
Abstract
Background and Purpose:
Traditional laparoscopic port placement for upper urinary tract surgery involves camera access via the umbilicus with working ports placed on either side of the camera at various locations. This diamond configuration requires the camera operator to cross hands with the surgeon, resulting in poor ergonomics. A standardized linear port configuration has been used for nearly all transperitoneal urologic surgery at our institution. The purpose of this article is to describe our experience with this simplified approach and its advantages.
Patients and Methods:
A retrospective review was conducted of all laparoscopic cases by a single surgeon from 2000 to June 2009. The linear port configuration includes three ports placed along the ipsilateral pararectal line with the most superior port one fingerbreadth below the costal margin and the inferior port at the level of the umbilicus. A 5-mm camera is used through the most superior port. A low transverse extraction site is typically used, if necessary.
Results:
There were 1264 laparoscopic cases performed using the linear port configuration. Of these, there were 1038 donor/radical/simple and 60 partial nephrectomies, 35 nephroureterectomies, 49 adrenalectomies, 50 pyeloplasties, 20 renal cryoablations, and 12 miscellaneous renal procedures. Of these, 98.2% were performed successfully via this port configuration. Three cases needed an additional port. The intraoperative complication rate was 0.9%, and mean estimated blood loss was 60 mL. There were 20 (1.6%) open conversions: 16 were elective and 4 secondary to complications.
Conclusion:
Simplifying port placement via a linear configuration for both right and left renal and adrenal surgery is feasible, easy to learn, simplifies strategic planning preoperatively, and provides excellent exposure. Using camera access through the superior port allows for direct visualization and minimizes interaction between the camera holder and surgeon's working envelope.
Introduction
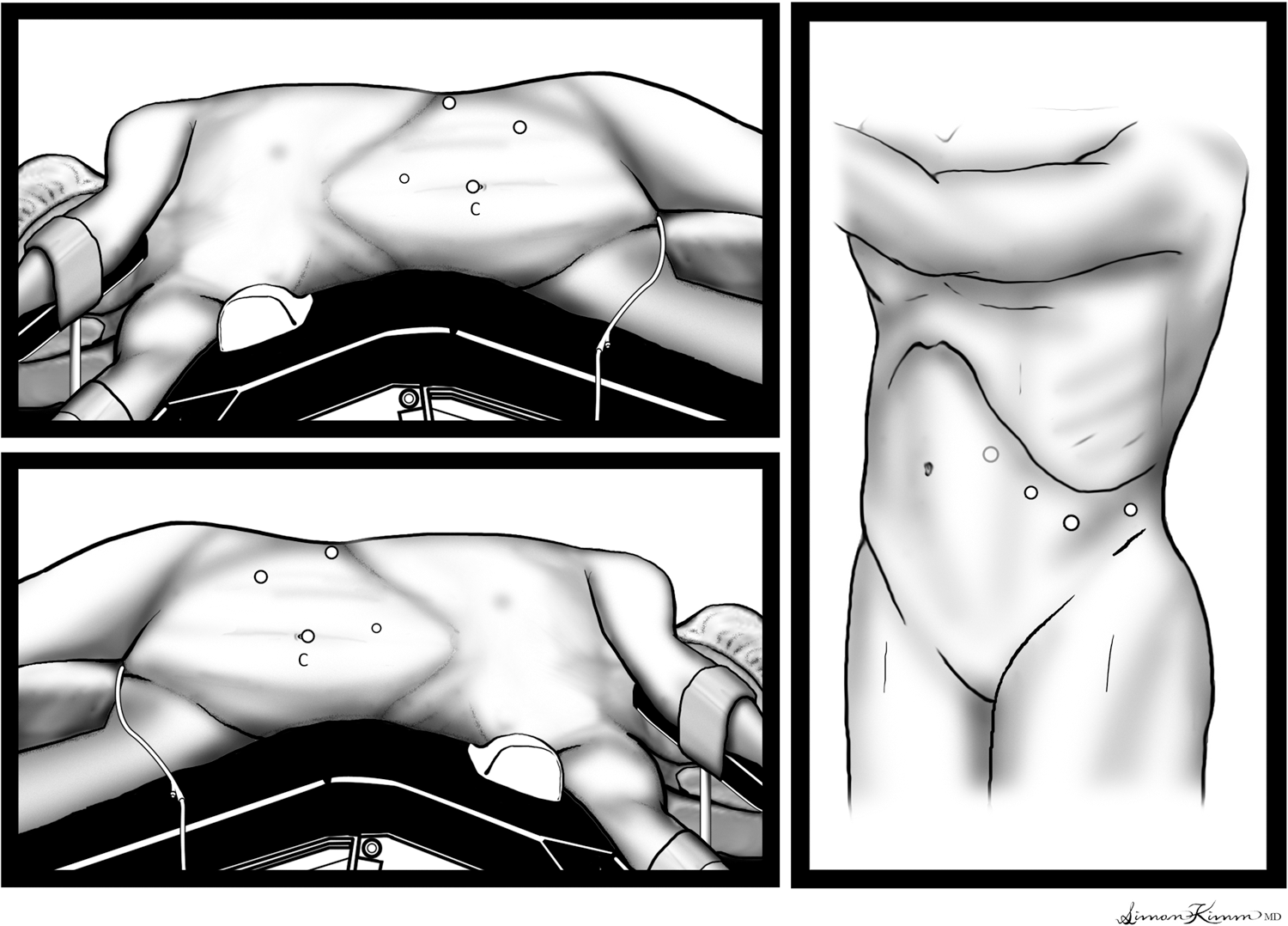
Traditional laparoscopic port configuration for left-sided renal surgery (top left); right-sided renal surgery (bottom left); left adrenal surgery (right). C=camera.
A simplified standardized linear port configuration was originally adopted for laparoscopic donor nephrectomy at our institution in late 2000. The early success with this method has resulted in its continued use for all urologic transperitoneal laparoscopic surgery. The purpose of this article is to describe our experience with this technique and discuss the feasibility and perceived advantages of this approach.
Patients and Methods
All laparoscopic cases from a single surgeon were reviewed from 2000 to June 2009 at our institution. A retrospective chart and database review was performed including all surgeries using the standardized linear port configuration. Data collected included age, sex, surgery, laterality, estimated blood loss (EBL), previous abdominal surgeries, number of ports and sizes used, intraoperative complications, open conversions, and surgical pathology. Current residents were surveyed for their subjective comments comparing this technique with other port placements they have learned. Previous minimally invasive surgery and endourology fellows from UCLA were polled regarding their practice patterns and whether they were still using this technique.
The patient is positioned in the near flank position. The ipsilateral arm is placed across the body in an “airplane,” and the contralateral arm is positioned on an arm board (Fig. 2). Slight table flexion is used, with the break in the table at the level of the umbilicus. The patient is positioned without use of the kidney rest or a beanbag. An axillary roll is placed, and the patient is secured to the bed with 2" cloth tape. Once positioned and the abdomen insufflated, the edge of the rectus muscle and costal margin are marked and provide the landmarks for port positioning.
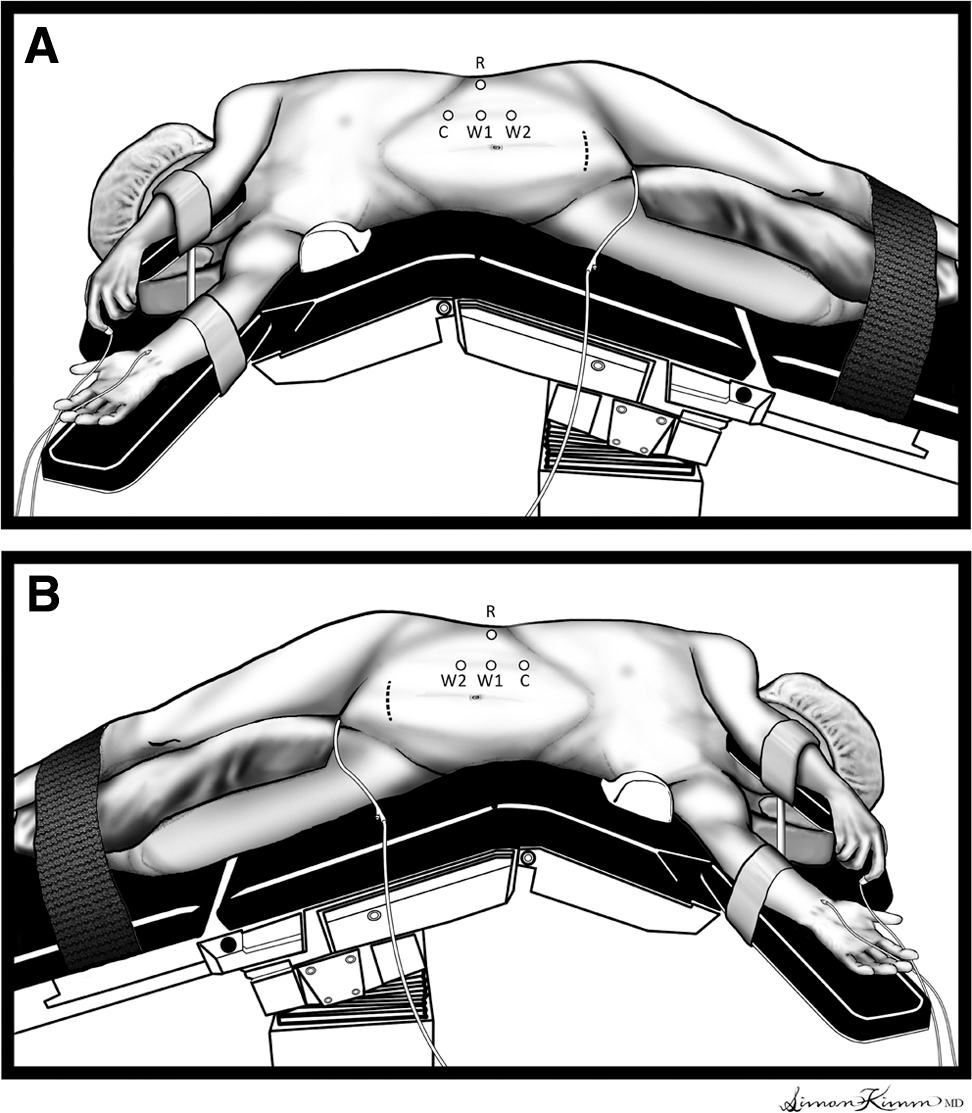
Linear port configuration for left- and right-sided upper tract surgery. C=camera; W1 and W2=working ports; R=retraction.
The linear port technique consists of three trocars placed in a linear fashion along the ipsilateral pararectal line (Fig. 3). The initial and most superior port is placed one fingerbreadth inferior to the costal margin with a visual trocar. The middle and inferior trocars are placed approximately four fingerbreadths apart. The most inferior of the three ports is approximately at the level of the umbilicus, but rarely lower. A 5-mm camera with a 30-degree lens is used through the most superior port throughout the case. A fourth 5-mm port is often placed off the tip of the 11th or 12th rib and used for retraction. An alternative for right-sided cases is a 3-mm locking blunt tip instrument placed in the midline and used for liver retraction. A low transverse, midline, or Gibson incision is used if an extraction site is needed. A 15-mm port is placed through the extraction site incision to place an endovascular stapler and/or entrapment sac (Fig. 3).

Patient positioned in operating room illustrating linear port placement along with a low transverse extraction site with 15-mm port in place.
Results
The series consists of 1264 surgeries, including radical, simple, partial, and donor nephrectomy, nephroureterectomy, adrenalectomy, pyeloplasty, renal cryoablation, and miscellaneous renal procedures. With the exception of donor nephrectomy, each surgery has a near equal distribution of both right and left operations (Table 1). There were 186 radical and simple nephrectomies, 852 donor nephrectomies, 60 partial nephrectomies, 35 nephroureterectomies, 49 adrenalectomies, 50 pyeloplasties, 20 cryoablations, and 12 miscellaneous renal procedures. Of these, 98.2% were performed successfully via this standardized linear port configuration. Mean EBL was 60 mL with a range of zero to 1500 mL (Table 1). If EBL was listed as minimal, it was assigned a value of 50 mL for nephrectomy procedures.
EBL=estimated blood loss.
There were 20 (1.6%) conversions to an open approach: 16 were for elective indications and four secondary to complications. Complications that resulted in conversion included a Veress needle injury to the common iliac artery, trocar injury to the colon, bleeding, and a stapler misfire on an accessory renal artery. Elective conversions were secondary to failure to progress because of difficult dissection, fibrosis, patient anatomy, or tumor fixation. Nine (45%) of 20 patients needing open conversions had previous abdominal operations (P<0.05), and another had previous ipsilateral shockwave lithotripsy and two ureteroscopies. Twelve (0.9%) patients were considered to have intraoperative complications. In addition to the above resulting in open conversion, complications included serosal tear, liver laceration, splenic laceration, and bleeding. There were two aborted cases—one for uncontrolled hypertension in a potential donor and one for ST depression in a patient who had planned to undergo a nephrectomy.
Residents and fellows with experience using traditional port configurations at other hospitals preferred the linear port configuration, reporting that the superior camera placement was more ergonomic when holding the camera and while operating. Intracorporeal knot-tying, however, was subjectively less difficult and frustrating for the trainees when temporarily shifting the camera to the middle, thus allowing the working ports to be further apart. Eight of the 10 fellows trained with this technique responded to an informal poll. All eight still use this port configuration in their practice; four of them teach this technique to urology residents.
Discussion
Triangulation is a general principle of laparoscopic port placement. This traditionally involves the assistant holding the camera within a port placed between two working trocars operated by the surgeon. This positioning is intuitive as it recapitulates human anatomy, with an arm on either side of the point of view. This approach is adapted for laparoscopic nephrectomy using a 10/12-mm camera port at the umbilicus, a second port more superior, also in the midline, and a third port inferior and much more lateral to the camera port. In obese patients, it is recommended to shift this same port configuration laterally. 4 One limitation of this arrangement, however, is the resulting poor ergonomics, with potential for interactions between the assistant holding the camera and the surgeon.
The linear port technique describes placing the camera through the superior port, which not only separates the camera holder and surgeon in space, but also provides the camera with a more direct field of visualization, because it is centered on the renal hilum (Figs. 4 –6). This camera arrangement may represent a paradigm shift for many who have been trained with the camera in the middle. Although both working ports are to one side of the camera, the surgeon's point of view remains intuitive because each port is within close proximity of the camera port.
Standard view via superior port perpendicular to renal hilum.
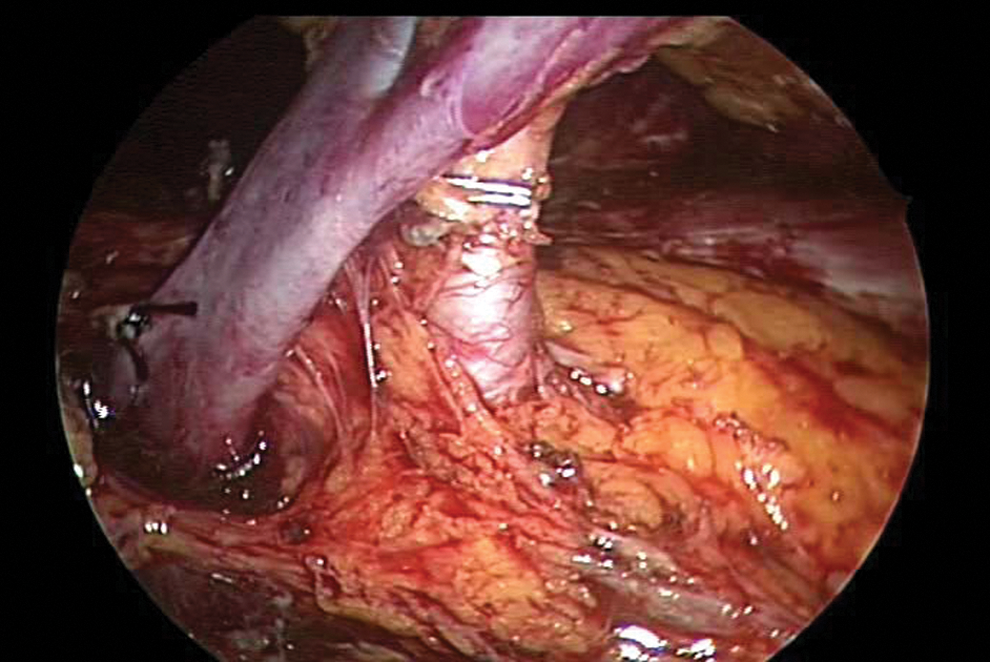
Laparoscopic instrument from inferior port dissecting left adrenal vein. Downward traction on upper pole of kidney exposing underlying muscle. Camera position allows visualization around the superior edge of the renal vein.

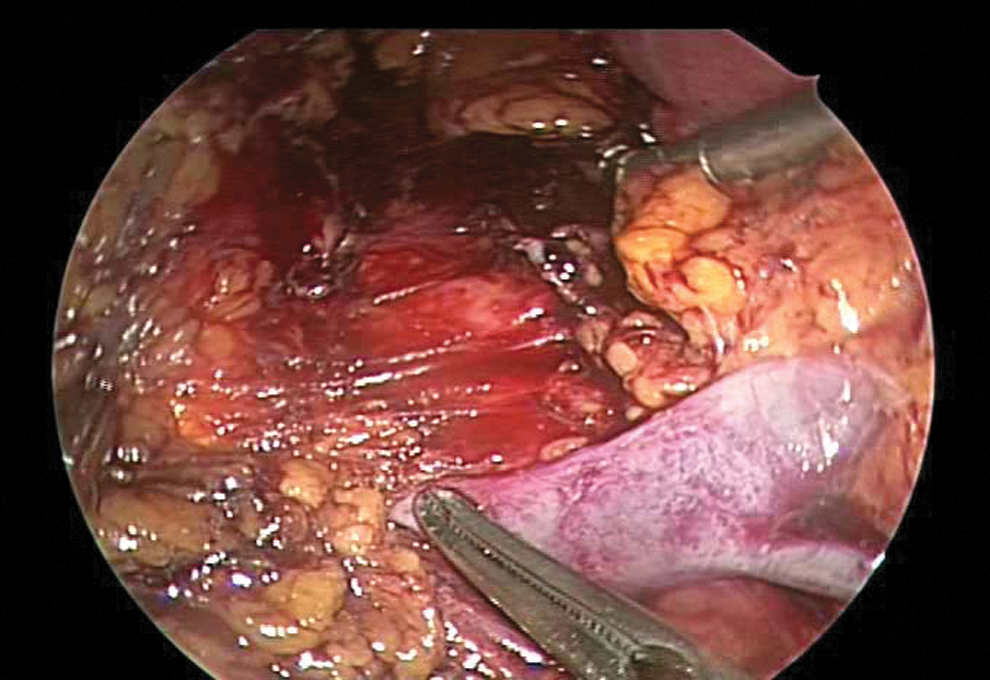
View of inferior edge of the renal vein looking back at the renal artery and lumbar vein. Left hand through middle port elevating kidney and right hand via inferior port dissecting lumbar vein.
It has been shown in a previous model that as the angle between the camera and working instruments increases, a deterioration of performance is witnessed for all skill levels. 7 This is especially true as the angle increases past 90 degrees. With the advent of angled scopes, however, the camera can easily be placed outside of the working field through the superior trocar site and maintain an intuitive perspective for the surgeon.
We use a 30-degree lens that is most often oriented in line with the surgeon's angle of view. For example, for right-sided cases, the lens (through the superior port) is generally aimed from left to right, or placed in the 7 to 11 o'clock position. In our experience, we do still occasionally place the camera temporarily through the middle trocar to facilitate complex intracorporeal suturing (during pyeloplasties and partial nephrectomy renorrhaphy). This allows a greater separation between the instruments, making knot-tying quicker and easier, depending on the experience of the operating surgeon.
Our described standardized linear port arrangement uses the anatomic landmarks of the costal margin and edge of the rectus muscle. The costal margin provides a bony landmark that is less variable than soft tissue structures, such as the umbilicus. These landmarks remain relatively fixed, even in obese patients. Placing the first trocar in relation to the rectus muscle and costal margin leads to a more reliable port configuration with consistent access and visualization. Because this configuration does require each port to be in close proximity, we prefer to use 5-mm trocars and a 5-mm laparoscope. A 10-mm camera, however, could also be used in this location. For most pediatric surgery, we have shifted to using a 3-mm trocar and camera and maintained excellent visualization.
Typically, four 5-mm ports are used when an extraction site is needed for large specimens. In this case, a 12-mm or 15-mm port site can be placed through the planned extraction site incision to facilitate the use of stapling devices and specimen entrapment sacs. Otherwise, a 10-mm or 12-mm trocar will be used as the inferior port, depending on the instruments needed. For example, when performing a laparoscopic partial nephrectomy, a 12-mm port is used at the inferior location to accommodate the Lapra-Ty (Ethicon) device, to facilitate passage of suture needles, for potential use of a stapling device, and extraction of specimen. A larger port is also used when performing endoscopic ultrasound during renal ablative treatment.
There are certain cases when we may deviate slightly from our standard configuration. As mentioned before, laparoscopic adrenal surgery is often performed using three to five ports placed in a row along the subcostal margin (Fig. 1). 6 The linear port arrangement can be used in adrenal surgery. In our experience with adrenalectomy, we initially modified the linear port arrangement by shifting the most inferior port 1 to 2 cm laterally. More recently, we have shifted this port back to the standard linear configuration for left-sided adrenal cases. We continue to shift the inferior port laterally during right-sided adrenalectomy, however, because it appears that this facilitates the dissection at the inferior vena cava/adrenal vein junction. Another modification can be used when approaching a partial nephrectomy on a posterior mass. In this case, we consider moving the most inferior port a few centimeters laterally as well. Alternatively, an additional port could be placed laterally if this proves to be beneficial. A final modification is made for very small pediatric patients, with the linear port arrangement shifted to the midline to allow for a comfortable working distance.
The standardized linear port configuration is easily taught and well accepted by the trainees at our institution. It is thought to be acquired easily, and the residents and fellows can reliably start the surgery without wondering about the ideal location of the ports. These efforts to simplify laparoscopy are believed to be valuable in this setting. It was noticed by several trainees that this configuration is more comfortable in that it allows one to operate with elbows at the side and not spread apart, lessening fatigue. It also allows the surgeon and camera holder to stand next to each other without crossing arms, and there is no need for one to either stand on a stool or sit to avoid each other.
At our institution, this approach was initially used during donor nephrectomy. The benefits of this approach eased the adoption of this port configuration for all upper urinary tract surgery. Although the open conversion rate is higher for nondonor surgeries (3%–5% vs 0.35%) in our series, port configuration was not thought to be a contributing factor. The majority occurred during the initial 5 years and reflected more difficult cases earlier in one's experience. Because there is no comparison or control group using the more traditional port configuration, we cannot determine if there would be a difference. An additional port was placed, however, if thought to facilitate the operation before converting (0.2%). The conversion rates seem to be similar to other large series—between 3.3% and 4.6%. 8 –10 Rowley and Wolf 9 reported a 4.6% conversion from standard laparoscopy, including an intermediate step of converting to hand-assisted laparoscopic surgery, likely lessening their open conversion rate. In our series, we did not incorporate this intermediate step that may theoretically benefit some patients, depending on the surgery and incision needed.
We recognize that this is a description of a simplified standardized port placement that has worked well for a single surgeon operating in a single tertiary referral center. An intrinsic limitation of this study is the lack of a comparison group of patients that underwent traditional port placement. Therefore, we are unable to compare outcomes or state this technique is definitively better. It is also understood that this port configuration and camera placement may represent a paradigm shift; however, we do believe this technique is easily transferrable to other surgeons and institutions. The fellow and chief residents often perform significant portions of the cases at our institution and demonstrate how this linear port configuration can be easily adopted and can obtain excellent visualization and access to the surgical field.
Conclusion
Standardized port placement via a linear configuration for both right and left renal and adrenal surgery is practical, easy to learn, and simplifies strategic planning preoperatively. Using the camera through the most superior port allows for direct visualization, but more importantly, minimizes interference between surgeon and camera holder, and improves ergonomics.
Footnotes
Acknowledgment
We would like to thank Simon Kimm for the generation of Figures 1 and ![]() .
.
Disclosure Statement
No competing financial interests exist.