
Abstract
Background and Purpose:
Transurethral resection of the bladder
Methods:
PubMed, MEDLINE, ISI Web of Knowledge, EBSCO, EMBASE, and Biomed Central databases were searched for reports in English from 1980 to June 2010. The end point was prevalence of persistent urothelial bladder cancer of any stage and grade at repeated TURB, assessed separately for Ta and T1 lesions at TURB. Persistence was presence at repeated TURB of same or lower stage cancer as at TURB; upstaging was presence of higher stage.
Results:
There were 2327 original articles and 562 reviews retrieved. Data from 15 studies were pooled and analyzed. Prevalence of T1 was reported in all and of Ta in 8. Persistence rate prevalence at repeated TURB was 0.39 (95% confidence interval [CI]=0.26 to 0.54) for Ta and 0.47 (95% CI=0.41 to 0.53) for T1. Persistence was 19.4% to 56% and 15.2% to 55%, and upstaging occurred in 0% to 14.3% of Ta and 0% to 24.4% of T1 at repeated TURB, respectively.
Conclusion:
High percentages of persistence and upstaging confirm a repeated TURB is needed in patients with high-risk nonmuscle-invasive bladder cancer. Further investigation is encouraged taking risk stratification into consideration to evaluate the role of repeated TURB in low- and mid- risk diseases.
Introduction
In cases of bladder cancer, TURB in general has become crucial for correct staging, diagnosis, and treatment. 8,9 It serves to identify patients for conservative treatment, organ-sparing strategy, or radical cystectomy despite its limitations, which are mostly biologic or operator dependent. Not all lesions are visible at first resection; judging the depth of resection is difficult if muscularis propria sampling is not performed; thus, the expertise of the operator is a crucial factor. Other difficulties include multiple cancer growths, location within a diverticulum, dome or bladder anterior wall, trabeculated or thin bladder wall, and risk of incidental perforation. 10 Another limit, despite being still controversial, is the potential development of a new lesion secondary to implantation of tumoral cells.
All these factors could compromise outcomes in terms of recurrence rate at the first follow-up cystoscopy. 8 In fact, guidelines generally recommend repeated TURB within a short time if the initial resection was incomplete, if multiple or large tumors were present, if there was a lack of muscularis propria in the specimen, and if a high-grade nonmuscle-invasive tumor or a T1 tumor was detected. 2,8,11
Because no randomized clinical trials or systematic reviews have been published on the role of repeated TURB in providing additional diagnostic and potential prognostic information and there are no data to support repeated TURB in Ta lesions, 12 we reviewed all data and performed a meta-analysis on the role of a repeated transurethral resection in nonmuscle-invasive urothelial bladder cancers. This analysis of available reports aimed at assessing persistence and upstaging of nonmuscle-invasive bladder cancer at second look.
Methods
Search strategy protocol
The entire process selection (ie, searches, selection, and study exclusion) was performed by AV and EC. Data for this review and meta-analysis were obtained by searching PubMed, MEDLINE, ISI Web of Knowledge, EBSCO, EMBASE, and Biomed Central databases. Search terms were: “bladder cancer,” “bladder neoplasm,” “cystectomy,” “second look,” “II look,” “second resection,” “repeat resection,” “re-tur,” and “repeat tur” in all articles and conference proceedings published in English between January 1980 and June 2010. Reviews and original clinical studies with abstracts were selected. Inclusion criteria: White-light repeated TURB performed to assess persistence of primary urothelial bladder cancer shortly after white-light TURB. Exclusion criteria: Incomplete TURB (as defined by authors), endocavitary adjuvant therapy after TURB because it could influence pathologic assessment at repeated TURB, resections with sources other than white light and different endoscopic techniques (eg, fluorescence followed by white light) for TURB, and repeated TURB because white-light TURB is the gold standard and because fluorescence, although improving endoscopic detection of bladder cancers, does not indicate stage adequately. 13
Because alternative techniques such as bipolar electrocautery and lasers are still under investigation, 12 they were excluded. We also checked the reference lists of every selected clinical study and review. Studies coming from the same database were excluded. The full strategy is available from the corresponding author.
Data extraction
MDL extracted data, after discussion to solve eventual discrepancies and reach consensus with AV and EC. From each eligible study, they recorded first author, year of publication, journal, type of publication (article or conference proceeding), type of study (retrospective or prospective), sample size (number of patients undergoing TURB and repeated TURB), and time between TURB and repeated TURB. Stage, grade, number and dimensions of lesions at TURB and at repeated TURB were obtained. Histologic characteristics at TURB and at repeated TURB were assessed separately for Ta and T1 lesions, and Tis was indicated. Because of the wide range of time the present review was conducted, the grading of urothelial bladder cancer was reported in accordance with the World Health Organization classification and T classification in accordance with the tumor, nodes, metastasis system from the American Joint Committee on Cancer.
The clinical end point was the prevalence of urothelial bladder cancer of any stage and grade at repeated TURB. Although adjuvant treatments, recurrences, and development of invasive disease depend not only on stage but also on grade, dimension, and number of lesions, stratification according to Ta or T1 at TURB served to determine whether stage was an indicator for repeated TURB in nonmuscle-invasive urothelial bladder cancer.
Persistence was defined as presence, at repeated TURB, of same or lower stage urothelial bladder cancer as at TURB; presence of higher stage cancer was considered upstaging. Persistence and upstaging of isolated Tis was not considered in the present analysis because Tis has a different natural history, clinical manifestations, diagnostic approach, treatment, and prognosis.
Because no individual, identifiable patient data were used in this review or meta-analysis, ethics approval or informed consent was not needed for this research project.
Statistical analysis
Statistical analysis was performed by VB. Rates of bladder cancer prevalence at repeated TURB were extracted from selected studies and combined applying a random-effect model (DerSimonian and Laird method) 14 that incorporates heterogeneity of effects. Heterogeneity of studies was evaluated by the Cochrane Q test and I2 statistics, which describe the percentage of total variation across studies that is because of heterogeneity rather than chance. 15 Heterogeneity was considered significant if P<0.10 and I2 was more than 50%. Begg and Egger tests 16,17 were used to test for publication bias. In a sensitivity analysis, we assessed the influence of individual studies on pooled estimates according to the Tobias method. 18 If the point estimate with one study omitted lay outside the confidence interval (CI) of the overall estimate of all trials, the study was indicated as having excessive influence. Meta-analysis calculations were performed using StatsDirect statistical software version 2.7.2.
Results
There were 2327 original clinical articles and 562 reviews screened for retrieval; 101 potentially eligible studies were selected, 54 of which were duplicates; 47 articles were retrieved, and 18 articles matched inclusion and exclusion criteria. 19 –36 (Fig. 1) Three conference proceedings were excluded because they were also published later as articles and thus considered duplicates. 34 –36 Finally, data were pooled and analyzed from 15 studies reporting histologic assessments of bladder cancer at repeated TURB. 19 –33 All focused on the role of the repeated TURB in T1 diseases at TURB; eight also dealt with the repeated TURB in Ta. 22,23,25 –27,29,31,33

Flowchart.
Study characteristics (Table 1)
All studies were published in peer-reviewed journals between the 1998 and June 2010; six were conference proceedings, 19,22 –24,29,30 and nine were clinical articles. 20,21,25 –28,31 –33 Six were retrospective studies, 20,26 –28,31,33 two prospective, 21,25 and study design was not specified in nine. 19,22 –24,29,30,32
5/47 pts underwent cystectomy after the TURB.
177 patients underwent repeated TURB, but 53 were T2 at TURB and not included in this study.
194/214 patients had bladder cancer diagnosed at TURB; 124/194 patients had a superficial disease and were eligible for II look; 41 pts did not undergo repeated TURB because 12 had small unifocal TaG1 tumor, 8 showed a poor performance status, 20 refused the operation, and 1 underwent immediate cystectomy. Finally, 83 pts underwent repeated TURB.
13/149 pts were ineligible for repeat TURB.
Pts=patients; TURB=transurethral resection of the bladder; n=number of patients; w=weeks; Eur Urol=European Urology; A=abstract; NA=not available; J Urol=The Journal of Urology; P=paper; Re=retrospective; Pr=prospective; J Endourol=Journal of Endourology; BJU Int=British Journal of Urology International; Urol Int=Urologia Internationalis.
The studies included 2464 patients who underwent TURB; 202/2464 (8.2%) patients were not considered in the analysis performed in four studies. 20,23,25,32 In 20 patients, bladder cancer was not the diagnosis, 2 patients showed Tis, 12 small unifocal TaG1, 21 complained poor performance status, 20 refused, and 127 underwent cystectomy because of a muscle-invasive disease or because an extensive superficial disease was considered to be incurable by TURB. 20,23,25,32 Finally, 2262/2464 (91.8%) patients underwent repeated TURB after 2 to 8 weeks for a nonmuscle-invasive bladder cancer.
At TURB, 816/2262 (36%) had Ta, 22,23,25 –27,29,31,33 1432 (63.4%) T1, 19 –33 and 14 (0.6%) an isolated Tis. 23,26,29,31 Tis was associated in 631 of 2262 (27.9%) patients undergoing repeated TURB. 19,20,26 –28,30,32 Solitary lesions were present in 4.5% to 71.3% and multiple lesions in 28.7% to 95.5% of patients 21,23,25,28,30 –33 (Table 2).
With/without.
1 isolated Tis, 3 associated with T1 lesions, and 1 with Ta.
135 TaG1,one TaG1+Tis; 72 TaG3, 255 TaG3+Tis; 10 T1G1, 16 T1G1+Tis; 20 T1G3, 20 T1G3+Tis.
n=number of patients; NA=not available; G=grade of differentiation.
Because two studies excluded patients in whom a muscle-invasive disease developed at repeated TURB, 27,28 upstaging was evaluated in 353/816 patients with Ta and 833/1432 patients with T1 disease at TURB, respectively. 19 –26,29 –33
Ta at TURB and II look
At TURB, 173/816 (21.2%) patients with Ta were G1, 106 (12.9%) were G2, 349 (42.7%) were G3, 26,27 and grading was not assessed in 188 (23%). 25,29,33 In 256/816 (31.4%), Tis was associated 26,27 (Table 2). Ta were solitary lesions in up to 63% of cases and multiple in up to 57%. Lesion sizes were not reported in any study. The II look was positive in the same location where the TURB had been performed in 46%, in a different site in 19%; the remaining showed disease both at the primary site and in at least one different location. 25
At repeated TURB, 405/816 (49.6%) patients were disease free (T0), 256 (31.4%) had Ta, 39 (4.8%) had T1, 10 (1.2%) had T2, and 106 (13%) had Tis. One study alone reported 105 of these 106 cases of Tis. 27 At repeated TURB, Ta disease persisted in 256/816 (19.4%–56%) patients, and upstaging was present in 49/353 (0%–14.3%) (Table 3). 22,23,25,26,29,31,33
TURB=transurethral resection of the bladder; N=number of patients; G=grade; NA=not available.
T1 at TURB and II look
At TURB, 85/1432 (5.9%) patients with T1 were G1, 198 (13.8%) were G2, 883 (61.7%) were G3, 20 –22,24,26 –28,30 –32 and in 299/1432 (20.9%) patients, grading was not clearly assessed. 19,23,25,29,33 In 511 (35.7%) patients, Tis was associated. 19,26 –28,30,32 T1 diseases were solitary in up to 71.3% of patients and multiple in up to 95%. 21,23,25, 28,30 –33 Lesion sizes were not reported in any study (Table 2).
At repeated TURB, 719/1432 (50.2%) patients were disease free (T0), 132 (9.2%) had Ta, 322 (22.5%) had T1, and 185 (12.9%) had Tis, with a persistence in 454/1432 (15.2%–55%) patients, 19 –33 and an upstaging in 74 of 833 (0%–24.4%) patients (Table 4). 19 –26,29 –33 At repeated TURB, T1 disease was present at the same site where the TURB had been performed in 44% to 86% and in a different location in 14% to 56%. 19,21,25,32
With/without.
The authors did not analyze patients with muscle-invasive disease at repeated TURB.
n=number of patients; G=grade of differentiation; Tis=carcinoma in situ; NA=not available.
TURB technicalities
Nine of 15 studies reported technical aspects of TURB, with Ta persisting in 19.4% to 56% of patients and upstaged in 3.9% to 8% and T1 persisting in 21.7% to 55% of patients and upstaged in 0% to 23%, respectively. 19,21,23,25,26,28,31 –33 Margins of lesions were sampled during the TURB in five studies, 21,25,26,28,31 with a persistence of 25.4% to 56% for Ta and of 25% to 55% for T1; the upstaging was 6.3% to 8% and 0% to 23.3%, respectively. Tumor base was sampled at TURB in four studies 21, 28,31,32 in which Ta diseases persisted in 32.3% and upstaged in 6.4%, 31 respectively; however, T1 persisted in 25% to 32.7% and was upstaged in 3.7% to 9.5%, respectively. 21,28,31,32 Locations of lesions was marked on a map in five studies. 19,21,23,25,32 Ta persisted at II look in 19.4% to 25.4% with an upstaging of 5.5% to 6.4%; however, T1 persisted in 26.2% to 55% and was upstaged in 0% to 10.5%, respectively. In two studies, the II look was performed by an expert surgeon; the persistence of Ta was 56% with an upstaging of 8% 26 ; however, T1 persisted in 26.2% to 40% and was upstaged in 3.7% to 23.3%, respectively. 21,26 In two studies, the II look was performed either by skilled surgeons or by trainees; Ta persisted in 22.2% to 32.3% and was upstaged in 5% to 6.4%; T1 persisted in 21.7% to 25% and was upstaged in 1.7% to 7.9%, respectively. 31,33
Four abstracts and two articles did not provide surgical details of either TURB or II look in 1055 patients. At repeated TURB, Ta persisted in 22% to 36% of patients, and lesions were upstaged in 0% to 14%. T1 persisted in 15.2% to 52% of patients, and lesions were upstaged in 0% to 24.4%. 20,22,24,27,29,30
Meta-analysis
We included eight studies in the meta-analysis of the Ta prevalence rate at II look and 15 in meta-analysis of the T1. As the heterogeneity test was highly significant (I2>80%, P<0.0001) in both analyses, the random-effects models were preferred to fixed-effects models. Beggs and Egger tests did not show significant publication bias. Sensitivity analysis did not result in loss of significance when one study was excluded at a time in both meta-analyses. The pooled prevalence rate of Ta at II look was 0.39 (95% CI=0.26 to 0.54) as shown in the forest plot (Fig. 2). The pooled prevalence rate of T1 at second look was 0.47 (95% CI=0.41 to 0.53) (Fig. 3). The pooled prevalence rate in studies in which multiplicity was assessed was not significantly different compared with the global prevalence rate (0.33, CI=0.26 to 0.4 for Ta; 0.46, CI=0.39 to 0.53 for T1). The pooled prevalence rate in studies that did not exclude patients in whom a muscle-invasive disease developed was not significantly different compared with the global prevalence rate (0.35, CI=0.26 to 0.44 for Ta; 0.45, CI=0.38 to 0.52 for T1).
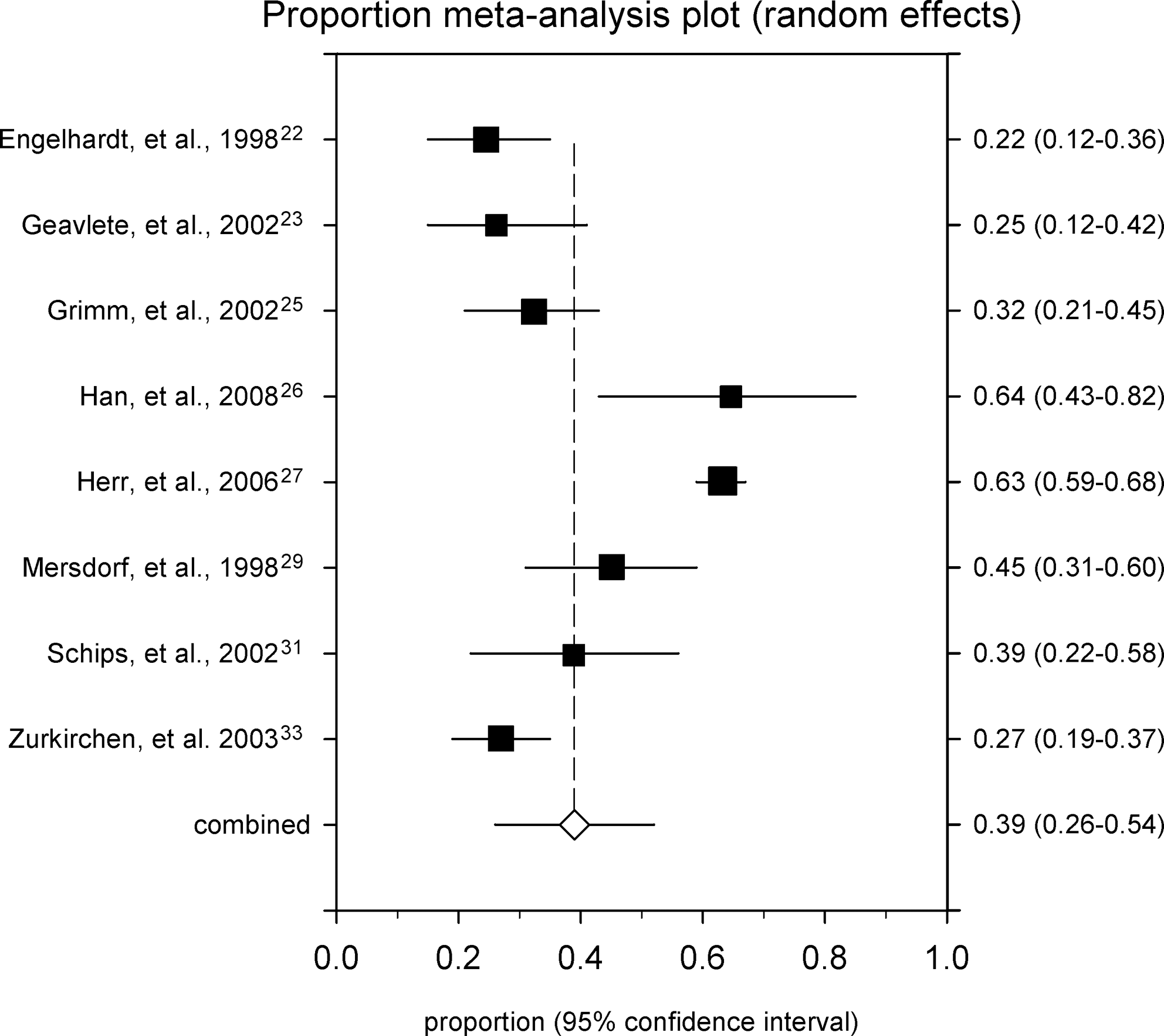
Prevalence rates of Ta bladder cancer at II look.
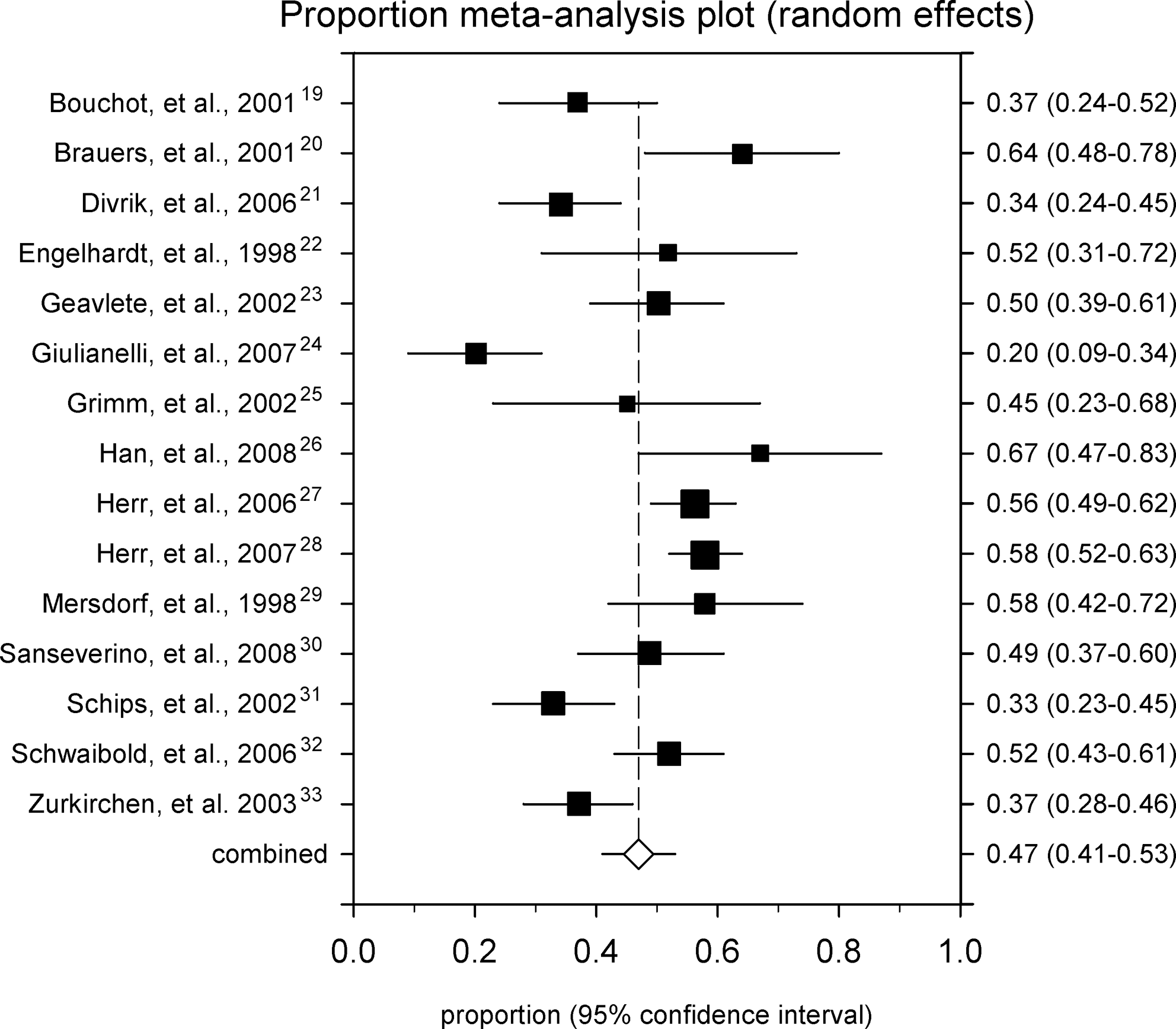
Prevalence rates of T1 bladder cancer at II look.
Discussion
The results of this first meta-analysis on the role of white light repeated TURB in the management of nonmuscle-invasive urothelial bladder cancers underlined the necessity of a continuous improvement of the endoscopic approach in accordance with a prevalence in Ta diseases of 39% and in T1 diseases of 47%, respectively. The high percentages of persistence and upstaging seemed linked to procedure-related technicalities, that are only partially overcome with separate resections of exophytic tumor, margins and base. 37,38
Margins were sampled in 5 of 15 studies, but the authors did not describe the technique. For instance, they did not indicate where margins were sampled and how many specimens were collected. 21,25,26,28,31 Despite margin sampling, Ta persisted in 25.4% to 56% and was upstaged in 6.3% to 8% of patients 25,26,31 ; T1 persisted in 25% to 55% and was upstaged in 0% to 23.3% at the II look, respectively. 21,25,26,28,31 Because the repeated TURB was positive in the same site where the TURB had been performed in up to 46% both in Ta and T1 diseases, 21,25 these resections could have been microscopically incomplete along the borders of the diseases. On the other hand, the need to sample tumor bed muscular layer has long been known.
Herr and associates 39 reported that when muscularis propria was present in specimens collected at the TURB, only 14% of T1 were upstaged compared with 49% of nonsampled cases. The present review underlines that when muscle is not clearly stated to be present in the TURB specimens, upstaging was 14.3% for Ta disease 29 and 23.3% for T1, respectively. 26 If the tumor base was sampled during the TURB, upstaging dropped to 6.4% for Ta disease 31 and to 9.5% for T1, 32 respectively. The unexpectedly 23.3% upstaging rate of T1 diseases assessed by Han and colleagues 26 seems secondary to the fact that the authors had operated on patients who were referred to their institution from other hospitals and no information was available on the first TURB techniques that had been performed elsewhere. 26
To improve high persistence and upstaging, different approaches such as using a bladder diagram, sampling suspicious areas and normal mucosa, or new technologies seem useful.
Using a bladder diagram would be useful to indicate tumor size, its location, as well as any tumor-suspicious areas. Photos or video pictures should also be taken. 37,38 Writing down disease position on a map would not only record sites resected at the TURB but would also help make the repeated TURB more accurate. In five articles that used a bladder map, persistence was assessed as up to 86% at the primary site and up to 56% elsewhere. 19,21,23,25,32 Furthermore, quality control of surgical procedures during follow-up cystoscopy could also be performed by analyzing exact locations of tumor recurrences, distinguishing whether lesions had been missed or were really early recurrences. To our knowledge, relationships between tumor sites, recurrence, and progression during follow-up cystoscopies have never been investigated.
Several authors suggested suspicious areas and normal mucosa should undergo biopsy, because high-grade, multiple Ta and T1 diseases showed significantly higher incidence of positive biopsies. 9,40 On the other hand, the role of random bladder mucosa biopsies during TURB is still controversial; in fact, patients who did or did not undergo biopsy showed similar recurrence and progression rates, even though they are reported to detect abnormalities in up to 24% of patients and determine a treatment switch in up to 7% of patients 9 We can argue that random biopsies are useful. At the II look, T1 diseases were discovered in areas other than those where the TURB had been performed in 16% to 56% 19,21,25,32 ; however, Herr and Donat 27 assessed that the 78% of patients in whom a stage progression developed complained of recurrence in remote sites within the bladder, with Ta diseases recurring in 83% to 86%. A possible explanation is that lesions might have been overlooked, because apparently normal mucosa was not routinely sampled at TURB and the repeated TURB was performed shortly afterward.
Using different methods, such as PPD photodynamic diagnosis (PPD) or narrow band imaging (NBI), could lower the persistence rate. The additional detection rate for PPD was higher than for white light cystoscopy (5%–49%) for nonmuscle-invasive tumors, with positive II look in 4.5% to 32.7%, lower than in cases of white light (25.2%–53.1%). 41 In addition, NBI seems an alternative and promising optical technology that enhances images of capillaries in the bladder mucosa; moreover, it has little cost and can be used an unlimited number of times in each patient without the necessity to instill a fluorescent agent. 42 NBI detected additional carcinoma in 41% of patients, 43 with sensitivity of 69% to 92% and specificity of 58% to 79%, 44 comparable to white light, and without the necessity of a long learning curve. 44
Despite their limitations, both PPD and NBI seem helpful in detecting bladder cancers and for a complete resection of all lesions. PPD allows better resection and coagulation of Tis, and NBI could increase the detection of small tumors or areas of cancer growth enhancing the contrast between the neoplastic and normal mucosa and facilitating a better identification of tumor margins.
According to the results of Zurkirchen and coworkers, 33 the importance of surgical skill seems unclear. The authors found 34.8% persistence and 1.7% upstaging rates, independent of whether the TURB was performed by a senior urologist or a trainee. Justification for this apparently contradictory discrepancy was that senior surgeons had to handle more difficult cases and, because they had to help whenever a resident was faced with a difficult resection, operations were considered to have been performed by experts. 33 Authors stated operations were performed by “senior urologist or trainee with help of the senior” without further descriptions of procedures. Even though TURB is considered a relatively simple procedure, a learning curve is needed to have enough experience to deal with “difficult” bladder cancers.
Guidelines from the European Association of Urology, the American Urological Association, and the First International Consultation on Bladder Tumors suggested performing repeated TURB when there was a lack of muscle in the sample specimen, when TURB was incomplete, when a high-grade nonmuscle-invasive tumor was present, and when a T1 lesion was detected. 2,11,45 In fact, according to current literature, 10% of Ta and 35% of T1 invade the muscle wall, and 5% of patients with the former and 20% with the latter undergo cystectomy. 46
According to these guidelines, repeated TURB was indicated in 1851 (81.8%) patients in this meta-analysis 19 –33 ; on the other hand, 431 of 816 (52.8%) patients with Ta disease did not clearly fulfill criteria for a repeated TURB. 22,23,25 –27,29,31,33 Information for a correct risk stratification depending on the number and dimensions of lesions, previous recurrence rate, stage at the resection (Ta or T1), presence of Tis, and grade of differentiation 47 are provided for none of those 431 patients. They did not have high-grade disease, Tis was associated with a noninvasive lesion in only two cases, tumor dimensions were not assessed, and lesions varied widely in number. The repeated TURB, however, led to a switch in treatment for up to 18% of patients in studies including 63 patients with Ta and 317 with T1 disease at TURB. 19,21,25,31,32 According to current reports, the 3-year recurrence rate is up to 48% in patients who undergo TURB without a II look, 48 compared with 33% in a series of 63 patients with Ta and 20 with T1 disease who underwent the repeated TURB. 25
II look appeared to impact favorably on the outcomes of superficial bladder cancers with higher probability to achieve a complete response than a single transurethral resection (TUR) (71% vs 43%); in fact, as Herr 49 has prospectively assessed, both Ta and T1 diseases progressed less frequently in the case of re-TUR when compared with a single resection (7% vs 31% for Ta and 8 vs 43% for T1). Furthermore, in a randomized clinical trial, Divrik and colleagues 50 assessed a recurrence-free survival rate of 69% vs 37% at 3 years (median 27 vs 12 mos), with 81% of recurrences occurring during the first year after the single resection.
Despite this significant influence on outcome because of better local therapy and significant changes in management, from the present review, II look does not clearly seem justified in all patients who are affected by superficial bladder cancer. In addition to the above, further aspects difficult to measure would modify the behavior of the disease, and thus the approach: Previous history of tumors, size, location, and configuration of the neoplasms; if lamina propria, muscle, and fat were seen; and endoscopically free of tumor. The II look, however, seems drive the outcome regardless of the stage of the disease, because recurrence and progression rates were similar in patients who were affected by Ta or T1 tumors after one or two TURBs. 49
We acknowledge that our meta-analysis is beset by some flaws. Tis was associated in 27.9% of patients, persisting in up to 25%. 20,26 –28,30,32 The most important variable, however, was the completeness of the first resection, because unresected tumors are unlikely to be controlled by endovesical adjuvant therapy; in fact, Tis was not independently associated with higher risk of developing muscle-invasive forms of bladder cancer. 49 Despite the fact that, in two studies, patients in whom a muscle-invasive disease developed at repeated TURB were not taken into consideration, 27,28 excluding those studies, the pooled prevalence rate did not change significantly if compared with the global rates assessed by the meta-analysis. Thirteen studies did not state whether patients showed recurrent tumors at the first resection. Such recurrences are more aggressive. Only two studies reported minor complications in 5/216 (2.3%) patients 21,32 ; on the other hand, this percentage is in line with current literature.
Ideally, studies included in systematic reviews and meta-analysis should be comparable with rigorous study design and with unbiased experimental methods and should evaluate the same outcome. Unfortunately, the prevalence of persistence was a secondary and comparable outcome only in a few observational studies included here, because no randomized clinical trials matched the inclusions and exclusion criteria. Moreover, populations were generally small; thus, heterogeneity was an unavoidable problem not completely resolved by adopting a random-effects model.
Conclusion
This first meta-analysis on the role of repeated TURB in the management of nonmuscle-invasive bladder cancers showed 39% of Ta and 47% of T1 tumors persisted at the II look. The heterogeneity revealed by the present review underlines that the effectiveness of the II look in some situations is still controversial, especially in low- and middle-risk diseases. The re-TUR reduces and solves many but not all the uncertainties, but is clearly an overtreatment in some situations. We are confident that our effort in performing this systematic review can stimulate the development of prospective studies to optimize the surgical management of urothelial bladder cancer in accordance with proper risk stratification.
Footnotes
Disclosure Statement
No competing financial interests exist.