
Abstract
Purpose:
To evaluate the learning curve of a surgeon with no previous laparoscopy experience in performing robot-assisted radical prostatectomy (RARP).
Patients and Methods:
A total of 120 patients with a 1-year follow-up after RARP were included to the study prospectively. Patients were grouped as the first, second, and third 40 patients. Surgical, oncologic, and functional outcomes were compared among groups. Analysis of variance, chi-square, and Kruskal-Wallis test were used for statistical analysis.
Results:
All groups were similar with respect to age, prostate-specific antigen level, body mass index, Gleason score, and distribution of the clinical stage. The operative time was 182 minutes for group 1, 168 minutes for group 2, and 139 minutes for group 3 (P=0.01). Individual times of various stages of the procedure (dissection of the seminal vesicles, entering the extraperitoneal space and dissection of the endopelvic fascia, incision of the bladder neck, division of the prostatic pedicles and preservation of the neurovascular bundle, and urethrovesical anastomosis) decreased significantly over time. Estimated blood loss was 287 mL for group 1 238 mL for group 2, and 170 mL for group 3 (P=0.04). The length of stay was 5.1 days for group 1, 4.0 days for group 2, and 3.1 days for group 3 (P=0.005). Positive surgical margin rates were 22% (9) for group 1, 17% (7) for group 2, and 6% (2) for group 3 (P=0.03). While seven patients in group 1 and two patients in group 2 had biochemical recurrence, no patient in group 3 had biochemical recurrence (P=0.04). Continence rates at 12 months were 72.5%, 85%, and 92.5% in groups 1, 2, and 3, respectively (P=0.01). Potency rates at 12 months for groups 1, 2, and 3 were 60.5%, 66.7%, and 76.6%, respectively (P=0.03).
Conclusion:
Surgical, oncologic, and functional outcomes of RARP improve with increasing experience. Outcomes similar to the published series by high-volume centers could be achieved after 80 to 120 RARP cases.
Introduction
In this study, we aimed to define the learning curve of a surgeon in performing RARP without any previous laparoscopy experience in terms of surgical, oncologic, and functional outcomes.
Patients and Methods
Between July 2008 and September 2010, a total of 162 patients with clinically localized prostate cancer underwent RARP by the same surgeon with no previous laparoscopy experience. After a 3-day robotic surgery training (standard Intuitive Surgical accreditation course), the first three cases were performed under the supervision of a mentor. The surgical technique described for LRP by Guillonneau and Vallancien 6 was used in all cases.
After Institutional Review Board approval, perioperative and postoperative outcomes were collected in a prospective fashion. A total of 120 patients with a 1-year follow-up were included. Patients were grouped as the initial, the subsequent, and the last 40 patients. Preoperatively, all patients were continent and had an International Index of Erectile Function-5 score over 17. Surgical, oncologic, and functional outcomes were compared among groups. Operative time, estimated blood loss, transfusion requirement, positive surgical margin rate, biochemical recurrence rate, length of hospital stay, continence, and potency rates were compared. Estimated blood loss was calculated as the volume in the suction tube minus the sum of the irrigation volume and estimated urine produced after the opening of the bladder. Biochemical recurrence is defined as two consecutive prostate-specific antigen (PSA) values over 0.2 ng/dL. Continence is defined as 0 to 1 pad. The modified Clavien grading system was used for the assessment of complications. 7
The operative stages were defined as follows: Patient positioning, trocar placement, and docking of the robot as the first phase (phase 1), dissection of the seminal vesicles as the second phase (phase 2), entering the extraperitoneal space and dissection of the endopelvic fascia as the third phase (phase 3), ligation of the dorsal venous complex as the fourth phase (phase 4), incision of the bladder neck as the fifth phase (phase 5), division of the prostatic pedicles and preservation of the neurovascular bundle as the sixth phase (phase 6), and finally, anastomosis as the seventh phase (phase 7). The times for each phase were recorded and compared among groups.
Results
Patient demographics and preoperative data are shown in Table 1. All groups were similar with respect to age, PSA, body mass index, Gleason score, and distribution of the clinical stage. The mean operative time was 182 minutes in group 1, 168 minutes in group 2, and 139 minutes in group 3. The decrease in operative time was significant (P=0.001). The mean estimated blood loss was 287 mL in group 1. Estimated blood loss declined to a mean of 238 mL in group 2 and a mean of 170 mL in group 3 (P=0.04). Blood transfusion rates were 17%, 12%, and 4% in groups 1, 2, and 3, respectively (P=0.02). Overall complication rates were 27.5%, 16%, and 10% in groups 1, 2, and 3, respectively (P=0.02). Major complications (Clavien III and IV) occurred in 7.5%, 5%, and 0% in groups 1, 2, and 3, respectively (P=0.03).
PSA=prostate-specific antigen; BMI=body mass index.
The mean length of stay was 5.1 days in group 1, 4 days in group 2, and 3.1 days in group 3 (P=0.005). The urethral catheter was removed after a mean of 8.6 days. Positive surgical margin rates were 22%, 17%, and 6% in groups 1, 2, and 3, respectively (P=0.03). Biochemical recurrence in a 1-year follow-up occurred in seven patients in group 1, two patients in group 2, and none in group 3 (P=0.04, Table 2). Continence rates at 12 months were 72.5%, 85%, and 92.5% in groups 1, 2, and 3, respectively (P=0.01). Potency rates at 12 months for groups 1, 2, and 3 were 60.5%, 66.7%, and 76.6%, respectively (P=0.03).
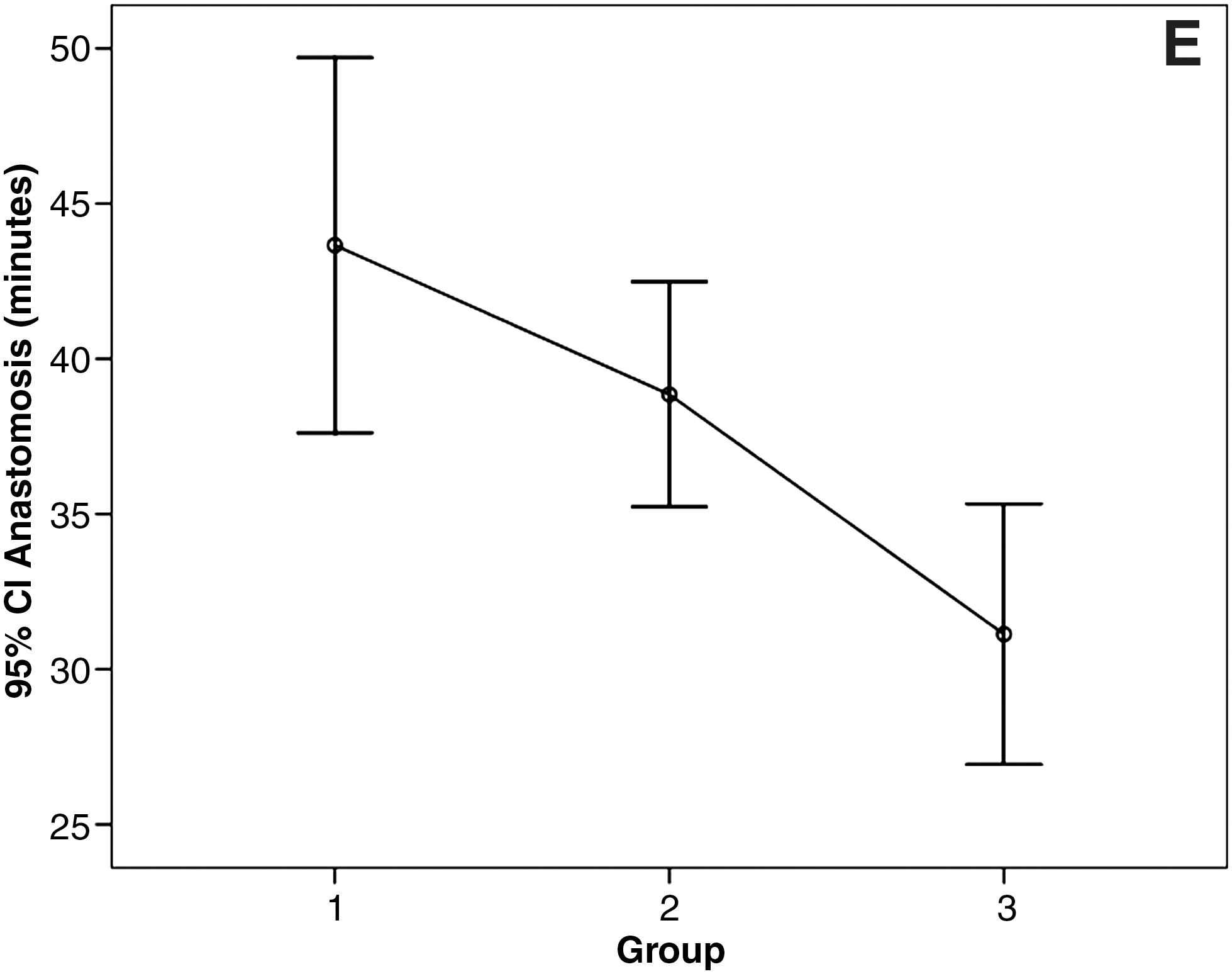
Comparison of the individual times for various phases of the procedure revealed that phase 1 (patient positioning, trocar placement, and robot docking) and phase 4 (ligation of the dorsal venous complex) did not improve over time (P=0.748 and P=0.234, respectively). Times for phase 2 (dissection of the seminal vesicles), phase 3 (entering the extraperitoneal space and dissection of the endopelvic fascia), phase 5 (incision of the bladder neck), phase 6 (division of the prostatic pedicles and preservation of the neurovascular bundle), and phase 7 (anastomosis) decreased significantly over time, however (Table 3, Fig. 1).

Comparison of the individual times for various phases of the procedure (error bars indicate the mean and 95% confidence interval [CI]).
There were 16 grade 2 (13 intraoperative or perioperative bleeding necessitating transfusion and 3 urinary tract infections) complications, 3 grade 3 (2 urinary anastomotic leaks necessitating cystoscopy and intervention, 1 port site bleeding) complications, and 2 grade 4 (1 rectal injury and 1 sepsis starting at postoperative day 25) complications (Table 2).
Discussion
New technology offers innovative options to further reduce the morbidity and improve the surgical, functional, and oncologic outcomes of radical prostatectomy. With the introduction of laparoscopic and robot-assisted surgery, the incisional morbidity has been significantly reduced. In addition, a recent cumulative analysis of comparative studies revealed that LRP and RARP were associated with positive surgical margin rates similar to those of open radical prostatectomy. 8
In a multi-institutional study, Palmer and associates 9 reported that the median operative time for RARP for surgeons with a median experience of 460 cases was 165 minutes. Our data reveal that a similar mean operative time of 168 minutes was reached after the initial 40 cases. In addition, the operative time in our series further decreased, indicating that superior outcomes should be expected with increasing experience.
In a review of outcomes reported by high-volume centers, which only included studies with at least 250 cases, the mean estimated blood loss for RARP was 164 mL. 10 In a study by Hakimi and colleagues 11 with an initial 75 RARP cases, the mean estimated blood loss was 230 mL. Our data revealed similarities with the published reports in the estimated blood loss of 238 mL in group 2 and 170 ml in group 3. The transfusion rates in groups 1 and 2 were rather high considering the estimated blood loss. The decision for blood transfusion was made by the attending anesthesiologist. The anesthesiology team had no previous laparoscopy or robotic surgery experience. Thus, we believe that there is also a “learning curve effect” for the anesthesiology team.
Menon and coworkers 12 reported 1.1 days of hospital stay after RARP. The length of hospital stay was 5.1, 4, and 3.1 days in groups 1, 2, and 3, respectively. While the decline in the length of hospital stay was statistically significant, it is substantially longer than the length of stay in the published series. This may be because of the discrepancies in health care systems and insurance company reimbursement methods of different countries.
In a recent study by Ou and colleagues, 13 the learning curve of reducing complications of RARP by a single surgeon was investigated. The authors reported complication rates of 18%, 12%, 18%, and 0% in their first, second, third, and fourth 50-patient groups. The major complication (Clavien III–IV) rates were reported as 6%, 2%, 4%, and 0% in the same groups. In our series, overall complications and major complication rates decreased significantly over time and reached to similar levels of the published series by high-volume surgeons.
Atug and associates 14 reported the positive surgical margin rates of the first 100 consecutive RARP patients divided in three groups based on the time of surgery. The positive margin rate was found to be 45%, 22%, and 11.7% in first, second, and third groups. In a recent study, Menon and coworkers 15 reported the overall positive surgical margin rate of 25.1% in a series of 1384 patients. Our data revealed a positive surgical margin rate of 22%, 17%, and 6% in groups 1, 2, and 3, respectively. While the low positive margin rate compared with data in published series may be because of patient selection bias, the decrease was statistically significant. In a review article, Jayram and associates 16 reported a biochemical recurrence rate of 21.3% in a 2-year follow-up. In another large series, the biochemical recurrence-free survival was found as 90.7% for 3 years and 86.6% for 5 years. 15 The biochemical recurrence rates in our series with a 12-month follow-up were 18% in group 1 and 5% in group 2. No biochemical recurrence occurred in group 3. The biochemical recurrence rate decreases significantly with increased experience and matches the rates in published series.
Functional outcomes, such as continence and potency rates, were reported in various studies to assess the learning curve and its impact on the outcomes. Despite the variation in definition of “continent” and “potent,” many authors published similar results in a 1-year follow-up. Menon and colleagues 4 reported a 96% continence rate in a 6-month follow-up. Joseph and coworkers 17 and Krambeck and associates 18 also reported 90-91.8% continence rate with a 12-month follow-up. Our data in the last 40 patients revealed a similar continence rate compared with the published series. The increase in the continence rate was statistically significant, and one can speculate that results similar to published data could be reached after 80 RARP cases. Correspondingly, several high-volume surgeons with large series reported their potency rates after RARP. At a 12-month follow-up, potency rates were found to be 70% to 78%. 12,19,20 Our data demonstrated that comparable results in potency could be achieved after 80 cases.
Ahlering and coworkers 5 reported that a laparoscopically naive yet experienced open surgeon could successfully transfer open surgical skills to a laparoscopic environment in 8 to 12 cases using a robotic interface. Palmer and associates 9 claimed that basic proficiency could be obtained with 40 RARP cases. The authors suggested, however, that obtaining “satisfactory outcomes” would take longer, from 100 to 300 cases. Our data showed significant decrease in total operative time, times of selected phases of the procedure, estimated blood loss, complication rate, positive margin rate, and biochemical recurrence rate. With the significant increase in continence and potency rates in 80 to 120 cases, outcomes similar to published series were achieved. We strongly believe that better outcomes will be achieved with increasing experience. Our data, however, revealed that a surgeon without any previous laparoscopy experience could achieve similar surgical, oncologic, and functional results of the high-volume centers after 80 to 120 cases of RARP.
Conclusion
Surgical, oncologic, and functional outcomes of RARP improve with increasing experience. Outcomes similar to the published series by high-volume centers could be achieved after 80 to 120 RARP cases.
Footnotes
Disclosure Statement
No competing financial interests exist.