
Abstract
Purpose:
To assess the impact on visual analog scale (VAS) pain scores of allowing male patients to view the procedure of flexible cystoscopy.
Patients and Methods:
A total of 86 male patients admitted to our hospital for flexile cystoscopy by a single urologist between 2010 and 2011 were randomized to two equal groups. Group 1 included 43 patients who were allowed to watch the video screen with the urologist. Group 2 included 43 patients who were unable to view the video monitor. All patients received the same real-time explanation during the cystoscopy. Patients recorded their pain feeling on a VAS ranging from 0 to 10 after the physician completed the cystoscopy. The pulse and respiratory rate were also recorded 5 minutes before the procedure and immediately after the procedure.
Conclusion:
Real-time visualization of flexible cystoscopy with simultaneous explanation improves male patients' comfort.
Introduction
Patients and Methods
A total of 86 male patients who were admitted to our hospital for flexile cystoscopy by a single urologist between January 2010 and January 2011 were randomized to two equal groups. Ethics review and approval was obtained, and every patient provided full written and informed consent. Indications for flexible cystoscopy included hematuria, surveillance for bladder tumors. Patients who accepted other procedures, including biopsies, urethral dilation, stent removal, and stent placement, were excluded from this trial. Any patient who was undergoing manipulation of the lower urinary tract was also excluded from the study. Patients with a history of chronic pelvic pain syndrome were also excluded.
Patients were informed of the study and then randomized to either group 1 or group 2. A random number was referenced to determine patient groups in the cystoscopy room. The staff urologist had a random number list to ensure an equal number in the two study groups. Patients were randomized into two groups: Group 1 included 43 patients who were allowed to watch the video screen with the urologist. Group 2 included 43 patients who were unable to view the video monitor. Both groups received real-time explanations before and during the procedure. Of the 86 flexible cystoscopies, 31 (14 in group 1 and 17 in group 2) were performed for diagnostic purposes, with the remainder being surveillance procedures. Twenty-six (12 in group 1 and 14 in group 2) were undergoing cystoscopy for the first time, with the remainder undergoing repeated cystoscopy.
All patients received local anesthesia with 10 mL intraurethral 2% viscous lidocaine for 3 minutes before flexible cystoscopy. All procedures were performed using a 16F flexible cystoscope (Olympus CYF-5A), 70-degree rod lens, digital camera (Olympus OTV-S7), and color video monitor (Olympus OEV-191H). Patients recorded their pain feeling on an VAS (visual analog pain scale) ranging from 0 to10 after the physician completed the cystoscopy. We defined no pain as a score of 0, mild pain as a score of 1 to 3, moderate pain as a score of 4 to 7, and severe pain as a score of 8 to 10. 2 The pulse and respiratory rate were also recorded 5 minutes before the procedure and immediately after the procedure.
We used SPSS version 13.0 to analyze data. VAS score was compared between groups using the Mann-Whitney U test, with P<0.05 considered statistically significant. The independent-samples T test was used to determine differences in vital signs between the two groups.
Results
The mean (±standard deviation) patient age was 62.9±10.5 years in group 1 and 64.5±11.2 in group 2 (P>0.05); age distribution in both groups was comparable. The ratio of patients who had previous cystoscopy in both groups was comparable (72.1% vs 67.4%, P>0.05). The mean duration of the procedure was 7.7±1.4 minutes in group 1 and 8.1±1.5 minutes in group 2 (P>0.05) (Table 1). Two patients in group 1 and one patient in group 2 were excluded for arrhythmia when comparing the preprocedure and postprocedure pulse. The preprocedure pulse and respiratory rate were comparable in both groups (P>0.05). There was no statistically significant difference in the postprocedure pulse rate and respiratory rate between groups (Table 2). Mean pain score on VAS was 1.12 (95% confidence interval [CI] 0.82 to 1.41) in group 1 and 3.33 (95% CI 2.55 to 4.10) in group 2. Patients who were allowed to watch the video screen experienced less discomfort at cystoscopy (P<0.001) (Fig. 1) (Table 2). Especially in patients who were undergoing their first or repeated cystoscopy, as well as in those who were undergoing flexible cystoscopy for diagnostic or surveillance purposes, we found that real-time visualization is effective in reducing their pain (Table 2). Classification of pain in the two groups is shown in Table 1.
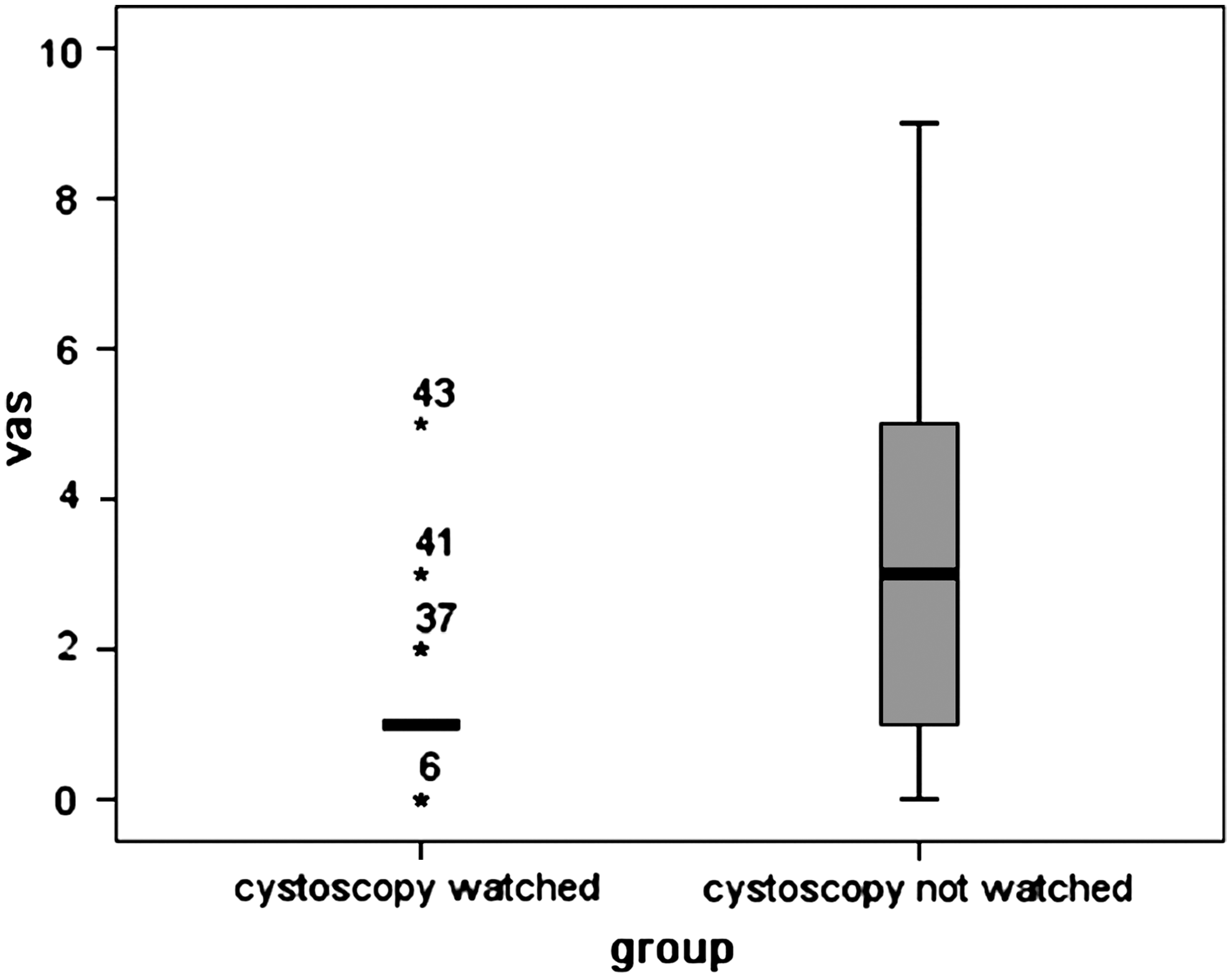
Mean pain score on the visual analog scale was 1.12 (95% confidence interval 0.82 to 1.41) in group 1 and 3.33 (95% confidence interval 2.55 to 4.10) in group 2.
SD=standard deviation.
Discussion
Previous studies examined maneuvers to reduce discomfort of men who were undergoing cystoscopy, including an assessment of the volume, 3 rate of delivery, 4 temperature of lubrication, 5 and the use of transcutaneous electrical nerve stimulation. 6 Some randomized controlled trials reported mixed results for the effectiveness of topical intraurethral lidocaine gel as local anesthesia during flexible cystoscopy. Recent meta-analysis confirmed the hypothesis that there is no statistically significant difference in the efficacy of pain control between lidocaine gel and plain gel lubrication in men during flexible cystoscopy. 7
In our trial, we demonstrate that the VAS score among male patients who watched the flexible cystoscopy procedure with simultaneous explanations was significantly lower, either in the patients with first ever cystoscopy or with repeated cystoscopy. There was no statistically significant difference in the postprocedure pulse rate and respiratory rate between the two groups. Several previous published studies have studied the impact of visualization and detailed explanation of procedure on decreasing the pain score. Patel and associates 8 and Soomro and colleagues 9 stated that male patient viewing of the cystoscopic procedure is a useful tool for reducing the discomfort experience during flexible cystoscopy. This statement is supported by our results. Cornel and coworkers, 10 however, reported that the pain experienced by male patients undergoing flexible cystoscopy is not strongly influenced by viewing the procedure.
Although our study showed no significant difference in the postprocedure pulse rate and respiratory rate between groups, which is consistent with the study by Soomro and associates, 9 the variations of pulse and respiratory rate in group 1 are less than group 2, however, potentially indicating that watching the flexible cystoscopy procedure with simultaneous explanations might smooth patients' mood and reduce their discomfort.
As we know, the external urinary sphincter lies at the level of the pelvic floor. Two trials have confirmed that the most painful part of flexible cystoscopy is when the tip of the cystoscope traverses the external sphincter. 11,12 In our experience, this is a critical part that could be targeted by strategies for reducing the discomfort experience. Gunendran and colleagues 13 stated that increased hydrostatic pressure by simple manual compression of the irrigation solution bag (500 mL of 0.9% saline) during cystoscope passage through the bulbar urethra just distal to the external urinary sphincter significantly reduced pain in male patients. In our study, when the cystoscope went through the bulbar urethra just distal to the external urinary sphincter, we asked the patients to take a deep breath and gave them an explanation of what they saw on the monitor to reduce their pain. Attention on the screen but not totally on the pelvic floor maybe partially explain the lower VAS score and better procedure tolerance in group 1.
Position seems to have a relationship with the VAS score. Soomro and coworkers 9 performed flexible cystoscopy on patients in the supine position and got a satisfactory result in lowing the VAS score; however, no procedures in our trial were performed in te supine position because the bed is specific for the lithotomy position.
This study had some possible limitations. First, the physician is not blinded in all procedures, which may lead to potentially more careful manipulation during one option than in the other. Second, the patient's position during the procedure may influence reported pain scores. The lithotomy position was used in our studies, but the supine position may be more comfortable. Third, because use of intraurethral lidocaine serves essentially as a placebo 7 and produces a higher pain score during injection of the lidocaine before flexible cystoscopy, 12 administering lidocaine gel seems to be unnecessary. In our study, considering the routine and patients' requirement for local anesthesia, intraurethral lidocaine was applied for all patients.
Conclusion
Educating patients by explaining the procedure and showing them what you are doing and seeing in real time may be one of the most important steps in office urology for patient satisfaction.
Disclosure Statement
No competing financial interests exist.