
Abstract
Background and Purpose:
Biofilms on the surfaces of urinary catheters are among the pivotal factors for recurrent and persistent infections in urology. Many techniques have been investigated and applied for eradication of these biofilms—but with no full success. The aim of this study was to examine the effect of sustained release medicated varnish, releasing chlorhexidine, on the formation of biofilm on the urinary catheter surface in an in-vitro model.
Materials and Methods:
A batch model was used to test the antibacterial/antibiofilm effect of the sustained release varnish: Catheter pieces coated with sustained release varnishes were placed in bacterial growth medium that was infected with Pseudomonas aeruginosa for 96 hours. Various concentrations of chlorhexidine impregnated in the varnish were tested. After the incubation period, the catheter pieces were assessed for biofilm formation by measuring the optical density, colony-forming units, and using confocal laser scanning microscopy, and electron scanning microscopy.
Results:
Biofilm growth measurement (colony-forming units [CFU]) on the catheter surface coated with the various concentrations of chlorhexidine in sustained released varnish revealed a 94% reduction with 1% chlorhexidine (P<0.0001) and 43% reduction with 0.1% chlorhexidine (P=0.08) coated varnish in comparison with a positive control or the placebo varnish in preventing biofilm growth of P. aeruginosa. These biologic assays were confirmed using confocal and electron microscopy.
Conclusions:
Of the various tested concentrations of sustained release varnishes, the 1% chlorhexidine concentration has demonstrated the superior antibiofilm effect on urinary catheters with P. aeruginosa. Although similar varnishes are used in dentistry, it needs extended research in animals before applying this technology in human trials.
Introduction
CAUTI is the most common nosocomial infection and second most common cause of nosocomial bacteremia. In the majority of cases, CAUTI is asymptomatic, but it can prolong hospitalization and increase hospital expenditure, ranging from $1000 to $2900, and provoke initiation of unnecessary antibiotic regimes, which can lead to multidrug-resistant organisms. CAUTI can progress to pyelonephritis, septicemia, and mortality leading to increases in the institutional death rate 1,3
After a catheter is placed and comes in contact with urine, a conditioning film is formed on the tube, resulting from the deposition of proteins, minerals, polysaccharides, and other host-derived factors in the urine. 4 This resulting surface will provide binding sites for the uropathogens, which initiates colonization, leading to biofilm formation and maturation. This biofilm is the pivotal cause for recurrent and persistent CAUTI.
Various strategies have been attempted to prevent biofilm formation on the urinary catheter surfaces, such as impregnating catheters with gendine, 5 rifampicin and minocycline, 6 nitrofurazone, 7 silver salts, 8 nanosilver particles, 9 triclosan, 10 heparin coating, 11 and drug combinations including chlorhexidine and protamine sulphate, 12 chlorhexidine and triclosan. 13 Surface acoustic waves have also been tested. 14
One means of prevention of biofilm accumulation is by coating the catheter with a varnish that sustains the release of the drug, therefore prolonging the duration of the drug at the target site. Such a technology has been tested in other medicinal fields. 15 Several agents can be incorporated into such a sustained release varnish (SRV). The active agent chosen for this study was chlorhexidine (CHX), which is a quaternary ammonium antiseptic compound that has been tested in medical devices and for urinary tract infection (UTI). 12,13,15
In this study, we tested the SRV technology on the formation of biofilm of Pseudomonas aeruginosa on siliconized latex catheters.
Materials and Methods
Sustained release chlorhexidine varnish
The SRV was formulated according to Beyth and associates. 16 The SRV is composed of ethyl cellulose (5 g), Klucel® EF (4 g), polyethylene glycol 400, and CHX diacetate dissolved in 100 mL of ethanol. Various concentrations of CHX—0.1%, 0.2%, 0.5%, 1%, 2%, 3% and 4% W/V—were incorporated into the SRV and tested.
Bacterial strain
The bacterial strain used was P. aeruginosa wild type (ATCC 27583). Bacteria grown overnight at 37°C in tryptic soy broth (TSB) (Neogen, Lansing, M) were used for the experiments.
Biofilm models
Siliconized latex catheters (Bard Limited, UK) were cut into small pieces of 4 mm in length. To calculate the accurate amount of SRV applied on the catheter, each of these catheter pieces was preweighed and then coated with the SRV, dried, and then reweighed (Figs. 1A, 1B). Positive controls were catheter pieces without any varnish but incubated with P. aeruginosa, and negative controls were catheter pieces incubated only in TSB without P. aeruginosa. Catheter pieces were also applied with a placebo varnish for comparison.

All samples were placed in an Erlenmeyer flask containing TSB, and a suspension of P. aeruginosa grown overnight was added and incubated for 48 hours at 37°C. After incubation, the catheter pieces were removed and washed gently with phosphate buffered saline (PBS) three times to remove loosely adhered bacteria. Next, the catheter pieces were placed in 2 mL of PBS and sonicated in a water bath (Elma Transsonic T 460, Singen, Germany). Optical density (OD) of the postsonicated effluent of the catheter pieces was measured using the UV/Visible Spectrophotometer (Camspec, Cambridge, UK) at a wavelength of 600 nm. Next, the sonicated fluid was serially diluted and plated on brain heart infusion agar using a quad loop spreader. After 24 hours of incubation at 37°C, the numbers of colony-forming units (CFU) were counted using a magnifying viewer (New Brunswick Scientific, Edison, NJ). All experiments were repeated four times in duplicated samples in each set of the experiments.
Confocal laser scanning microscope
Biofilm formations on the catheter samples were examined using a confocal laser scanning microscope (CLSM). The catheter pieces were prepared as described above and the biofilm was fixed with 4% freshly prepared formaldehyde for 10 minutes and then rewashed with double distilled water. Next, the samples were stained with propidium iodide (Sigma, Steinheim, Germany) at 1 in 1000 dilution and left for 30 minutes in the dark, washed again with double distilled water, after which the samples were studied under CLSM (Olympus FV 300, Tokyo, Japan). The fluorescence was observed by using a 10X/0.5 lens (Olympus). The green fluorescent light was excited with a helium-neon laser at 543 nm excitation line. The autofluorescence of the samples was set to background levels. The specimen was examined in at least five different areas and repeated in multiple experiments. 17
Scanning electron microscope (SEM)
The catheter samples prepared as described above were washed with PBS and then fixed with 2.5% freshly prepared glutaraldehyde, kept for 24 hours at 4°C and then rewashed in PBS. The samples were dehydrated through a graded series of ethanol solutions and were mounted on stubs after air drying and introduced into a sputter coater (Polaron, CS7640, Hertfordshire, UK) for a coating process with a fine layer of gold-palladium (10 nm). The samples were examined under a Sirion high resolution SEM (FEI, Eindhoven, The Netherlands). Visual inspections were performed at 1500 and 5000 magnification.
Statistical analysis
Statistical analysis was performed using the Student two-tailed paired t test. A P value <0.05 was considered as statistically significant.
Results
The influence of the SRV containing CHX on biofilm formation of P. aeruginosa on catheter pieces was tested by means of CFU, OD, CLSM, and SEM as follows:
Bacterial analysis
Bacterial analysis of the biofilm using the OD and CFU techniques demonstrated a dose dependent response. As the concentration of CHX in the SRV was increased, the amount of total bacteria in the biofilm decreased. The reduction in bacterial counts with 3% CHX in the SRV was 74.5%±12.32% compared with control (P<0.0001) while 0.1% of CHX in the SRV decreased biofilm formation only by 12.3%±24.3% (P=0.44) (Fig. 2A).
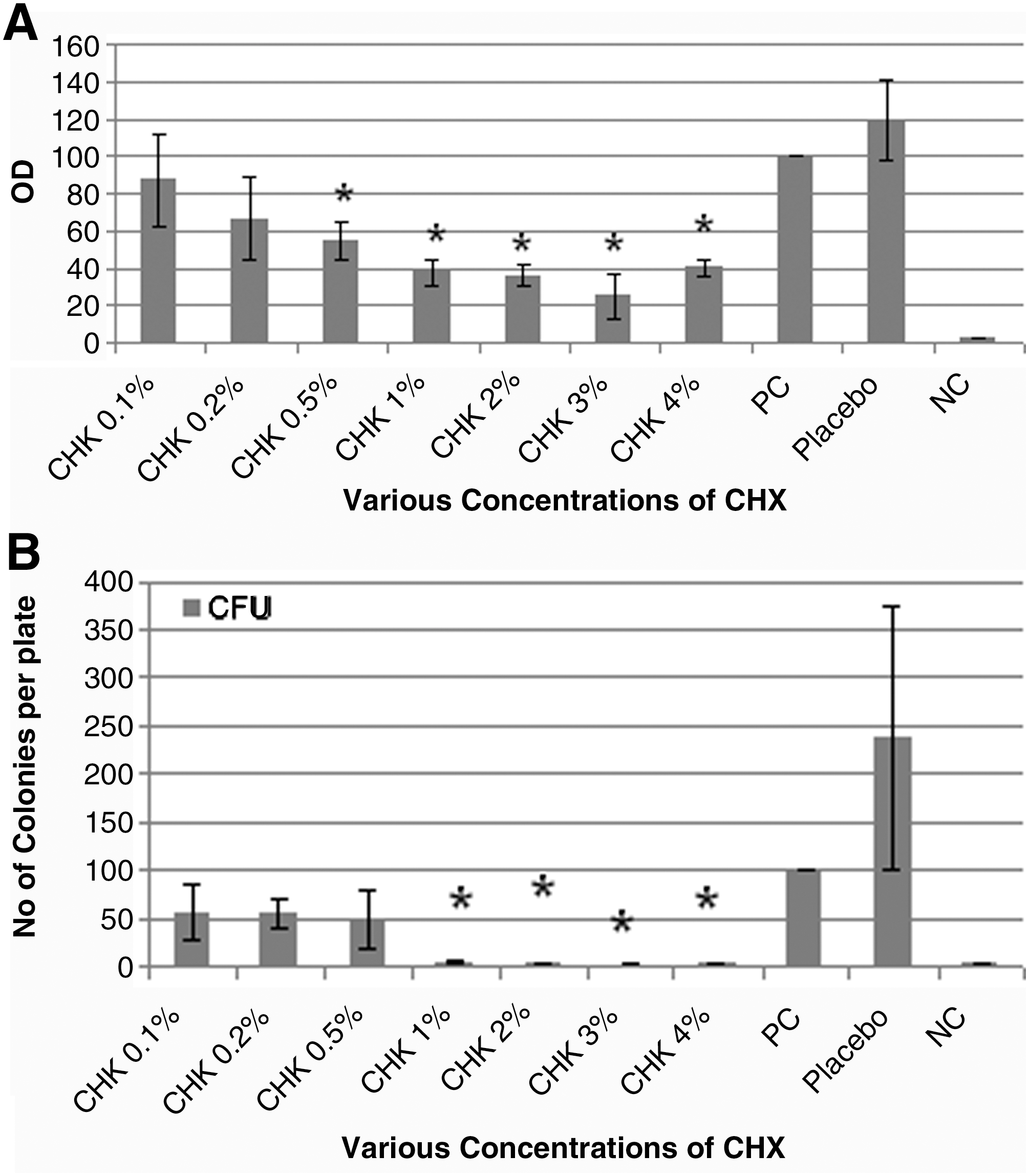
A similar dose dependent response was also observed in the CFU method (Fig. 2B). The amount of live bacteria accumulating on the catheter samples pretreated with SRV of 1% CHX decreased by 94.8%±3.08% (P<0.0001) while 0.1% CHX SRV decreased bacterial counts by 43%±28.75% (P=0.08) (Fig. 2B).
CLSM
The total biofilm mass was measured as the signal intensity noted from the surface of the catheter. The negative control of the catheter had no fluorescent emission after microscopic adjustments (Fig. 3A). A very low signal was observed with the SRV of 1% CHX (Fig. 3B), while a strong signal intensity of the attached biofilm of the positive control was demonstrated (Fig. 3C).
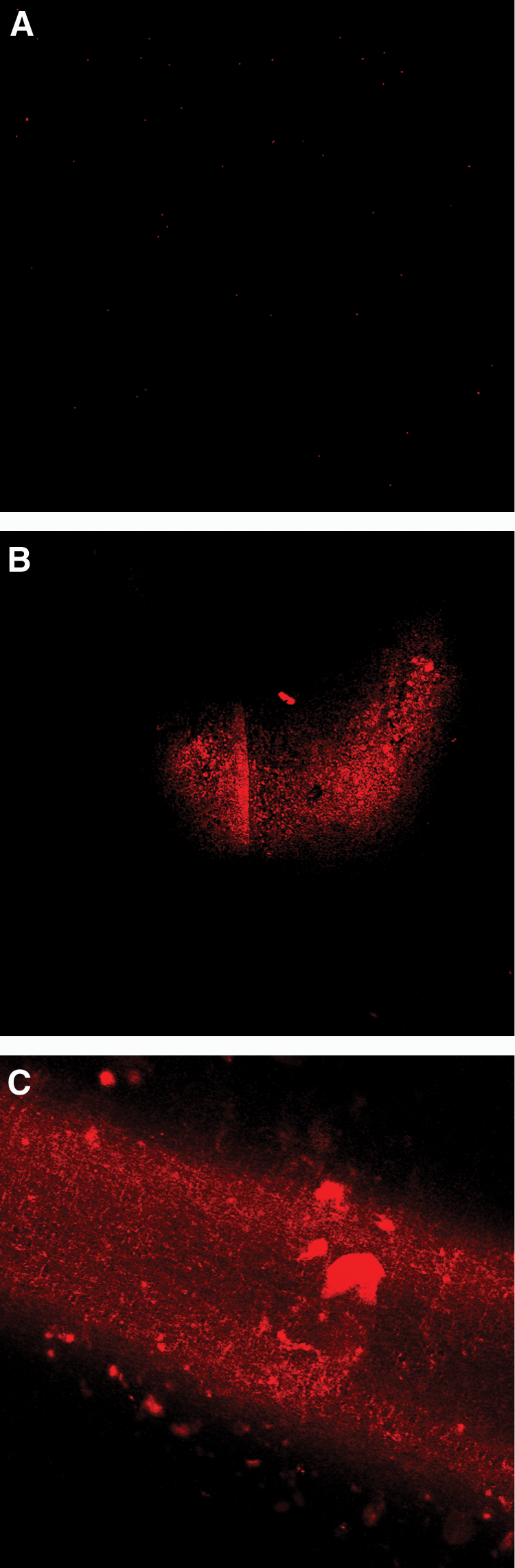
Confocal laser scanning microscope pictures of biofilm formed on a catheter:
SEM
The surface topography of a normal catheter has crevices, pits, and a rugged nature with particles of the material (Fig. 4A). The catheter piece that was incubated without organisms—ie, negative control—showed a normal catheter but coated with conditioning film (Fig. 4B). P. aeruginosa embedded in the extracellular matrix could be seen after incubation with the bacteria (Fig. 4C), whereas the catheter coated with the SRV of CHX 1% was free from bacterial colonization (Fig. 4D).
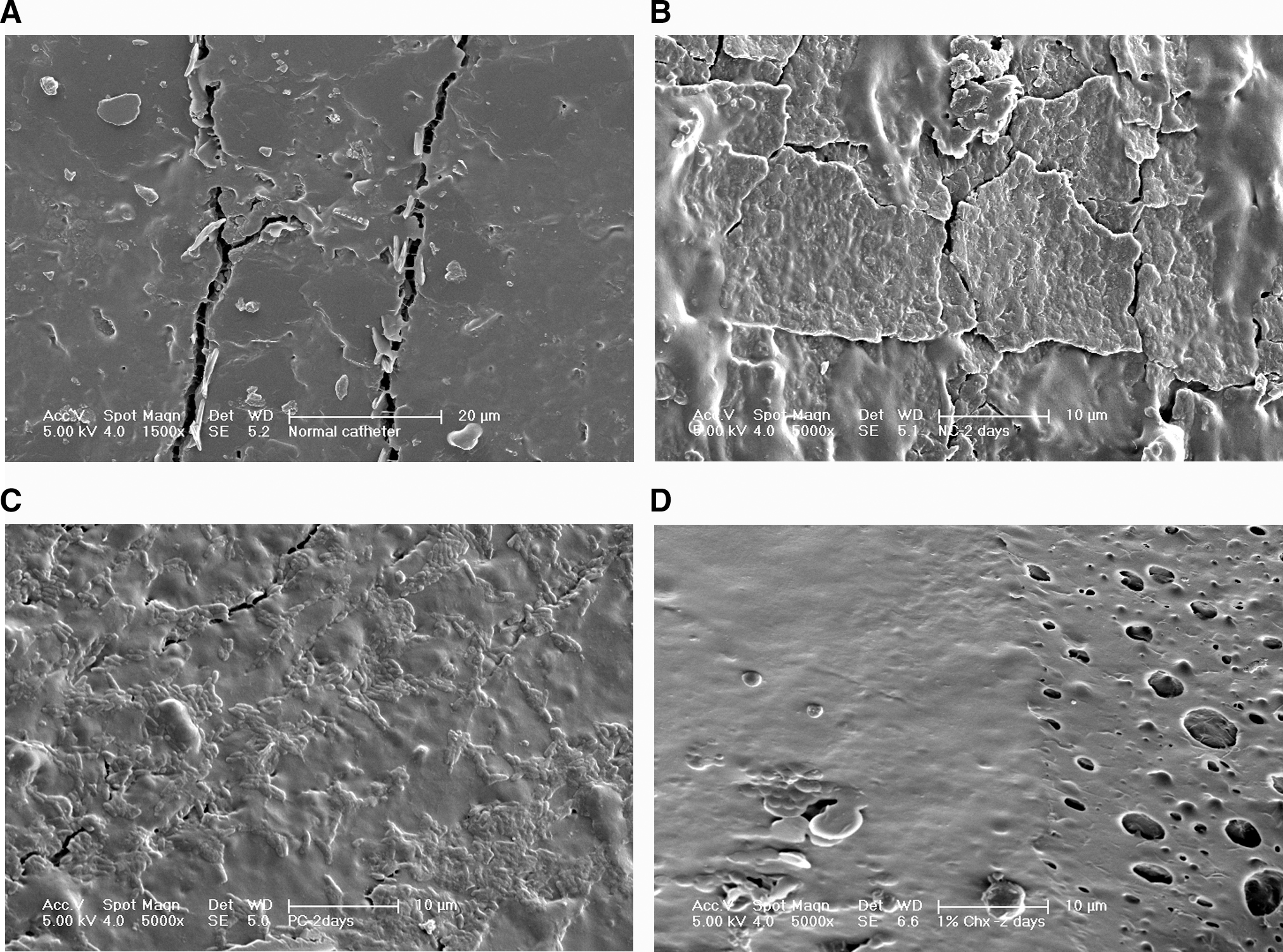
Scanning electron microscope images of catheter surfaces.
Discussion
Bacterial accumulation on indwelling urinary catheters is a major clinical problem in urology. 1,2 Colonization by bacteria imparts serious problems, such as necessitating removal of the catheter, replacement of the catheter, and treatment of the infection, usually with antibiotics. Countering the initiation of these biofilms is an important step in the prevention of CAUTI.
Most episodes of infection follow extraluminal ascent of bacteria, although both the internal and the external surfaces of the catheter are susceptible to contamination. The process begins with bacterial access into the urinary tract; the next step is attachment and colonization onto the catheter surface. 18 Initially, the bacteria form a monolayer on the surface and then grow into microcolonies that mature into biofilm embedded in an exopolysaccharide matrix, which protects the embedded bacteria from the host's natural defense system as well as from antimicrobial therapy.
P. aeruginosa has been identified as one of the important causative agents in infection of the urinary tract especially in patients with indwelling catheters. 19 P. aeruginosa is noted for its ability to produce a persistent biofilm on the surface of catheters.
Bacteria immobilized in a biofilm are unique in nature because of lower susceptibility to antibacterial agents than planktonic bacteria. 20 This effect is mediated by a densely populated immobilized ecosystem, coated with exopolysaccharides that retard the diffusion rate of antibacterial agents into the deep layers of the biofilm. 21
Applying SRV adjacent to the biofilm coating the catheter serves as reservoir for controlled release of medication to the biofilm. Maintaining locally high dosages of the drug at the infected site will allow better penetration into the biofilm. The use of sustained release delivery systems such as the SRV allows a graduated release of the drug and therefore better antibacterial efficacy against the bacteria immobilized in the biofilm. 15,22
Many techniques have been suggested to affect the P. aeruginosa biofilm on catheters. 23 –28 The SRV technology has numerous pharmacologic advantages that stem from the ability to control the release of the drug from the matrix of the SRV, prolong duration of the drug at the desired site, better penetration into the biofilm layers, and reduced systemic and local side effects because the amounts of drug released are low. We tested the effect of a coating of SRV containing CHX on biofilm formation on catheters. This technology using a similar SRV of CHX, or with other active agents, has been applied in in-vitro experiments and has also proven effective in human dental applications. 15 This study is the first attempt to use this technology in the urologic field, on urinary catheters, to prevent biofilm formation on the catheter. Using an external coating on the catheter rather than impregnating an agent in the polymeric matrix of the catheter will not affect the properties of the catheter before and after the release of the drug. In addition, better control of the release rate can be achieved when coating with SRV, as the release rate can be controlled by modifying the pharmaceutical formulation.
The drug we chose was CHX because it is known for it broad antiseptic properties. 29 The CHX in our SRV formulation is not bound to the polymeric matrix but is entrapped between the polymeric chains. Therefore, the release kinetics of the drug are dependent on its diffusion rate and on the pharmaceutical release controllers.
Our results indicate that the CHX varnish reduced the formation of biofilm mass on the surface of urinary catheters compared with the control. The antibacterial effect of the CHX varnish found is dose dependent—ie, the lower CHX concentrations, 0.1% or 0.2%, did not affect biomass formation, whereas 0.5% CHX and above reduced the biofilm. Confirmation of the results using SEM and CLSM also indicates the working potential of this SRV in biofilm prevention on the urinary catheter surface.
Although the antibiofilm effect is demonstrated at SRV formulations of higher dosages of CHX, it still remains to examine whether this is a simple antibiofilm effect or a mixed antibiofilm/antibacterial effect. It has been reported that cationic agents such as CHX may kill bacteria, but on the other hand, because of their positive charge, they initiate adsorption of cells to surfaces.
Biofilm formation is a multistep process in which, at the initial stages, the bacteria dock onto the conditioning film that later will propagate into a massive biofilm. 30,31 In this study we tested the biologic efficacy of the CHX—SRV as a novel means in the prevention of the initiation of the first step in biofilm formation. Similar formulations have shown a much longer effect in other human organs, 15 but it still remains to be proven also in CAUTI. It is also conceivable that other active drugs, such as triclosan, silver, gentian violet, heparin, or protamine sulphate, can be incorporated into the SRV and tested as well.
Footnotes
Acknowledgments
To all who had helped in conducting the experiments, such as Ofir Lidor, Dr. Mark Feldman, Dr. Guy Hidas, Dr. Mark Tahrish (Department of Confocal Microscopy, Hadassah Hebrew University Hospital, Ein Kerem, Jerusalem, Israel) and Evagenia Blyvas (The Unit for Nanoscopic Characterization, The Hebrew University of Jerusalem, E. Safra Campus Givat Ram, Jerusalem, Israel).
Disclosure Statement
No competing financial interests exist.