient positioning, port placement, and access technique were identified. A surgeon who had previous experience with 898 TP robot-assisted radical prostatectomies (TP-RARPs) performed EP-RARP in 30 patients. We evaluated setup results, emphasizing access-related difficulties, and compared the EP cohort with a nonrandomized, concurrent TP cohort of 62 patients for short-term outcomes.
Results:
The median setup time for EP was 26 minutes (range 15–65 min) for EP compared with 14 to 17 minutes for the comparable TP setup and dropping the bladder. During EP setup and dissection, peritoneal entry occurred in 37%, incorrect port spacing in 10%, epigastric vessel injury in 10%, and other minor pitfalls in 10%. No significant differences were found between EP and TP in postsetup operative times, hospital stay, complications, surgical margin status with organ-confined disease, or lymph node dissection yield. EP had significantly higher estimated blood loss (300 vs 200 mL, P=0.001) and more symptomatic lymphoceles when extended pelvic lymph node dissection was performed (3/16 vs 0/47, P=0.001).
Conclusions:
Using postgraduate education resources, an experienced TP-RARP surgeon successfully transitioned to EP-RARP, achieving the major objectives of safety and equivalent outcomes. We identified several minor nuances in the setup that need further refinement in future education models.
Introduction
Ideally, surgeons receive all necessary training during their residency or fellowship programs and are prepared to handle the spectrum of potential challenges. One method of incorporating a complex new technology or technique into a surgical practice, therefore, is to recruit a new surgeon whose formal training included the desired topic. In some circumstances, however, recruiting a new surgeon is not feasible or is considered to be unnecessary. An alternative strategy is to identify effective training resources for currently employed surgeons; that is, to provide them with postgraduate training.
In the postgraduate training model, resources may include video instruction, continuing medical education courses, surgical observation, animal or dry laboratories, surgical simulators, and proctored cases. Although such resources can be effective, there may be limitations in the scope of case complexities presented, and the total time available for training is limited because the trainee likely carries a full-time practice. The precise educational needs of each trainee will be different; for example, training a surgeon who is skilled in open surgery to gain competence in laparoscopic surgery could be a more complex task than training a surgeon who is skilled in laparoscopy to gain competence in robot-assisted surgery.
To implement new techniques for the surgical management of localized prostate cancer, our department used a recruitment model to adopt laparoscopic radical prostatectomy in 2002 (SM) and robot-assisted radical prostatectomy (RARP) in 2006 (JW.D)—both using standard transperitoneal (TP) access. In 2010, however, we added the extraperitoneal (EP) access technique 2 using a postgraduate training model. Therefore, the purposes of this study were to evaluate the effectiveness of our postgraduate training model for EP-RARP and to identify any unmet training needs.
Materials and Methods
Prerequisites and resources
Previous studies suggested that experience in TP access for laparoscopic or robot-assisted prostatectomy is a prerequisite to learning EP access. 3,4 Our assumption was that the TP access was the preferred environment to focus on optimizing cancer control, functional recovery, avoiding complications, and developing effective training methods. 5 We assumed that TP access was the preferred environment for solving intraoperative challenges, such as massive glands (ie, >100 g), median lobes, accessory pudendal arteries, and pubic arch interference. Therefore, the prioritization for learning EP was low, and the total TP-RARP experience was 898 cases between 2004 and 2010 (JWD) before attempting the first EP-RARP. Furthermore, the training and initial series studied has been limited to a single surgeon.
Table 1 outlines the resources used to learn EP-RARP: Case observations (n=4), digital video disc (DVD) instruction (n=2), postgraduate courses (n=3), and published literature with technical descriptions and key diagrams (n=5). We did not use surgical proctoring, animal or dry laboratory dissections, or surgical simulations.
DVD=digital video disc.
Technique
We identified equipment needs specific to EP-RARP (Table 2) compared with a typical TP case card, and specified the key differences in access technique (Table 3). The patient position and padding are the same, but for EP, there is only half of the full Trendelenburg position (full=40 degrees). In theory, the Trendelenburg position is not needed for EP, but without it, the bladder tends to require additional cephalic exposure, and further compromise will occur if any peritoneotomy occurs. If peritonomomy occurs, the use of suction may result in a “wind-sock” effect whereby the differential pressure between the two cavities causes a rebound bulge of the peritoneum into the field. To correct this problem, the surgeon should make the peritoneal hole larger over the iliac vessels so that the pressure can equilibrate faster.
EP=extraperitoneal.
EP=extraperitoneal; TP=transperitoneal; ACIS=anterior superior iliac spine.
The locations of all port placements are described in Table 3 and illustrated in Figure 1. Note that the working robotic ports 1 and 2 are located significantly closer to the pubic arch for EP than for TP access. Because the patient is in half Trendelenburg, however, the pubic arch is at a more open angle, which permits access to the apex of the prostate. The initial balloon dilation of the EP space opens room for the robot medial ports 1 and 2. The lateral ports necessitate additional dissection starting just under the epigastric vessels at their distal ends and aiming laterally just over the spermatic cord.
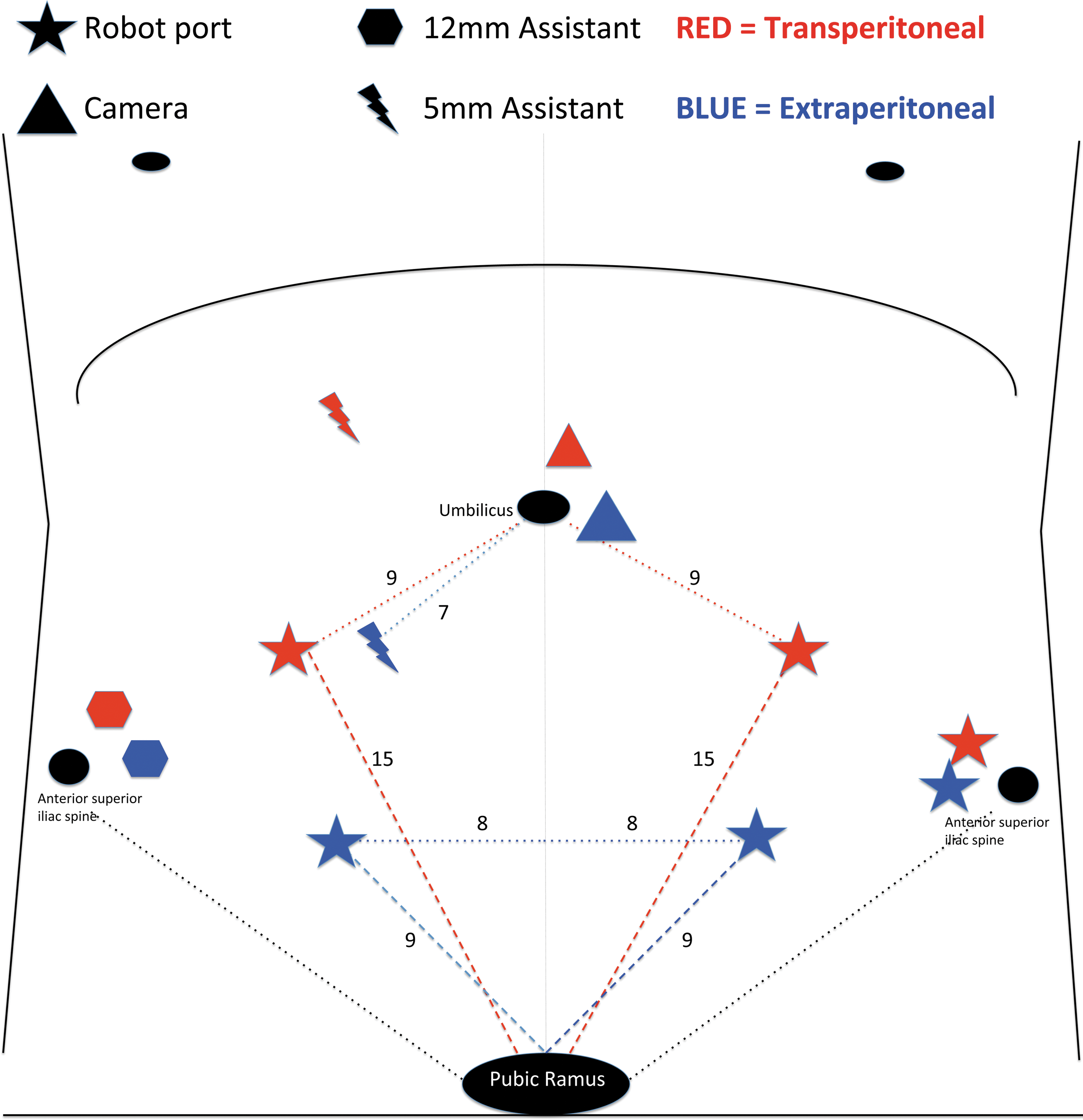
Port placements: Extraperitoneal (blue) vs transperitoneal (red). The extraperitoneal port placement is based on the descriptions of Joseph and associates. 2
By placing a finger over the skin in the area of the planned lateral port placement, the surgeon can feel the camera and determine when the space is large enough for port placement. The camera is moved to the lateral port, and the camera port is removed. The left index finger is placed through the fascial hole to allow blunt dissection of the peritoneum superiorly to place the 5-mm assistant port, which is used primarily for suction. The finger is used as a guide to keep the port placed at an angle that avoids the TP space. Finally, the camera port is replaced, a purse-string suture is tied around the port, and Xeroform™ gauze is wrapped and sutured in place to seal the gas leak. The robot is then docked. All procedures were performed with the da Vinci S model (Intuitive Surgical Inc., Sunnyvale, CA).
Once the EP access and docking are complete, the operation proceeds through the same steps as the TP procedure. In general, the reduced space in the EP procedure is more noticeable to the assistant than to the console surgeon. The pelvic lymph node dissection (PLND) can be performed similar to that of TP, including an extended template. The first step is to identify the ureter and hypogastric artery. To find these landmarks, the surgeon should transect the vas deferens and mobilize it toward the obliterated branch of the hypogastric artery. The spermatic cord is mobilized laterally, and the pocket of peritoneum overlying the iliac vessels is mobilized and retracted superiorly. The lymph node dissection templates for an extended PLND can be applied except at the tissue medial to the hypogastric artery. A 10-mm multi-fire titanium clip applier is used to seal the lymphatics that are cut at the proximal, distal, and lateral borders of the template.
While working on the lymph nodes or anastomosis, the prostate can be placed out of the way in one of the lateral spaces that was bluntly dissected for port placement. If the prostate is too large to fit into the lateral space, it may need to be sutured to the abdominal wall. To exit, we undock but leave the EP space insufflated. The camera is placed through the lateral port and the Endocatch bag string is extracted through the camera port. The camera is then replaced through the midline port and used to guide a Carter-Thomason (Cooper Surgical, Trumbull, CT) closure of the lateral 12-mm port. A drain is then positioned through the left robot port 3. The camera port incision is then extended enough to extract the specimen in its Endocatch bag and repaired with interrupted 0 polydioxanone (Ethicon, Inc, Somerville, NJ) closure of the fascia.
Patient selection
From January 2010 to May 2010, 30 patients with localized prostate cancer were selected for EP-RARP by a single surgeon (JWD). The selection criteria included low- to intermediate-risk disease (no PLND was attempted until case 4), body mass index (BMI) <35 kg/m2 (one patient was 40 and lost weight to 37 preoperatively), and no previous pelvic surgery or laparoscopic herniorrhaphy using mesh. During the same period, the same surgeon (JWD) performed 62 TP-RARPs.
Data collection specific to EP-RARP
We prospectively recorded standard demographic, clinical, pathologic, and short-term results, including complications classified by the Clavien method. 5 For this study, we also recorded the time needed to complete each of 11 distinct steps of the procedure (data from trainees excluded from the analysis), 6 and immediate postprocedure comments by the surgeon about the quality of port placements, avoidance of peritoneotomy and epigastric vessel injury, and time to set up access.
Statistical analysis
We used the Wilcoxon rank-sum test to compare variables measured on a continuous scale and we used the Fisher exact test to compare categorical variables (eg, disease risk, stage, complications, surgical margin status). Differences were considered statistically significant if the two-sided P value was less than 0.05.
Results
Setup
The median setup time for EP-RARP from incision to robot docking was 26 minutes (range 15–65 min), including setup times for the first three procedures of 65, 45, and 28 minutes. This setup time for EP-RARP also accomplishes step 1 of a TP case—dropping the bladder. The equivalent time for TP would be the sum of docking 7 to 10 minutes for incision to docking (consistent and no longer recorded) plus a median of 7 minutes (range 2–97 min) to drop the bladder (formally recorded), for a total median setup time of 14 to 17 minutes.
Pitfalls encountered learning EP access
Peritoneal entry occurred in 11 (37%) of 30 cases. The entries occurred commonly along the medial umbilical ligament or over the iliac vessels. The entries occurred during the initial dissection for port placement or later in the procedure in cases for which PLND was performed. Five of the EP-RARP patients had a history of lower abdominal surgery, and the setups for four (80%) of these cases resulted in peritoneal entry. In 3 (10%) of 30 cases, the port spacing was judged to be in error and caused collisions between ports or between the robotic instruments and the pubic arch. Furthermore, in three (10%) cases, injury occurred to the epigastric vessels during either port placement (n=1) or instrument exchange (n=2). These and other pitfalls encountered while learning EP-RARP are shown in Table 4.
Comparison of EP and TP
The EP and TP patient cohorts had similar BMIs and prostate volumes. The EP-RARP patients were younger, however, and because of selection criteria, had lower-risk disease (Table 5). Despite the longer setup time needed for EP, the total postsetup operative times were not significantly different. The median estimated blood loss was significantly higher for EP than for TP (300 vs 200 mL, P=0.001). No significant differences were found between EP and TP in duration of hospital stay, incidence of complications, incidence of positive surgical margins in patients with organ-confined disease, or PLND yield.
Estimated blood loss=volume in suction canister minus irrigation used in the field.
EP-RARP=extraperitoneal robot-assisted radical prostatectomy; TP-RARP=transperitoneal robot-assisted radical prostatectomy; BMI=body mass index; PLND=pelvic lymph node dissection.
Although the overall incidence of complications was not significantly different between EP and TP, we noted that 3 (19%) of 16 EP-RARP patients who also underwent extended PLND needed lymphocele drainage. Conversely, none of the 47 TP-RARP patients who underwent TP needed lymphocele drainage (P=0.001). There were no instances of other known radical prostatectomy complications, such as urinary leaks, anastomotic strictures, or injuries to ureters, iliac vessels, or the bowel in either cohort.
Discussion
The key finding from our study was that a postgraduate education model can be used by surgeons with substantial TP-RARP experience to gain proficiency in EP-RARP without altering short-term outcomes during the training period. The unmet training needs were minor and included efficiency in dissecting the full EP space and avoiding peritoneotomy, epigastric artery injury, and port spacing errors. We were aware of previous descriptions of bilateral peritoneal fenestration after EP-RARP with lymphadenectomy to reduce the incidence of symptomatic lymphocele; for instance, Stolzenburg and associates 7 reported reducing symptomatic lymphoceles from 14% to 0% with this technique. We attempted to prevent lymphoceles with extensive clipping, as is often performed in open radical prostatectomies. It may be that the extended PLND transects such a large volume of lymphatic channels, however, that clipping cannot fully seal. We have since adopted this technique.
To our knowledge, this is the first study to assess the applicability of a carefully documented postgraduate training model to teach EP-RARP to surgeons with TP-RARP experience and to then self-evaluate this model. Potential limitations of this study include the nonrandomized comparison of EP with TP, the single-surgeon results, and the decision to not use surgical proctors. In particular, the comparison of TP with EP is meant to illustrate the initial feedback one might receive when adding this technique to an established TP practice, and our conclusions should not be considered as definitive. Nevertheless, our documented learning experience might improve future learning curves for EP-RARP, and future DVD and didactic instruction should incorporate tips and tricks to avoid the pitfalls we identified.
We recommend that surgeons learning EP-RARP select patients with BMI <35, no previous abdominal surgery, and low-risk disease (ie, PLND is not needed) for the first 10 to 30 procedures or until they are proficient at setup and avoiding common pitfalls. For two of our early cases, we selected patients who had previously undergone significant abdominal surgery (and thus theoretically might have benefited from the EP approach), including midline incisions extending to the pubis. We found that the midline scarring from the previous surgery prevented full balloon dilation to both sides of the EP space. The remaining contralateral dissection therefore had to be performed by laparoscopic sharp dissection. The resultant anatomy from such a modification will not look familiar to the surgeon unless straightforward cases have been performed first. Since this study, we have solved this problem in similar patients by making a second fascial incision on the contralateral side of the midline from the initial balloon entry. This allows further balloon dilation to the contralateral side and will often break down the midline scarring to complete the space.
Most reports of EP-RARP and EP-laparoscopic radical prostatectomy have focused on the feasibility of the techniques and their possible advantages over TP-RARP, 8 –14 such as avoidance of bowel complications, avoidance of encountering scarring from previous abdominal surgery, protection of the peritoneal compartment from postoperative urine leaks or hemorrhage, and reduced need for the full Trendelenburg position. In contrast, the TP technique provides a larger space, allows for posterior seminal vesicle dissection, facilitates extended PLND, and is preferred for patients who have had laparoscopic herniorrhaphy with mesh. Therefore, the literature does not support one technique as superior in all cases. Rather, as Capello and colleagues 11 concluded, “Surgeons should be familiar with both approaches in order to provide patients with the best care.”
Indeed, despite our extensive experience with TP-RARP, we commonly find patients with potential indications for EP access: Previous abdominal surgery, symptomatic inguinal hernia needing mesh repair, or cardiac disease with drug-eluting stents (in the last scenario, RARP is performed without discontinuing aspirin, and EP access will provide better tamponade than TP if postoperative bleeding occurs). As future robotic instruments become smaller, necessitate fewer access ports, and offer a greater range of motion, the TP access may no longer have a geometric advantage. Barret and coworkers 15 reported their initial experience with single-port access for RARP in the EP space. In the future, we believe EP may become the standard approach for minimally invasive surgery, just as it is for open surgery, for the simple reason that it is better not to open the peritoneum unless you have to.
Conclusions
Using a postgraduate education model, an experienced TP-RARP surgeon successfully learned to perform EP-RARP. The major learning objectives were achieved, and we identified several minor pitfalls that should be addressed in future training programs.
Footnotes
Acknowledgments
Supported in part by the Ken and Ashley Lee Foundation, the Katz Foundation, and the National Institutes of Health through MD Anderson's Cancer Center Support Grant CA016672.
Disclosure Statement
John W. Davis: Scientific Study, Genprobe, Cougar Biotechnology. No competing financial interests exist for any of the other authors.