
Abstract
Purpose:
The aim of this study is to compare the perioperative outcomes after transumbilical laparoendoscopic single-site (LESS) radical nephrectomy (LESS-RN) performed by a surgeon during his learning curve of this novel procedure with the outcomes after standard laparoscopic radical nephrectomy (LRN) for patients with a solitary renal tumor. Using this information, we examined whether LESS exhibits any objective advantages over standard laparoscopy.
Patients and Methods:
Twenty patients who underwent LESS-RN for a solitary cT1N0M0 renal mass (group 1) were matched and compared with 33 patients who underwent standard LRN (group 2) for tumors of similar sizes. Patient and surgical data, pathologic outcomes, and follow-up information, including patient responses regarding cosmetic satisfaction, were analyzed.
Results:
The minimum duration of follow-up was 6 months for both groups. Patients in group 1 had significantly (P<0.05) quicker recoveries of bowel function, shorter postoperative analgesic time, and lower pain scores during their hospital stay. At the time of the last follow-up, all patients remained symptom free, and no evidence of recurrence was detected. Compared with that of standard LRN patients, LESS-RN patients exhibited better cosmetic satisfaction scores postoperatively at least to 6 months (P=0.013).
Conclusions:
Transumbilical LESS-RN is a feasible, safe, and efficacious procedure with favorable perioperative outcomes that results in significantly improved control of postoperative pain, more rapid recovery of bowel function, and increased cosmetic satisfaction. Additional research, including randomized controlled trials and long-term follow-ups, however, will be needed to draw solid conclusions regarding the relative efficacy of this procedure compared with standard approaches.
Introduction
We present a case-control study comparing transumbilical LESS radical nephrectomies (LESS-RNs) and conventional laparoscopies with respect to perioperative outcomes and follow-up data.
Patients and Methods
The Institutional Ethics Committee of Changhai Hospital approved the use of the data maintained in our institutional patient registry. This was a retrospective, case-control study comparing patients undergoing either LESS-RN or standard transperitoneal LRN beginning with our initial transperitoneal LRN case in December 2007. Before the end of 2007, the retroperitoneal approach of LRN was the surgeon's preferred surgical procedure. Between December 2007 and May 2011, a total of 110 LRN procedures were performed by a single surgeon (LHW) (Fig. 1).
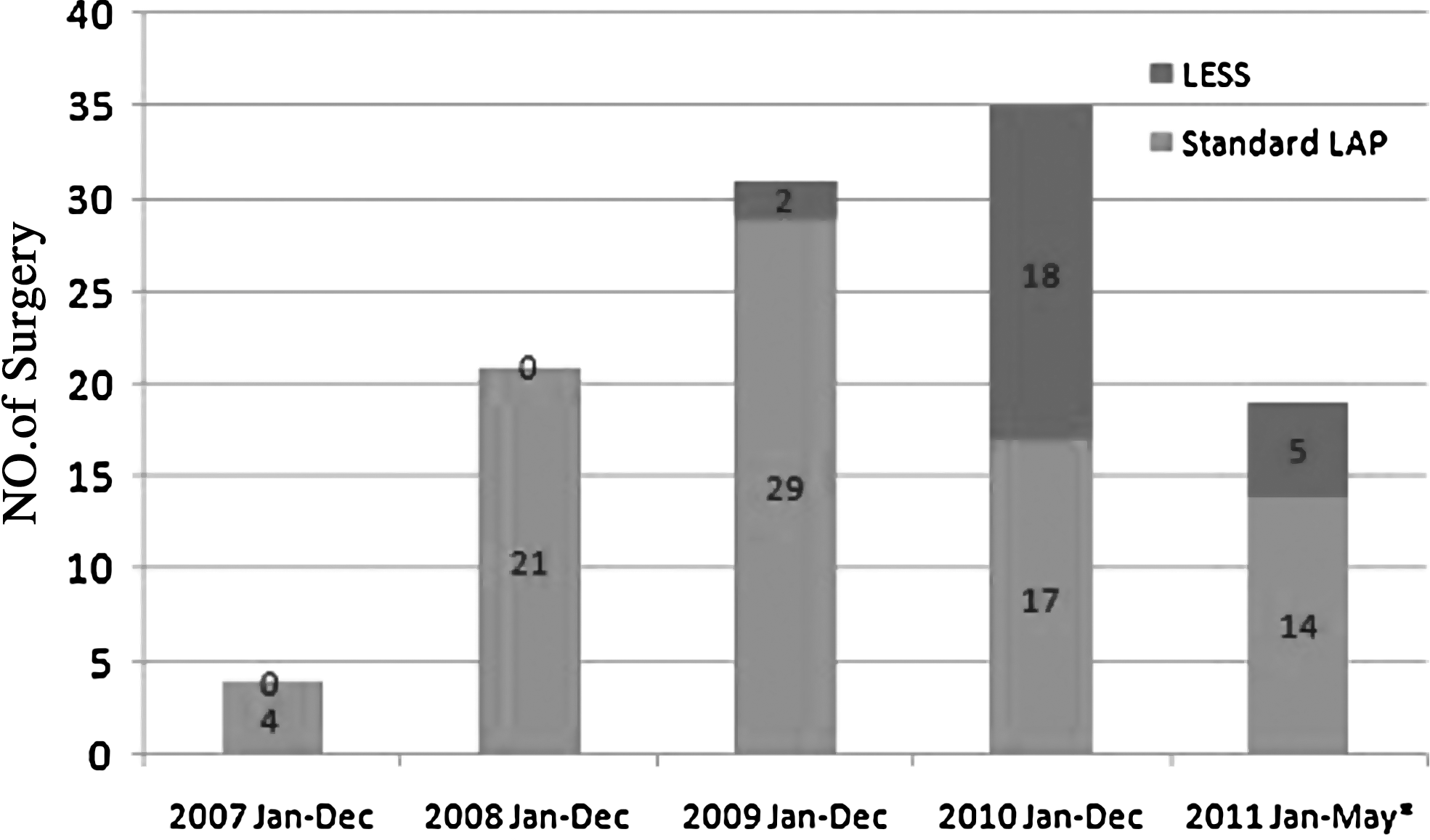
Yearly comparison of standard transperitoneal laparoscopic radical nephrectomy vs laparoendoscopic single-site radical nephrectomy.
RN was indicated for enhancing renal masses that were not amenable to nephron-sparing surgery by either laparoscopic or open surgery. Additional indications included the patients' own decision to undergo a radical procedure.
We identified 85 patients who were treated by standard LRN and 25 patients treated by LESS-RN for a single unilateral renal mass. The perioperative and 6-month follow-up outcomes of the LESS-RN group (n=20) were compared with the outcomes from 33 matched patients who were treated with standard LRN between December 2007 and December 2010. Patients were matched retrospectively on the basis of patient age, body mass index (BMI), affected side, tumor size and location, and surgical indication (cT1 stage). Patients were treated with either standard LRN or LESS-RN according to the surgeon's clinical judgment, not at random. Criteria for LESS-RN included a relatively small renal mass (cT1 stage) with a relatively low BMI (<30) and no previous abdominal surgery. Patients were informed that additional incisions or open surgical conversions might be warranted during the procedure.
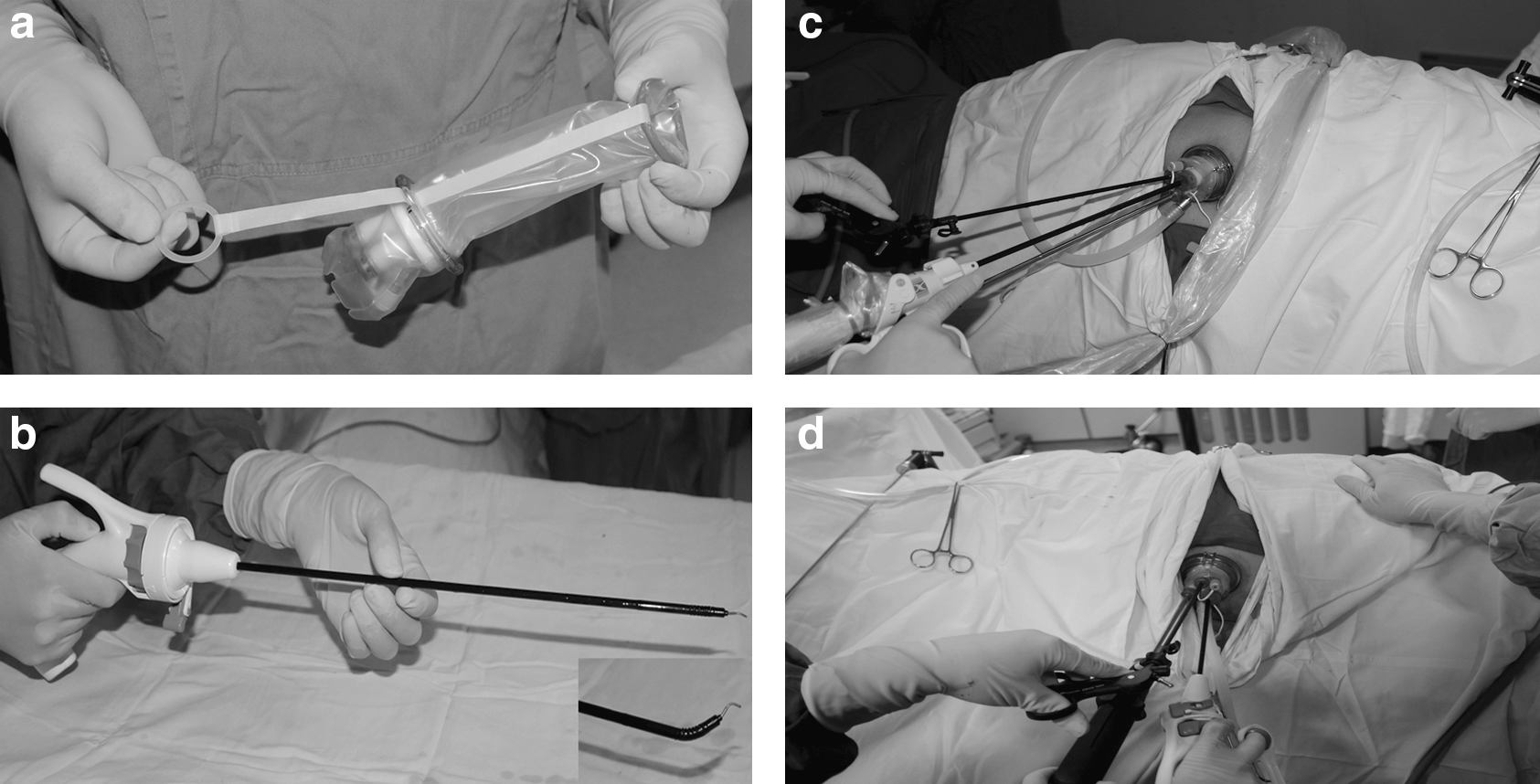
Transumbilical LESS-RNs were performed using a multichannel TriPort™ (Advanced Surgical Concepts, Wicklow, Ireland) through a 2- to 3-cm skin incision. An ancillary 5-mm trocar was applied to facilitate retraction with a grasper during our first two procedures via a skin incision in the anterior axillary line below the 12th rib. LESS procedures were conducted according to standardized techniques using a combination of articulating instruments, including the Autonomy Laparo-angle™ (Cambridge Endo, Framington, MA), and standard laparoscopic instruments (Fig. 2). For conventional laparoscopy, the following three to four trocars were used as necessary: One 12-mm trocar near the respective linea pararectalis at the umbilicus level, one 12-mm trocar approximately 2 cm below the costal margin at the midclavicular line, one 12-mm trocar 2 cm above the crista iliaca in the anterior axillary line, and one 5-mm subcostal trocar in the anterior axillary line for retraction.
The renal artery, vein, and ureter were sequentially divided with 5-mm Hem-o-lok clips (Weck, Research Triangle Park, NC) and titanium clips (Olympus, Tokyo, Japan). The intact specimen was placed into an EndoCatch bag (Covidien, Norwalk, CT) and extracted. Adrenalectomy was not performed routinely for cT1 tumors; this was only conducted in the 10 patients with factors leading to suspicions of metastatic disease (2 patients in group 1 and 8 patients in group 2). Renal hilus lymphadenectomy was performed when intraoperative inspections revealed suspicious nodal enlargements (4 patients in group 1 and 10 patients in group 2).
When necessary, patients received continuous intravenous analgesics for a maximum of 48 hours. The pain scale was self-administered on postoperative days 0 (6 hours after surgery), 1, and 2, and on the day of discharge. Patients were regularly followed up with the appropriate studies at 3, 6, and 12 months after surgery, and once annually thereafter. Cancer patients were evaluated using CT scans at 6 and 12 months after surgery and then every 12 months if there was no evidence of recurrence or metastasis.
Patient demographics and perioperative data, including operative time, estimated blood loss, transfusion requirements, percent decreases from preoperative serum levels of hemoglobin, surgical conversions, time off of oral intake, postoperative pain assessments, postoperative hospitalization length, intra- and postoperative complications, pathologic results, cost of surgical instruments, and short to intermediate-term follow-up data were recorded. Complications were classified according to the Clavien grading system. 3
For pain and cosmetic satisfaction assessments, the visual analog scale (VAS) was used, which ranges from 0 (no pain and completely unsatisfied, respectively) to 10 (excruciating pain and fully satisfied, respectively). The highest pain score was included for analysis. For cosmetic satisfaction assessments, all patients were followed up by a mailed questionnaire that was self-administered no sooner than 6 months postoperatively.
The two groups were analyzed using chi-square and Mann-Whitney tests for categorical and continuous variables, respectively. Statistical significance was set at P<0.05, and all P values were two-tailed. Statistical analyses were performed using SPSS v. 16.0 (SPSS, Inc, Chicago, IL).
Results
Patient demographics and tumor characteristics are summarized in Table 1. No statistically significant (P>0.05) differences were noted between the two groups. Surgical and pathologic data are shown in Table 2. LESS-RN procedures were well tolerated and resulted in significant decreases in postoperative analgesic time, visual analog pain scales, and time to oral intake. The cost of the surgical instruments for the LESS-RN procedure was about $1176, but the instruments for the standard LRN procedure cost only about $392.
SD=standard deviation; LESS=laparoendoscopic single-site; LAP=laparoscopy; BMI=body mass index; ASA=American Society of anesthesiologists.
SD=standard deviation; LESS laparoendoscopic single-site; LAP=laparoscopy; OT operative time; EBL estimated blood loss; Hgb hemoglobin; VAS=visual analogue scale; LOS=length of stay; RCC=renal-cell carcinoma.
In group 1, a 5-mm ancillary trocar was inserted during the first two cases of LESS-RN for tissue retraction. In one case, a conversion from LESS to standard laparoscopy occurred because of an uncontrollable hemorrhage from an inadvertent injury of an anomalous renal artery branching from the celiac trunk. The converted patient received a transfusion intraoperatively and transient pyrexia developed (Clavien grade I) postoperatively. Spontaneous pneumothorax developed during the induction of anesthesia in one patient with chronic obstructive pulmonary disease; this was managed by thoracic closed drainage. Because of these complications, this patient was kept in the hospital for 12 days after the operation. In group 2, one patient had an intraoperative hemorrhage and received a transfusion, but surgical conversion was not needed. Postoperative bleeding developed in two patients; this was managed conservatively by transfusion (Clavien grade II).
Surgical margins were negative in both groups. No patients exhibited local lymph node metastases or direct invasions of the ipsilateral adrenal gland. Of the 20 patients in group 1, 19 demonstrated pathologic renal clear-cell carcinomas, and the last patient had a sarcomatoid carcinoma with a stage distribution of 7 T1a and 13 T1b. In group 2, there were 29 patients with renal-cell carcinomas (27 ccRCC and 2 chRCC), one patient with oncocytoma, one patient with angiomyolipoma (AML), and two patients with nephroblastoma with stage distributions of 19 T1a and 14 T1b.
The mean follow-up duration for the LESS-RN group and the standard LRN group were 9±4.01 (range 6–18) and 18.2±6.36 (range 6–24) months, respectively. During this period, no local recurrences or metastases were observed. For the cosmetic satisfaction investigation, the response rate of the mailed questionnaires for groups 1 and 2 was 94.7% (18/19) and 81.8% (27/33), respectively. Nine patients (three patients in group 1 and six patients in group 2) with a mean age of 71.7 years expressed “negligible attention to the cosmetic influence of the skin scar.” The mean cosmetic satisfaction score was significantly higher in the LESS group than in the group treated by standard LRN (9.3±0.61 vs 8.4±1.03, P=0.013) (Fig. 3).
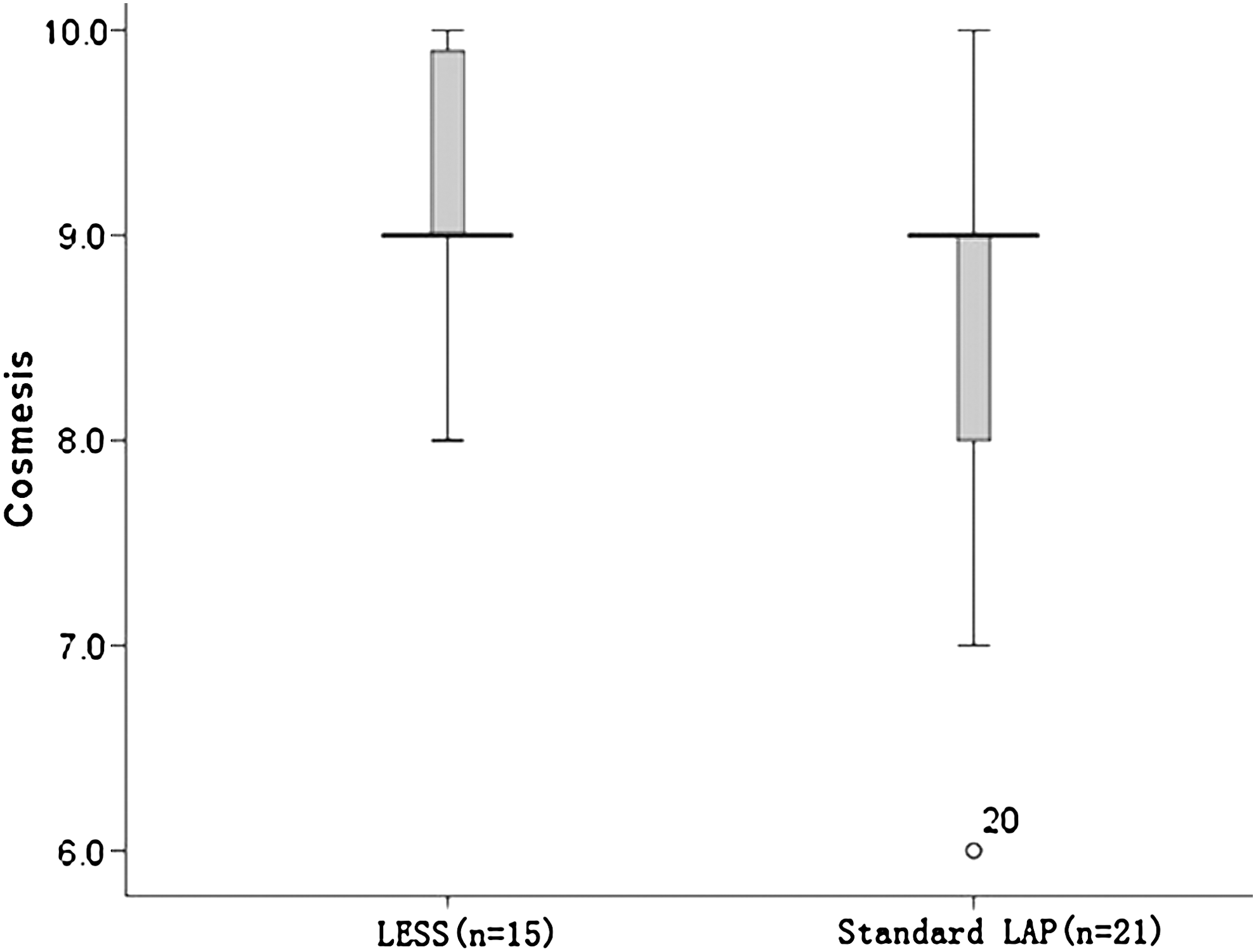
Comparison of the cosmetic satisfaction scores between the two groups. LESS=laparoendoscopic single-site; LAP=laparoscopy.
Discussion
The pioneering laparoscopic nephrectomy was completed successfully in 405 minutes in an 85-year-old woman with 3-cm solid renal mass in 1990. 4 Since then, LRN had been accepted gradually as a viable surgical option with a lower morbidity and equivalent tumor control rates for T1–T2 renal tumors compared with open surgery. 5 –7 The LESS procedure, which is part of an effort to continually improve postoperative pain control and convalescence, has shown a remarkable increase in use recently. 8 Initial case reports and small noncontrolled studies from different institutions have indicated that RN using LESS is a feasible alternative to conventional laparoscopy. 9 There is lack of adequate studies, however, to elucidate the true benefits of LESS-RN compared with conventional laparoscopies.
In the present study, not only the surgical feasibility, safety, and the perioperative outcomes, but also the pain, recovery, and patient-reported cosmetic satisfaction scores were evaluated to assess the advantages of performing LESS-RN in this patient group. This study clearly demonstrated the advantages of LESS-RN. For example, LESS-RN results in reduced need for postoperative analgesia, faster postoperative recovery of bowel function, and better cosmetic satisfaction.
Three critical issues, however, must be emphasized in our surgical practice; namely, the selection of relatively small kidney tumors (cT1 stage), a nonmuscle-splitting incision, and the avoidance of morcellation. The underlying rationale is that the removal of renal tumors that are too large would necessitate larger incisions that would consequently negate the advantages of LESS-RN. In addition, we believe that nonmuscle-splitting incisions represent one of the key factors for ensuring low levels of postoperative pain. Using morcellation, reduced postoperative narcotic requirements and shorter lengths of stay were reported. 10 The adverse effects of morcellation, however, including potentially compromising pathologic assessments and allowing for tumor seeding in the case of sac rupture, do not justify using this method when treating cancer. In those cases, the most reasonable course of action appears to be intact specimen extraction.
Many studies have established the feasibility and safety of the LESS-RN procedure. In concordance with these other studies, we found that, in comparison with the standard LRN, LESS-RN procedures are not associated with increased complication rates, even when the surgeon is relatively inexperienced with the technique. Historically, in a multi-institutional review involving 185 patients undergoing LRN, 71% of the complications occurred at each institution during the initial 20 cases of what has now been accepted as the standard of care. 11 There should be a low threshold for ancillary port or conversion, however, especially during the early phase of performing LESS-RN. It is extremely technically challenging to acquire adequate hemostasis during LESS surgeries because of the limited working space and the potential for severe instrumental collision.
To date, most comparative studies have shown a noninferiority of LESS over conventional laparoscopy with respect to perioperative outcomes and have revealed an encouraging tendency toward decreased postoperative pain and better cosmesis. 12 –17 Two of the most recent comparative studies on LESS-RN and conventional laparoscopy have reported inconsistent findings with respect to postoperative pain control and the length of hospital stay. 18,19
To determine whether there are any objective benefits for patients undergoing LESS-RN compared with conventional laparoscopy, we used a self-administered questionnaire to evaluate cosmetic satisfaction. This questionnaire has been previously used by Dillenburg and associates 20 in 2006 to assess cosmetic satisfaction in a comparison between retroperitoneoscopic and open surgical RN. In our work, the mean cosmetic satisfaction score favored the LESS-RN group (9.3±0.61 vs 8.4±1.03, P=0.013). Nevertheless, a group of nine elderly patients expressed that the cosmesis of the skin incision was not important to them. Thus, it should be noted that the importance of cosmesis varies greatly between patients. The point at which the advantages justify the increased overall expenses, however, must be taken into consideration. In addition, the VAS used for cosmetic satisfaction assessment warrants validation and quantified evaluation.
Finally, this study is susceptible to all limitations inherent in any retrospective study, and because of the small number of patients in the LESS cohort, even though we obtained statistically significant data, the results may not be clinically significant.
Conclusions
Transumbilical LESS-RN is a feasible, safe, and efficacious procedure with favorable perioperative outcomes that results in significantly improved control of postoperative pain, more rapid recovery of bowel function, and increased cosmetic satisfaction. Additional research, however, including randomized controlled trials and long-term follow-ups will be needed to draw solid conclusions regarding the relative efficacy of this procedure compared with standard approaches.
Footnotes
Acknowledgments
Supported by the Military Major Project for Clinical High-tech and Innovative Technology of China (NO. 2010gxjs057) and the Municipal Hospitals' Project for Emerging and Frontier Technology of Shanghai (NO. SHDC12010115).
Disclosure Statement
No competing financial interests exist.