
Abstract
Purpose:
To determine whether the presence of median lobe (ML) affects perioperative outcomes, positive surgical margin (PSM) rates, and recovery of urinary continence after robot-assisted radical prostatectomy (RARP).
Patients and Methods:
We analyzed 1693 consecutive patients undergoing RARP performed by a single surgeon. Patients were analyzed in two groups based on the presence or not of a ML identified during RARP. Perioperative outcomes, PSM rates, and recovery of urinary continence were compared between the groups. Continence was assessed using validated questionnaires, and it was defined as the use of “no pads” postoperatively.
Results:
A ML was identified in 323 (19%) patients. Both groups had similar estimated blood loss, length of hospital stay, pathologic stage, complication rates, anastomotic leakage rates, overall PSM rates, and PSM rate at the bladder neck. The median overall operative time was slightly greater in patients with ML (80 vs 75 min, P<0.001); however, there was no difference in the operative time when stratifying this result by prostate weight. Continence rates were also similar between patients with and without ML at 1 week (27.8% vs 27%, P=0.870), 4 weeks (42.3% vs 48%, P=0.136), 12 weeks (82.5% vs 86.8%, P=0.107), and 24 weeks (91.5% vs 94.1%, P=0.183) after catheter removal. Finally, the median time to recovery of continence was similar between the groups (median: 5 wks, 95% confidence interval [CI]: 4.41–5.59 vs median: 5 wks, CI 4.66–5.34; log rank test, P=0.113).
Conclusion:
The presence of a ML does not affect outcomes of RARP performed by an experienced surgeon.
Introduction
The surgical technique of RARP is currently standardized, and large series are currently mature enough to show feasibility, safety, and reproducibility of the procedure. 3 In addition, excellent functional and oncologic outcomes have been reported consistently in large RARP series. 2 Nevertheless, the impact of a challenging anatomy, such as the presence of a prostatic median lobe (ML), on RARP outcomes has not yet been fully assessed. The presence of a ML may obscure the plane between the posterior border of the prostate and the bladder neck, making this dissection technically demanding, especially during the initial learning curve. Therefore, positive surgical margin (PSM) rates at the bladder neck and perioperative outcomes, such as estimated blood loss (EBL) and operative time, could be hypothetically affected by the presence of a ML. In addition, the larger bladder neck defect and the potential obstructive bladder dysfunction present in patients with a ML could also potentially affect the recovery of urinary continence after RARP. 4,5
Nevertheless, only a few studies with small sample size and including the surgeons' initial learning curve have analyzed the impact of a ML on RARP outcomes. In this study, we sought to assess the effect of the presence of a ML on perioperative outcomes, PSMs, and recovery of urinary continence after RARP performed by an experienced surgeon.
Patients and Methods
We analyzed 1693 consecutive RARPs performed by a single surgeon (VRP) over a 26-month period. Patients were analyzed in two groups based on the presence or absence of a ML, as identified by the surgeon during RARP. The prospective collection of data was approved by our Institutional Review Board, and written informed consent was provided by all patients.
Table 1 shows patient characteristics.
BMI=body mass index; PSA=prostate-specific antigen; AUA-SS=American Urological Association symptom score.
Urinary continence was evaluated with a self-administrated validated questionnaire (Expanded Prostate Cancer Index Composite), 6 which was administered at 1, 4, 6, 12, and 24 weeks after catheter removal. The definition of continence was based on patients' responses to the questionnaire item number 5: “How many pads or adult diapers per day did you usually use to control leakage during the last 4 weeks?” Continence was defined as the use of “no pads.” The number of weeks postoperatively before recovery of urinary continence was also recorded. Only patients with at least 6 months of follow-up after RARP were included in the analysis of continence rates.
Surgical technique and perioperative management
All operations were performed using a transperitoneal six-port technique, as described previously. 7 –11 A 30-degree down-facing lens was used during the bladder neck dissection. The presence of a ML was an intraoperative diagnosis based on anatomic landmarks and surgical maneuvers, such as contralateral deviation of the balloon when traction applied to the Foley catheter and absence of the posterior bladder neck drop off after incision of the anterior bladder wall. In patients with a circumferential or midline ML, deviation of the balloon catheter may manifest as an elevation of the bladder neck. Large MLs were retracted upward using the fourth arm to locate its junction with the posterior bladder wall.
At this point, the ureteral orifices should be carefully inspected, because they often lie in close proximity to the borders of a large lobe. If the ureteral orifices are not easily identified, intravenous injection of indigo carmine or methylene blue may also be used. The posterior bladder wall was then incised full thickness inferior to the base of the ML. The key is to begin the dissection at the lateral corners of the bladder and then progress medially. The dissection should progress forward under the ML, primarily; once the ML is passed, the dissection should then direct downward toward the vas deferens and seminal vesicles. The retrigonal vertical bladder fibers constitute an important landmark during the posterior bladder neck dissection. Dissection through these fibers leads to identification of the vas deferens and seminal vesicles.
If deemed necessary, bladder neck reconstruction should be performed to bury the ureteral orifice out of the path of the anastomosis in cases of large MLs. Bladder neck reconstruction was performed using a bilateral transverse plication technique as recently described by the authors. 10
As a rule, patients were discharged on postoperative day 1, as long as they were able to eat, drink, and ambulate without intolerable pain or abdominal discomfort.
All patients had cystography on postoperative day 4 or 5 before catheter removal. Up to 200 mL of contrast media was instilled into the bladder with gravity. When a urinary leakage was identified, the Foley catheter was retained for an additional 3 to 7 days.
Statistical analysis
The groups were compared for age, preoperative PSA levels, body mass index, prostate weight, biopsy Gleason score, American Urological Association symptom score (AUA-SS), EBL, operative time, blood transfusion rates, number of nerve-sparing procedures, number of bladder neck reconstruction procedures, number of days with catheter, hospital length of stay (LOS), overall complication rates, tumor volume, pathologic stage, PSM rates, and continence rates. The Student t test or the Mann-Whitney rank sum test was used to compare numeric variables. The chi-square test or the Fisher exact test was used to compare categorical variables. Finally, we used the Kaplan-Meier method and the log-rank test to compare the interval before the return of urinary continence in the two groups. Statistical analysis was performed with the SigmaStat program (Systat, 2006), version 3.5, and statistical significance was set as P<0.05.
Results
A ML was intraoperatively identified in 323 (19%) patients. Patients with ML were slightly older (median 63 vs 60 years, P<0.001), had higher PSA levels (median 5.7 vs 4.7 ng/mL, P<0.001), higher AUA-SS before RARP (10 vs 6, P<0.001) and larger prostates (median weight 64 vs 46 g, P<0.001) when compared with patients without ML (Table 1).
The median EBL, blood transfusion rates, median number of days with urinary catheter, LOS, number of nerve-sparing procedures, cystographic leakage rates, incidence of postoperative urinary retention, and overall complication rates were similar between the groups. The number of bladder neck reconstruction procedures (93.5% vs 65.7%, P<0.001) and the mean overall operative time (80 vs 75 min, P<0.001), however, were higher in patients with ML. Nevertheless, when stratifying the operative time by prostate weight, no difference was found between the groups (<50 g: 75 vs 75 min, P=0.091; 60–69 g: 75 vs 75 min, P=0.104; ≥70 g: 80 vs 80 min; P=0.106) (Table 2).
Complications within 30 days of surgery.
PSM=positive surgical margin.
The two groups had no significant differences in their pathologic stage, frequency of PSMs, and Gleason score of the surgical specimen (Table 2). In the ML group, the overall PSM rate was 10.2% (33/323), and the PSM rates in patients with pT2 and pT3 tumors were 5.4% (14/260) and 30% (19/63), respectively. In the group without ML, the overall PSM rate was 9.7% (169/1730), and the PSM rates in patients with pT2 and pT3 tumors were 6.7% (72/1073) and 32.5% (97/297), respectively. The PSM rate at the bladder neck was also comparable between the groups (1.8% vs 1.4%, P=0.91)
Two hundred and thirty-four patients in the ML group and 1030 patients in the group without ML had at least 6 months of follow-up after RARP and were included in the analysis of continence rates. The continence rates at 1, 4, 6, 12, and 24 weeks after catheter removal in the ML group were 27% and 48%, 69.5%, 86.8%, and 94.1%, respectively. At the same postoperative intervals, the continence rates in the group without ML were 27.8% and 42.3%, 64.1%, 82.5%, and 91.5%, respectively. No statically significant difference was found in the continence rates between the groups at all time points evaluated. Likewise, when stratifying the continence rates by three prostate weight groups, there was no statistically significant difference between patients with and without ML at all postoperative intervals analyzed (Table 3).
Finally, the median interval to recovery of continence was also comparable between patients with (median=5 weeks; 95% confidence interval [CI]: 4.41–5.59) and without ML (median=5 weeks; 95% CI: 4.66–5.34) (log-rank test, P=0.113) in the Kaplan-Meier curves (Fig. 1).
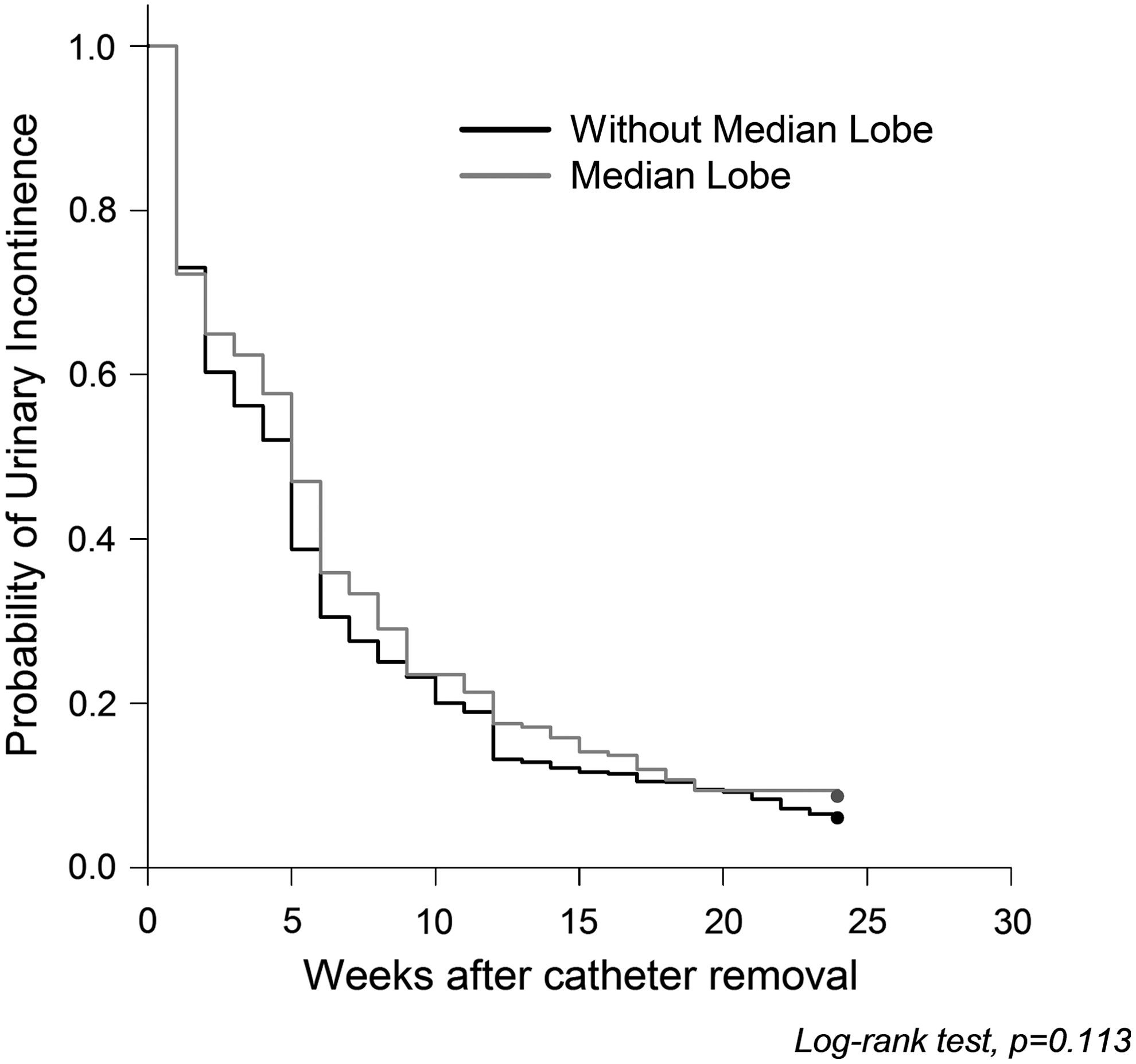
Kaplan-Meier curves showing the probability of urinary incontinence after robot-assisted radical prostatectomy, with and without presence of median lobe (log-rank test, P=0.113).
Discussion
Since the first RARP was described in 2000, 3 the procedure has undergone significant technical refinement, and large series reporting high-quality oncologic and functional outcomes have been consistently published. 2,12 As a result, RARP has become the chosen treatment option for an increasing number of patients with localized prostate cancer, prompting urologic surgeons to face challenging cases (ie, obese patients, large prostates, previous prostatic surgeries, and ML) more frequently in their clinical practice.
The presence of a prostatic ML protruding into the bladder is one of the most common among these anatomic challenges faced during RARP. Because the robotic approach is in an antegrade manner, the identification of the plane between the posterior bladder neck and the prostate is usually challenging in patients with a ML. As result, several adverse outcomes, such as higher PSM rates at the bladder neck, longer operative time, higher EBL and ureteral injury rates, could be potentially maximized by the presence of a ML. In addition, in an attempt to remove the ML completely, a wide excision of the bladder usually produces a larger bladder defect in these patients. Because bladder neck preservation has been associated with better recovery of continence after radical prostatectomy (RP) in some previous studies, 4,13 the existence of a ML could be, therefore, potentially associated with lower continence rates after RARP.
Nevertheless, only a few studies analyzing the effect of a ML on outcomes after RARP and no studies reporting its impact on laparoscopic RP and open RP outcomes are published in the literature (Table 4). 14,15 In addition, these studies were limited by the relatively low experience level of the surgeons, because fewer than 30 RARPs were performed in patients with ML in each series, and small sample size.
Only 29 consecutive patients were included in the control group.
Higher incidence of pT3 (41% vs 14%) tumors in the group without median lobe. Stage-specific positive surgical margin rates not reported.
Statistically significant difference.
Continuous variables presented as median values (mean value are presented in the other studies).
AUA-SS=American Urological Association symptom score; PSA=prostate-specific antigen; EBL=estimated blood loss; PSM=positive surgical margine; LOS=length of stay; ML=median lobe.
Jenkins and associates 14 published the first study on the effect of a ML on RARP outcomes. These authors analyzed 345 RARPs over a 32-month period; a ML was intraoperatively identified in 29 (8%) patients who were compared with 29 patients without ML. The number of surgeons included in the study was not specified. Perioperative parameters and overall complication rates were comparable between the groups. Patients with ML had larger prostates (60 vs 45g, P=0.003) and needed bladder neck reconstruction more frequently during RARP (55% vs 3%, P<0.001). Nevertheless, the overall operative time and the anastomosis time were similar in the two groups. There was trend to higher bladder neck transection time in the median lobe group (34 vs 24 min, P=0.09), but this difference was not statistically significant, most likely because of small sample size (underpowered test).
The overall PSM rates were lower in patients with ML (21% vs 10%); however, this difference also did not reach statistical significance. In addition, the incidence of pT3 tumors was higher in the group without ML (41 vs 14%), which could have influenced the PSM rates. Unfortunately, stage-specific PSM rates were not reported in this series. Finally, the mean interval to recovery of continence was comparable between the groups (183 vs 128 d, P=0.36)
Subsequently, Meeks and colleagues 15 compared perioperative and continence outcomes of 29 (18%) RARPs performed in patients with the presence of a ML with 125 consecutive RARPs in patients without ML. All procedures were performed by a single surgeon. Prostate weight (67 vs 50 g, P<0.01), EBL (464 vs 380 mL, P=0.05) and LOS (2.6 vs 1.7 d, P=0.02) were significantly greater in the ML group. The overall operative time (349 vs 287 min, P=0.005) was also significantly higher in patients with presence of a ML, which was caused by an increased time needed for seminal vesicle (39 vs 30 min, P=0.014) and posterior bladder neck dissection (19 vs 13 min, P=0.007). There was no difference between the groups in PSMs (10 vs 11%, P=0.89) and complication rates, such as urine leaks (22% vs 15%, P=0.25) and bladder neck contractures (7% vs 5%, P=0.12). Finally, the continence rates at 3 months (78% vs 72%, P=0.38) and 6 months (94% vs 78%, P=0.12) after RARP were also equivalent between patients with and without ML (Table 4).
Similarly to these previous studies, in our series, patients with ML were older (median age 63 vs 60 y, P<0.001), had larger prostates (64 vs 46 g, P<0.001), greater preoperative AUA-SS (10 vs 6, P<0.001), and higher number of bladder neck reconstruction procedures (93.5% vs 65.7%, P<0.001). By contrast with the Meeks and coworkers 15 study, however, the EBL (median 100 vs 100 mL, P=0.150) and LOS (median 1 vs 1 d, P=0.572) were similar between the groups in our series. In addition, these authors pointed out that the increased operative times needed for patients with ML in their study were not likely related to the larger prostate size, but it was specifically caused by the presence of the ML. Nevertheless, when stratifying the operative time by prostate weight, no difference was found between the groups in our study (<50 g: 75 vs 75 min, P=0.091; 60–69 g: 75 vs 75 min, P=0.104; ≥70 g: 80 vs 80 min; P=0.106), showing that the slight increase in the operative time in the ML group was actually related to the higher prostate weight.
Similar results were shown in previous series evaluating the influence of prostate weight on RARP outcomes; Link and colleagues 16 analyzed perioperative outcomes in 1847 consecutive RARPs stratified by prostate weight (group 1–less than 30 g, group 2–30 to 49.9 g, group 3–50 to 69.9 g, and group 4 –70 g or greater) and demonstrated longer operative time for patients with larger prostates (mean operative time 2.8 vs 2.8 vs 3 vs 3.2 h, respectively, P<0.01).
Similarly to Jenkins and associates 14 and Meeks and coworkers 15 studies, the overall incidence of complications, (4.6 vs 5.3%, P=0.719) the anastomotic leakage rates (1.5% vs 0.9%, P=0.431), and PSMs (10.2 vs 9.7%, P=0.884) were similar between patients with and without ML in our series. Nevertheless, when considering the entire cohort of patients, the overall complication rates and the incidence of anastomotic leaks were significantly lower in our series when compared with these two previous studies (Table 4). We believe that the disparity in the results can be explained by the unequal surgeons' experience, because in our study, all the procedures were performed by a single surgeon with more than 1500 RARPs performed.
As previously reported, 17,18 the surgeons' experience can significantly affect functional and oncologic outcomes after RP, especially in patients with a challenging anatomy, such as the presence of a ML. The complication rates and the incidence of anastomotic leaks also tend to decrease as the surgeon's experience increases, as recently reported by Coelho and colleagues. 19 Therefore, the limited experience of the surgeons in the previous series evaluating RARP outcomes in patients with ML is a potential confounding factor that could have negatively influenced the results.
Finally, although the incidence of bladder neck reconstruction procedures and the prevalence of lower urinary tract symptoms (LUTS) were higher in patients with ML in our series, the median time to recovery of urinary continence and the overall continence rates at 1, 4, 6, 12, and 24 weeks after catheter removal were similar between the groups. Similar results were shown by Jenkins and associates 14 and Meeks coworkers. 15
The impact of bladder neck sparing and reconstruction on recovery of urinary continence after RP is still unclear; therefore, the lack of difference in the continence rates between the groups in our study is not unexpected. Selli and associates 4 and Deliveliotis and colleagues 13 have shown that bladder neck preservation significantly improves the early recovery of continence after radical retropubic prostatectomy (RRP). Contrarily, Srougi and coworkers 20 concluded that preservation of the bladder neck causes a higher incidence of PSMs (10% vs 0%; P=0.08) and does not improve recovery of urinary continence after RRP (continence rates at 2 d, 2 and 6 mos after catheter removal were 79%, 87%, and 95% with resection, and 67%, 87%, and 97% with bladder neck preservation, respectively; P>0.05 at all intervals analyzed and actually).
With regard to the potential correlation between preoperative LUTS and recovery of urinary continence after RP, the results currently published are also controversial; Lepor and Kaci, 21 analyzing 500 patients who underwent RRP by a single surgeon, showed that the severity of LUTS does not correlate with early return of continence after surgery (odds ratio [OR] 0.992, 95% CI 0.961–1.024, P=0.625). Contrarily, Lee and colleagues 5 prospectively analyzed 107 consecutive RARPs and showed that increased LUTS severity is associated with decreased likelihood of achieving continence at 6 weeks after RARP (OR 0.28, P=0.03).
The strengths of our study included the large single surgeon series and the uses of self-administrated validated questionnaires to evaluate continence postoperatively. The limitations of our study were the limited external validity and the subjective evaluation of the presence of a ML. Finally, although the PSM rates were similar between the groups, long-term oncologil outcomes (biochemical free-survival) were not analyzed because of the short follow-up.
Conclusion
The presence of a ML does not affect perioperative outcomes, PSM rates, and early continence outcomes in patients undergoing RARP performed by an experienced surgeon. There was a slight increase in the operative time in patients with ML that was, however, related to the larger prostate size in this group.
Footnotes
Disclosure Statement
No competing financial interests exist.