
Abstract
Purpose:
To analyze the effectiveness of simplified urethropexy in the evolution of urinary incontinence after radical laparoscopic prostatectomy.
Patients and Methods:
Between January 2007 and December 2008, 104 patients were included in a randomized trial to assess the effectiveness of simplified urethropexy. The simplified urethropexy technique was performed on conclusion of a urethrovesical anastomosis with running suture and, before cutting the suture material, a suture was applied using the same material with a needle through the pubic tubercle, tightening it and securing it with a Hem-o-lok. Fifty-one patients qualified for the trial in the simplified urethropexy group (group 1) and another 51 in the control group without urethropexy (group 2). Incontinence was defined as the lack of the need for protection for normal life, and the degree of continence was compared at 3, 6, and 12 months after surgery.
Results:
Surgery lasted 141 minutes in group 1 and 139 in group 2 (NS). There were no secondary complications such as urine retention, osteitis pubis, or bladder perforation. After 3 months, 47.1% of patients in each group declared continence (NS). After 6 months, 72.6% of patients in group 1 and 66.7% in group 2 (P<0.05) declared continence. After 12 months, 92.2% of patients in group 1 and 84.3% in group 2 declared continence.
Conclusions:
In our experience, simplified urethropexy is a simple, nontime-consuming technique that shows a slight clinical improvement in continence within 6 and 12 months, without reaching significant differences with the Fisher Test. It would be necessary to perform a trial with a greater number of patients to confirm these data.
Introduction
In laparoscopic surgery, the performance of these techniques may be complex because of the greater technical difficulty of completing the sutures. We present our experience in a simplified urethral suspension technique in radical laparoscopic prostatectomy.
Patients and Methods
Between January 2007 and December 2008, we performed a trial on the use of simplified urethropexy in the recovery of continence after radical prostatectomy. The exclusion criterion was having had previous prostate surgery (transurethral resection of the prostate or adenomectomy), previous radiotherapy, as well as the application of extraperitoneal technique because of previous abdominal surgery.
This trial was approved by our Institutional Review Board and included a total of 104 patients. The patients were informed of the technical modification and were randomized consecutively into the simplified urethropexy group (52 patients) and the control group without urethropexy (another 52 patients). One patient from the urethropexy group was excluded from the trial because he was unavailable for follow-up and another patient from the control group was excluded because of development of urethritis that had necessitated subsequent catheterization and an urethral stricture that was pending a surgical solution. Thus, 102 patients were eligible for the trial, 51 in each group.
Continence was defined as the lack of need for protection in normal life. The McNemar test was used for dichotomous variables (continence yes or no) and the Fisher test to compare the degree of continence between both groups at 3, 6, and 12 months after surgery.
Regarding surgical technique, all patients underwent laparoscopic transperitoneal radical prostatectomy (LRP) by the same surgeon (CNM) who had a wide experience in LRP (more than 300 cases at the beginning of this study). In all the cases, the puboprostatic ligaments were sectioned, because this is the technique that is normally used at our center. Continuous cervicourethral anastomosis was performed, beginning in the 5 o'clock position. In the urethropexy group, after completing the suture, the same needle was used to apply one stitch to the pubic periosteum, and after tightening it, it was secured with a Hem-o-lok (Fig. 1). The tension applied to this traction must be enough to get an elevation of the anastomosis without being necessary to contact the pubis.

When finishing anastomosis, the same needle was used to apply one stitch to the pubic periosteum and after tightening it, it was secured with a Hem-o-lok.
Results
Both groups were compatible in relation to age, body mass index, prostate volume, prostate-specific antigen level, and preoperative Gleason score.
Neurovascular preservation was performed in 37 patients of each group. There were no differences in the duration of the operations between the two groups (141.8 min in group 1; 142.1 min in group 2). There were no significant differences in intraoperative bleeding (266 mL, group 1; 309 mL, group 2). The bladder catheter was left for 8.3 days in group 1 and for 8.5 days in group 2 (Table 1).
There are no statistically significant differences between the two groups for any of the variables.
There were no secondary complications after the urethropexy, such as urine retention, pubic pain, or vesicourethral perforation from the Hem-o-lok.
From an oncologic point of view, both groups had a similar distribution of class pT2 tumors (76.5% in group 1; 80.4% in group 2). There were no differences in the rate of overall positive margins (11.8% in group 1; 13.7% in group 2), or in the apical location margins (2% in group 1; 3.9% in group 2) (Table 2).
There are no statistically significant differences between the two groups for any of the variables.
PSM=positive surgical margins.
After 3 months, 24/51 (47.1%) of the patients in each group declared continence (McNemar test and Fisher test: NS). After 6 months, 37/51 (72.6%) patients declared continence in group 1 and 34/51 (66.7%) in group 2 (P<0.005, McNemar test; P=0.67, Fisher test). After 12 months, 47/51 patients declared continence (92.2% in group 1), and 43/51 (84.3% in group 2) (P<0.05, McNemar test; P=0.35, Fisher test) (Fig. 2).
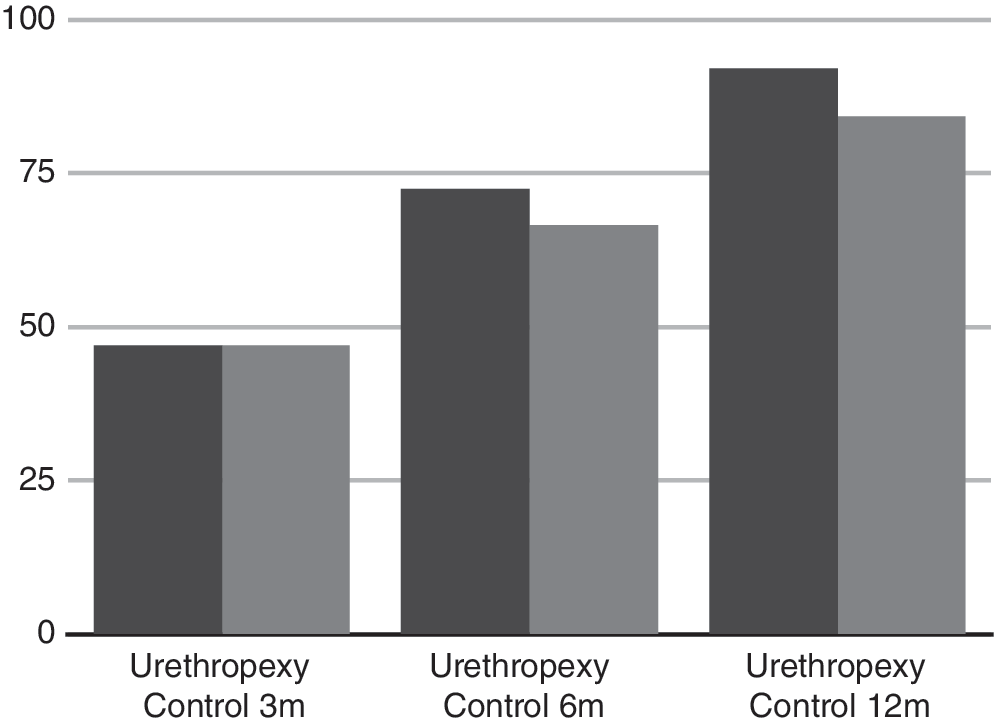
Continence recovery at 3, 6, and 12 months in urethropexy and control groups.
Discussion
Urinary incontinence is one of the main consequences of radical prostatectomy, causing morbidity and deterioration in quality of life. 1,6 Many technical variations have been described with the aim of reducing it, either during prostate dissection or in relation to the reconstruction of the pelvic floor of the urethral support after prostate excision.
During prostate dissection, it was attempted to improve continence by preserving the bladder neck 7,8 or preserving the puboprostatic ligaments. 9
Some authors described a significant improvement in early continence in cases of preservation of the bladder neck, 7,8,10 although others did not note any differences and even claimed an increase in the rate of positive margins (10% vs 0% P=0.08) when the preservation was performed. 11 It is a routine procedure for us to preserve the bladder neck and, in our series, in both groups, we performed this technique in a similar percentage (Table 1).
With regard to the preservation of the puboprostatic ligaments, Lowe 9 reported an increase in continence after 3 months, when the anterior urethral ligamentous attachments are not sectioned. This way, the urethra is more stabilized, and the degree of incontinence is reduced to around 30%. In robot-assisted surgery, Patel and associates 2 described a variant of puboprostatic preservation, which consists of executing a suspension point from the prostate tissue to the pubic periosteum before apical dissection. The rate of continence at 3, 6, and 12 months went from 78%, 89%, and 90% to 92.8% (P<0.03), 97.9% (NS), and 97.9% (NS), respectively. This beneficial effect of the preservation of the puboprostatic ligaments has been confirmed by other trials, 12,13 and none of them mentions an increase in the positive apical surgical margins. 2,9,12,13 In our case, we did not preserve the puboprostatic ligaments in any of the cases in our trial, for fear of multiplying the margins in this location. The low rate of apical margins we recorded in our series (2.9%), however, has made us consider this possibility in the future.
In radical retropubic prostatectomy, the use of fascia 4 or reabsorbable 14 suburethral slings has been described, achieving a rate of continence after 3 months of 87% and 93%, respectively. The inconveniences of this technique are a longer surgical period, the difficulty of performing minimally invasive surgery, and the risks of urine retention after insertion of the sling.
In robot-assisted surgery, Koliakos and colleagues 15 described the performance of an anterior and posterior urethral attachment, suturing the posterior fibrous tissue of the sphincter to the residual Denonvilliers fascia. This approach represents an improvement in continence after removal of the catheter, which went from 12.5% to 39%. Through the robotic preservation of the puboprostatic collar and the performance of a puboperineoplasty by means of three sutures on each side, Takenaka and coworkers 5 mention an immediate continence rate of 42.1% and 71.4% after 4 weeks.
Noguchi and colleagues 3 describe the attachment of the vesicourethral anastomosis to the dorsal complex by means of two sutures at the 11 o'clock and 1 o'clock positions, with a 53% improvement in continence after 1 month as opposed to after 3 months, of 73% against 47%. 3 Campenni and associates 6 describe the attachment of the periurethral tissue to the lower portion of the pubic bone, with 76% continence after 6 months for the group with the attachment as opposed to the 59% of the control group.
All the reconstruction techniques described above have the disadvantage of the complexity of performance by laparoscopy, because of the greater difficulty in applying these sutures by laparoscopy. The technique that we propose has the advantage of its ease of performance. Because the same suture as that with which we perform the anastomosis is used, we do not need to apply new laparoscopic stitches once we have completed the anastomosis. The advantage in continence in the medium term may be secondary to the fibrotic attachment of the urethra in a higher than normal position. The lack of effectiveness in the short term may be because a strict attachment is not made as in the cases in which two lateral stitches are applied; however, the advantage is that there is no urine retention from overcorrection. This technique could be used associated with other anti-incontinence mechanisms, such as the preservation of puboprostatic ligaments.
Conclusions
In our experience, simplified urethropexy is a simple, nontime-consuming technique that shows a slight clinical improvement in continence within 6 and 12 months, without reaching significant differences with the Fisher test. It would be necessary to perform a trial with a greater number of patients to confirm these data.
Footnotes
Disclosure Statement
No competing financial interests exist.