
Abstract
Purpose:
To present intermediate-term oncologic efficacy of cryoablation (CA) for the treatment of patients with small renal masses in a multi-institution multisurgeon cohort.
Patients and Methods:
We retrospectively reviewed billing records and tumor registries, identifying 116 renal tumors in 116 patients treated with CA by six surgeons at four institutions. Patient age, sex, tumor size, RENAL nephrometry score, complications, and recurrences were recorded.
Results:
One hundred-sixteen patients (66.4% male, 33.6% female) with 116 tumors underwent renal mass CA with a mean follow-up of 27.4 months (range 1–112 mos). Mean tumor size was 2.76±0.97 cm (range 1.1–5.5 cm). Twenty-seven complications occurred in 23 patients for an overall complication rate of 19.8%. Low-grade complications (Clavien I and II) accounted for 92.6% (n=25) of overall complications. Seven (6%) patients had enhancement on initial imaging and were considered incomplete ablations. Local recurrence and metastatic disease developed in four and one patients, respectively. In patients with biopsy-proven renal-cell carcinoma (RCC), the 2- and 5-year recurrence–free survival (RFS) probability was 0.83 (95% confidence interval [CI]: 0.74, 0.95) and 0.77 (95% CI: 0.60, 0.94), respectively. After excluding biopsy proven RCC patients with incomplete ablations, the 2- and 5-year RFS increased to 0.91 (95% CI: 0.82, 1.00) and 0.85 (95% CI: 0.71, 1.00) respectively.
Conclusion:
CA of renal masses results in acceptable oncologic efficacy accompanied by a tolerable complication profile in a cohort with a mean follow-up of 27.4 months. CA remains a viable treatment option for small renal masses in selected patients.
Introduction
We add to the growing body of literature to further define the role of CA in the treatment of patients with renal masses.
Patients and Methods
After obtaining Institutional Review Board approval, we used billing records and cancer tumor registries to identify adult patients undergoing CA as primary treatment for a renal mass. Percutaneous, laparoscopic, and open surgical approaches were included. Patients with metastatic renal-cell carcinoma (RCC) or hereditary syndromes predisposing to multiple, bilateral or recurrent renal tumors were excluded. Charts were retrospectively reviewed and patient demographics recorded. Renal mass size, laterality, location, and R.E.N.A.L. (radius, exophytic/endophytic, nearness, anterior/posterior, location) nephrometry score were recorded. 6 Complications were graded based on the method of Clavien. 7
Ablations were performed based on surgeon preference. Both commercially available CA systems—Endocare (HealthTronics Inc, Austin, TX) and Galil (Galil Medicaere Yokneam, Israel)—were used. The size and number of probes chosen was based on tumor characteristics in an effort to create an ice ball that completely encompassed the mass and a small portion of normal tissue. Each mass underwent two freeze-thaw cycles, the thaw cycles either active or passive.
Laparoscopic, percutaneous, and open approaches were used, based on tumor location, clinical situation, and surgeon preference. To briefly summarize the laparoscopic approach, the kidney was exposed using either a transperitoneal or retroperitoneal approach and adjacent structures were mobilized to prevent CA injury. Intraoperative ultrasonography was performed selectively to identify the lesion and guide probe placement. The lesion was exposed by dissecting away adjacent perirenal fat, and the overlying adipose tissue was sent for pathologic examination. Core biopsy of the lesion was performed at surgeon discretion. Cryoprobes were then inserted under visual and/or ultrasonographic guidance, and the ablation was performed. Surgicel® (Ethicon Somerville, NJ) and FloSeal® (Baxter, Deerfiedl, IL) were used as needed for hemostasis.
For percutaneous CA, the patient was placed in the prone position after induction of general anesthesia. CT guidance was used to position probes into the lesion and monitor the ice ball size during the ablative process. All percutaneous ablations were performed in the interventional CT suite with both the urologist and radiologist present. Open CA was performed in cases in which the patient was undergoing another intra-abdominal procedure. In all open cases, transperitoneal access was used. As with the laparoscopic approach, ultrasonography and visual guidance were used to identify the tumor and guide probe placement before probe placement.
CA follow-up protocols were not standardized between the different surgeons, but patients received initial contrast-enhanced imaging with either CT or MRI shortly (4–6 weeks) after the ablation. Lesions with persistent contrast enhancement on this first imaging study were considered incomplete ablations as opposed to recurrent cancers. Subsequent imaging typically occurred on a biannual or annual basis. Contrast enhancement or lesion growth on subsequent imaging was categorized as a local recurrence at the ablation site. Rim enhancement, thought to arise from epithelial injury and interstitial hemorrhage along the periphery of the ablated lesion, was not considered a treatment failure or recurrence. Imaging, laboratory evaluation, and physical examination were used to identify metastatic spread.
Summary statistics are presented for patient demographics, tumor characteristics, and renal biopsy results. Kaplan-Meier survival analysis for the entire cohort and those with biopsy-proven RCC was performed to determine recurrence-free survival (RFS). Kaplan-Meier analyses were performed on the entire cohort and then again after excluding those with initial treatment failure. The R statistical package (
Results
We identified 116 patients with 116 tumors who underwent CA as the initial treatment for their renal mass (Table 1). Six different surgeons performed these ablations at four different institutions. Mean age at the time of ablation was 68.3±12.4 years. Median Charlson score was 0 (0–6). Mean tumor size was 2.76±0.97 cm. R.E.N.A.L. nephrometry scores were low (4–6), intermediate (7–9), or high (10–12) in 62.2%, 33.7%, and 4.1%, respectively. Laparoscopic, percutaneous, and open approaches were used in 92.2%, 6.1%, and 1.7% of cases, respectively. A total of 27 complications were noted in 23 patients for an overall complication rate of 19.8% (Table 2). Low-grade complications (Clavien I and II) occurred in 19.8% of procedures and accounted for 92.6% of overall complications. High-grade complications (Clavien ≥III) occurred in 1.7% of procedures and accounted for 7.4% of overall complications. Renal biopsy was performed in 81.9% patients and revealed RCC in 65.3%.
RCC=renal-cell carcinoma.
Mean follow-up was 27.4 months (range 1–112 mos). A total of seven tumors had persistent enhancement on initial imaging and were considered primary treatment failures. Of patients with these initial treatment failures, four elected surveillance, two underwent partial nephrectomy, and one underwent radical nephrectomy. Of the three patients electing surgical extirpation, pathologic evaluation revealed clear-cell RCC in two and chromophobe in one. After a mean follow-up of 37.9 months (range 13–69), all 7 patients were alive without evidence of metastatic disease.
Tumor recurrence developed in five patients. Local recurrences developed in four patients after a mean follow-up of 24.5 months (range 9–45 mos). Two patients underwent surgical intervention, partial and radical nephrectomy, with pathology reports showing RCC and were subsequently lost to follow-up. One patient elected observation for 56 months before undergoing a partial nephrectomy that revealed RCC and is alive without evidence of disease 14 months later. Metastatic lung cancer developed in one patient who elected observation, and the patient died from that disease. Biopsy-proven RCC to the spine developed in one patient undergoing CA for a 3.8 cm tumor at 11 months after surgery. Renal ablation site biopsy at 11 months postablation showed only fibrosis, raising the question as to whether this metastatic lesion was present but undetectable before ablation.
Kaplan-Meier survival curves for RFS in all patients and patients with pathology-confirmed RCC can be found in Figures 1 and 2, respectively. The 2- and 5-year RFS rates were 0.89 (95% confidence interval [CI]: 0.82, 0.96) and 0.86 (95% CI: 0.78, 0.95). After restriction to patients with pathology-confirmed RCC, the 2-year RFS decreased to 0.83 (95% CI: 0.74, 0.95) and the 5-year RFS rate decreased to 0.77 (95% CI: 0.60, 0.94). Excluding those patients who had an incomplete ablation, the 2- and 5-year RFS rates were 0.95 (95% CI: 0.90, 1.00) and 0.92 (95% CI: 0.82, 0.99), respectively (Fig. 3). After excluding the patients with incomplete ablations, for patients with confirmed RCC, the 2- and 5-year RFS were 0.91 (95% CI: 0.82, 1.00) and 0.85 (95% CI: 0.71, 1.00), respectively (Fig. 4).
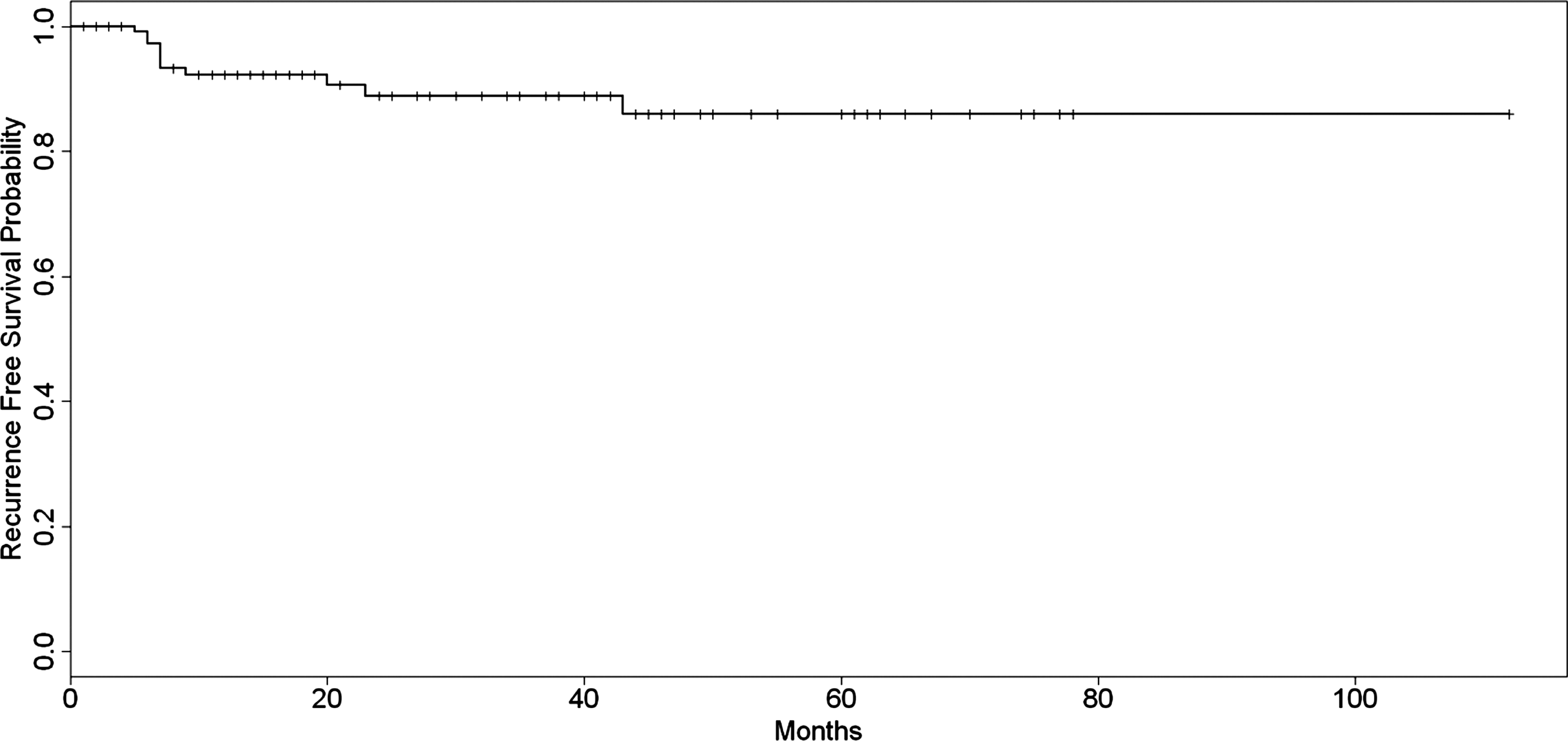
Kaplan-Meier curve for recurrence-free survival for all patients.

Kaplan-Meier curve for recurrence-free survival for patients with confirmed renal-cell carcinoma.
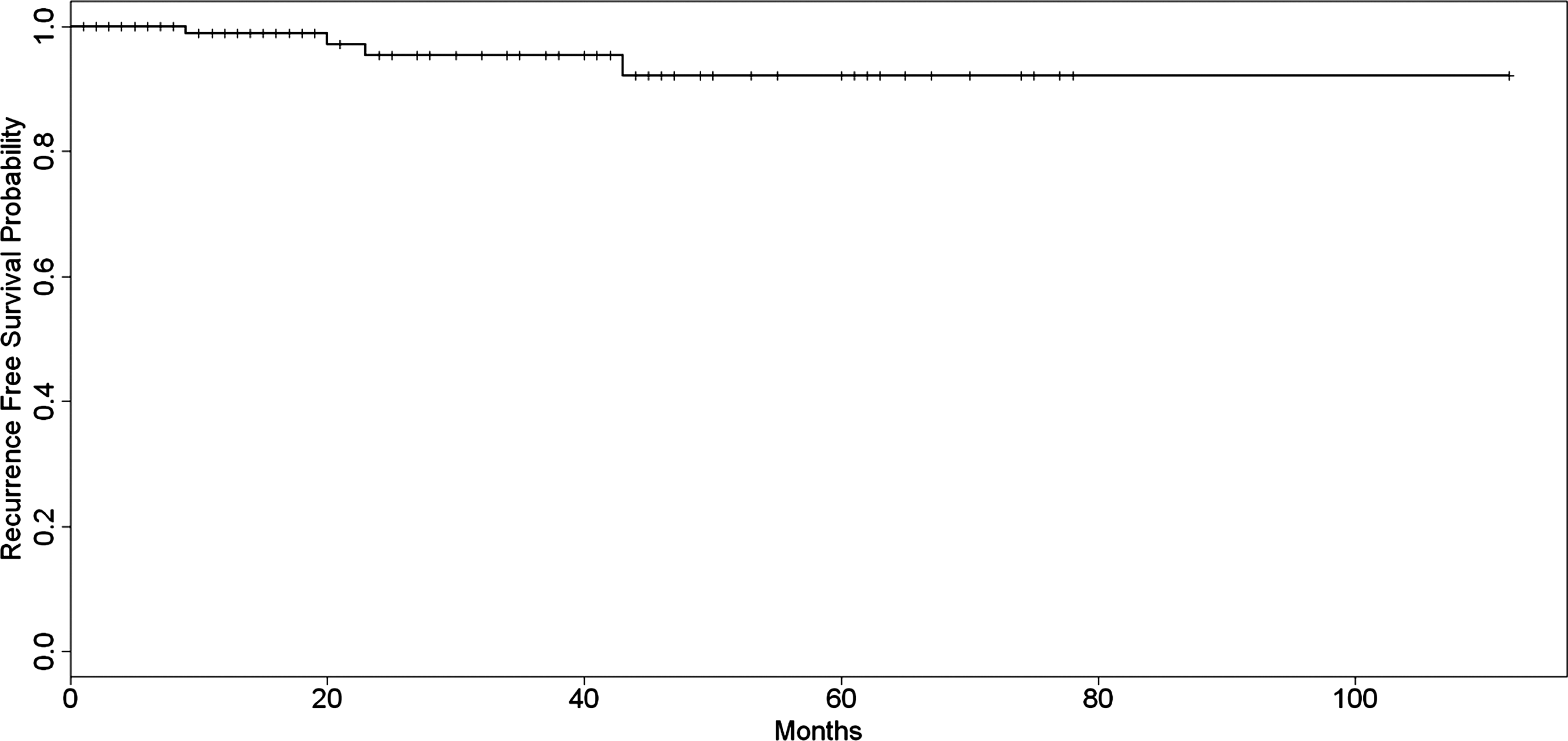
Kaplan-Meier curve for recurrence-free survival for all patients (excluding incomplete ablations).

Kaplan-Meier curve for recurrence-free survival for patients with confirmed renal-cell carcinoma (excluding incomplete ablations).
Discussion
As the use of axial imaging has increased, so has the diagnosis of renal masses, with an estimated 58,000 new cases in the United States in 2010. 1 Complete surgical excision by way of partial nephrectomy, with its attendant decrease in cardiovascular complications and mortality, is now the standard of care for the treatment of patients with small renal masses. 8,9 CA is a reasonable surgical option in patients who are candidates for nephron-sparing surgery, but are unwilling or unable to undergo partial nephrectomy. Recent guidelines for the management of small renal masses state that a discussion regarding CA is an option in healthy patients with cT1 renal mass and recommended in patients with increased surgical risk. 9
Intermediate-term individual and institutional series examining patients with sporadic renal masses treated with CA report local control and cancer-specific survival rates of 83.6% to 100% and 94% to 100%, respectively. 10 –15 Kunkle and Uzzo 16 found CA had low rates of local recurrence (5.2%), need for re-treatment (1.3%), and the development of metastatic disease (1%). In a separate analysis, Kunkle and associates 17 found that although CA was associated with an increased risk of local recurrence (relative risk=7.45) compared with partial nephrectomy, there was no difference in the development of metastatic disease.
In the series with the longest follow-up to date, Aron and colleagues 4 recently reported the oncologic outcomes of 80 patients who were treated with laparoscopic CA and had a minimum follow-up of 5 years. Followed for a median of 93 months (range 60–132 mos), the 5-year overall survival, cancer-specific survival, and RFS was 84%, 92%, and 81%, respectively. The 10-year survival analysis indicated overall survival, cancer-specific survival, and RFS were 51%, 83%, and 78%, respectively. No patient in this series was noted to have an incomplete ablation, but the authors did note 11 (20%) locoregional and/or distant failures, with time to failure ranging from 6 to 90 months.
In patients with biopsy-confirmed RCC who had an adequate initial treatment of their tumor, we noted a 92% probability of 5-year RFS. These results correlate well with other longer-term studies; however, we observed a higher incidence of unsuccessful ablations (6%). While tumor characteristics and adjacent vascular structures may contribute to unsuccessful ablations, the placement of too few probes resulting in inadequate lesion size is also likely responsible. A recent publication examining the isotherms of two different cryoprobes in gel, ex-vivo and in-vivo found that: (1) gel and ex-vivo isotherms did not predict in-vivo freezing; (2) in-vivo temperatures 5 mm distal to the probe are not adequate for producing cell death; and (3) in-vivo neither system achieved a temperature of −20°C at each point along even the 10-mm isotherm, a significant discrepancy from manufacturer supplied isotherms performed in gel. 18 These results argue for the anticipation of smaller per-probe ablation zones and the use of temperature monitoring probes.
CA is a safe option for the treatment of patients with renal masses with acceptable morbidity. Complication rates for percutaneous and laparoscopic approaches range from 0% to 11% and 10% to 62%. 4,12,19 Using the Clavien complication grading system, Finley and coworkers 19 reported complications in 11.1% of percutaneous ablations and 38.9% of laparoscopic ablations. Comparing laparoscopic and percutaneous CA, Lehman and colleagues 12 reported a 62% complication rate in the laparoscopic group compared with 0% in the percutaneous group. Ablation complications were all in tumors >3.1 cm (mean 4.7 cm). Similarly, Laguna and associates 20 found a 15.5% complication rate in patients undergoing laparoscopic CA with a receiver operating characteristics analysis suggesting a 3.4 cm cutoff for developing complications. Keeping with these observations, we noted a 19.8% complication rate, the majority of which, 92.6%, were minor (Clavien grade I or II), and the mean tumor size in ablations with complications was 2.86 cm.
The current study is subject to the limitations of a retrospective analysis. Multiple surgeons may be both a weakness and strength of the study design because variations in technique add a confounding variable that could affect outcomes; however, this likely reflects the overall urologic community practice. Despite the variation in practice, encouraging results are seen in patients undergoing successful CA, and follow-up strategies in patients with unsuccessful CA have prevented the development of metastatic disease.
Conclusion
We present intermediate term treatment outcomes in patients undergoing primary CA for the treatment of SRMs. Based on these results CA remains a viable treatment option for the well selected patient.
Footnotes
Disclosure Statement
Dr. Anderson has served as a proctor for Galil Medical.