
Abstract
Background and Purpose:
Laparoscopic and robotic partial nephrectomy involves temporary clamping of the renal artery, making the kidney susceptible to ischemic damage. Isoprostane represents one potential marker of oxidative injury. The objective was to determine if renal interstitial isoprostane levels can quantitate renal damage secondary to warm ischemia. A second goal is to investigate allopurinol for renoprotective abilities using this model. We chose to investigate potential renoprotection of allopurinol because previous studies have demonstrated transplant kidneys pretreated with allopurinol to have less damage from ischemia.
Materials and Methods:
A microdialysis probe was inserted into the renal parenchyma of rats to allow continuous dialysis and collection of the effluent for isoprostane levels. After clamping of the renal vessels for predefined intervals of ischemia, the interstitial effluent from the probe was collected and subsequently analyzed for isoprostane levels with and without allopurinol pretreatment.
Results:
Clamping of the renal artery and vein produced increases in isoprostane levels during the ischemic period and larger increases during reperfusion. There was a trend for increased postclamp isoprostane levels as clamp times increased. When comparing isoprostane levels in rats that did not receive allopurinol, there were significant differences between the clamp and postclamp levels of isoprostane, with allopurinol offering protection to the kidney from ischemic changes caused by clamping the renal hilum.
Conclusions:
Our data have demonstrated that isoprostane levels are a potential real-time marker of renal ischemia and reperfusion injury. We also found allopurinol administration demonstrated a trend toward renoprotective abilities in the hilar occluded kidney.
Introduction
Partial nephrectomy for renal carcinoma involves clamping the renal artery temporarily, rendering the kidney ischemic during tumor resection. While decreasing hemorrhage, this exposes the kidney to becoming susceptible to ischemia and reperfusion injury. The time limit of reversible ischemic damage to the kidney is controversial. Experimental studies with human subjects demonstrated that renal damage and cellular degeneration of the nephron begins after 30 minutes of clamping. 2,3 Warm ischemia time (WIT) is the strongest modifiable surgical risk factor for postoperative chronic kidney disease. 4 Some experts recommended that WIT should be kept less than 20 minutes, and in difficult cases in which warm ischemia time may exceed 35 minutes, one should provide cold ischemia for a renoprotective effect. 5,6
In vivo studies have demonstrated the ability of 8-isoprostane to predict oxidative stress during ischemia, 1 yet studies have not been performed to measure ischemic damage during partial nephrectomy by quantifying renal interstitial 8-isoprostane levels. We predict measurements of renal 8-isoprostane levels during partial nephrectomy may be able to quantify real-time irreversible kidney damage and ischemia outcomes. We hypothesize that renal interstitial 8-isoprostane levels will increase as vascular clamp time increases and rise further during reperfusion phases.
This study aims to investigate the relationship between renal ischemia injury and concentrations of 8-isoprostane in a rat kidney model during renal hilar clamping. Renal tissue 8-isoprostane level was measured using a microdialysis probe inserted in the renal parenchyma.
In addition, using 8-isoprostane as a marker of renal ischemia, this model can also be adopted to investigate renoprotective abilities of various pharmacotherapeutics. After determining that the biomarker 8-isoprostane was an effective marker of ischemia, we investigated whether allopurinol was an effective agent for renoprotective abilities. Allopurinol, a xanthine oxidase inhibitor, is believed to reduce reperfusion injury by scavenging free radicals produced during reperfusion of ischemic tissues. 7 Xanthine oxidase has been hypothesized to be a potential source of oxygen-derived free radicals during ischemic-reperfusion injury. 7 By measuring differences in 8-isoprostane levels during renal hilar clamping in rats that have been premedicated with allopurinol, a second goal of this study was to investigate allopurinol for renoprotective abilities using this model. We chose to investigate allopurinol for renoprotective abilities because previous studies have demonstrated transplant kidneys pretreated with allopurinol offer protection from ischemic damages. 8,9 An additional study by Hopson and associates 7 revealed allopurinol was able to reduce reperfusion injury in the porcine myocardium.
Materials and Methods
All of the experimental procedures described in this study were approved by and performed in accordance with the guidelines established by the Tulane University Animal Care and Use Committee. These experiments were conducted in male Sprague-Dawley rats weighing 250–300 g (8 wks old) that were purchased from Charles River Laboratories (Wilmington, MA), housed at least 3 days for acclimatization in a temperature- and light-controlled room, and allowed free access to a standard diet (Ralston-Purina, St. Louis, MO) and tap water.
Rats were anesthetized with thiobutabarbital sodium (Inactin®, Sigma-Aldrich, St. Louis, MO) at a dose of 100 mg/kg. Supplemental doses of anesthesia were administered throughout the experimental period as needed. The rats were placed on a servocontrolled surgical table that maintained body temperature at 37°C. Tracheostomy was performed, and the animals were continuously provided with a mixture of 95% O2 and 5% CO2 through the endotracheal tube (PE-200). The right jugular vein was catheterized for intravenous administration of 6% albumin solution at a rate of 20μL/min and continual monitoring of the carotid artery blood pressure using the AcqKnowledge data acquisition system (Biopac, Goleta, CA).
The left kidney was exposed via a flank incision and placed in a Lucite cup (Fig. 1). After a 60-minute stabilization period, the experimental protocol was started. After clamping the renal vessels, effluent from a BASi IV-10 Vascular 10-mm membrane microdialysis probe were collected and 8-isoprostane levels were analyzed. This was performed by inserting the microdialysis probe into the renal parenchyma and connecting it to a microinfusion pump that was perfused with isotonic saline and heparin (30 units /mL) at a rate of 1 μL/min (Fig. 2). After a 30-minute equalization period, renal interstitial fluid from the microdialysis probes were collected during the following time periods: Preclamp (after 30 min of initial equalization), during clamp (15 min after clamping renal hilum), and postclamp (30 min after unclamping) (Fig. 3). The experiment was repeated on additional rats, while extending the clamp time to 30, 45. and 60 minutes, in addition to obtaining pre- and postclamp 8-isoprostane levels (as performed with the 15-min clamp-time experiment). At each time period, 5 to 10 additional rat kidneys were analyzed for isoprostate levels.
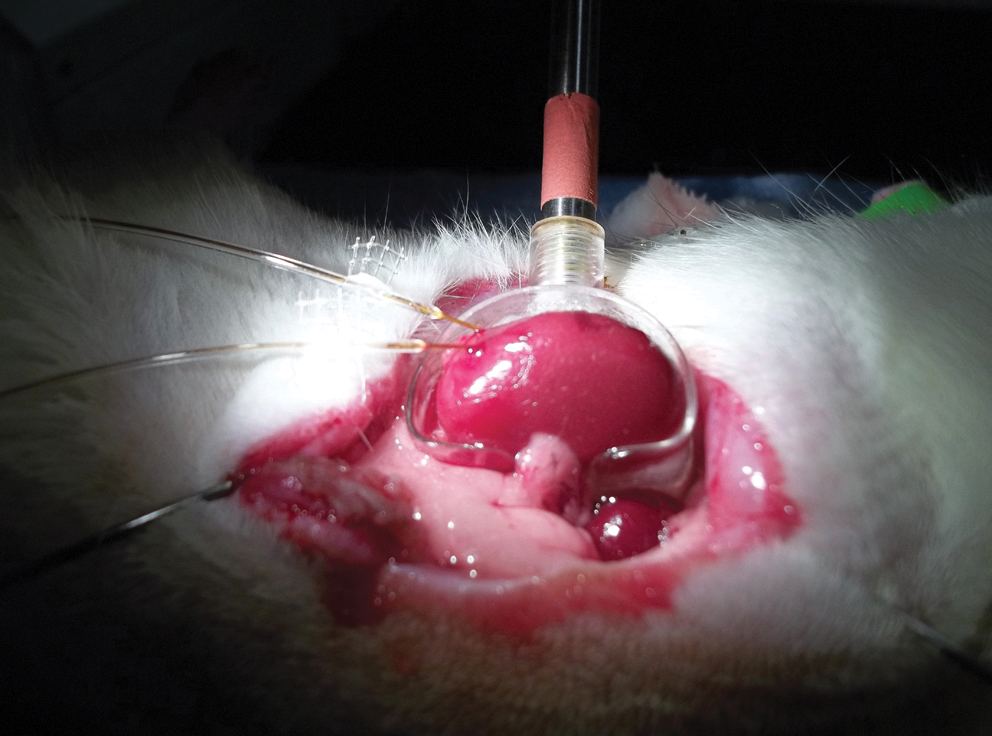
Left kidney was exposed via a flank incision and placed into a Lucite cup.
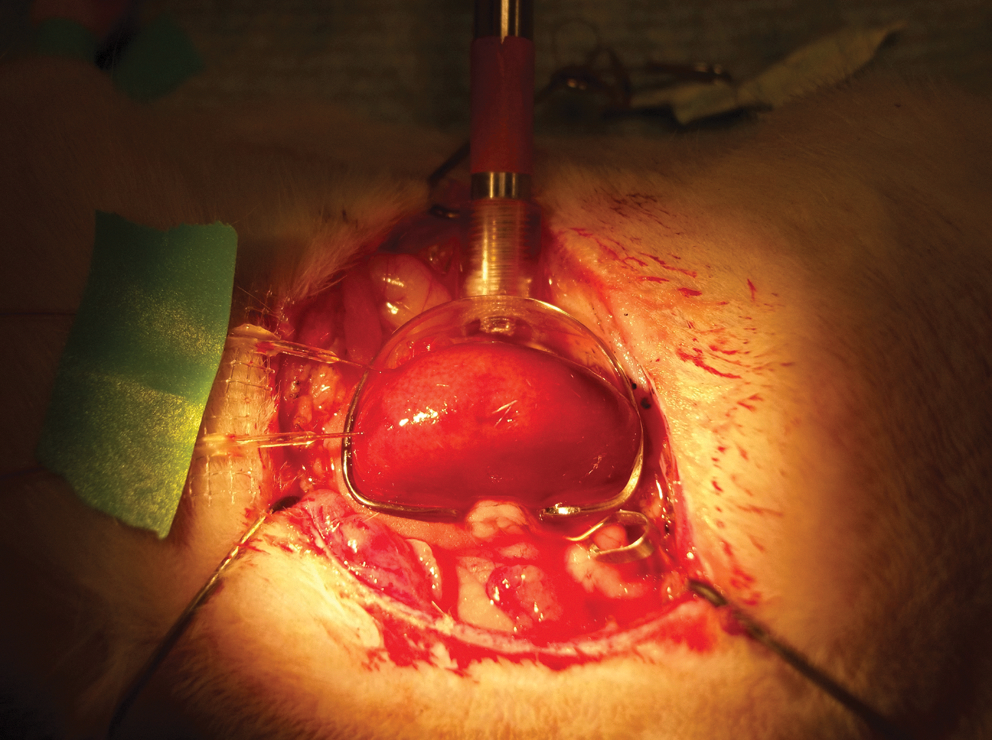
The microdialysis pump was inserted into the renal parenchyma and connected to a microinfusion pump.

Isoprostane collection.
Seven additional rats were used to study the effect of allopurinol on renal ischemia-reperfusion injury. They underwent the same operative procedure as the 60-minute clamp group, but were treated with allopurinol (100 mg/kg) (MP Biomedicals, Solon, OH) injected as a bolus 5 minutes before renal unclamping (55 min after clamping). The analysis was accomplished by first including a 30-minute equalization period, followed by measuring 8-isoprostane levels in the rat kidney interstitial fluids before clamping, after clamping for 60 minutes, and again 30 minutes after unclamping the renal hilum—similar to what had been performed in the rats that were not premedicated with allopurinol.
All of the interstitial fluid samples were preserved with 0.005% butylhydroxytoluene prepared in ethanol and kept frozen (−80°C) until analyzed. The fluid samples were subsequently analyzed for 8-isoprostane levels using an enzyme immunoassay kit (Cayman Chemical, Ann Arbor, MI) and Optima microplate reader (BMG LABTECH, Cary, NC). At the conclusion of the live experiments, the left kidney was removed, stripped of all surrounding tissue, blotted dry, and weighed so that the calculated parameters could be expressed per gram of kidney. 10 The rats were sacrificed at the end of the experiment.
All values were normalized per gram of kidney. Data are expressed as means±standard error (SE). Statistical comparisons of differences in the groups were carried out by one-way analysis of variance and Student t test. Differences in the mean values were deemed significant at P<0.05.
Results
In the 15-minute clamp period, the average increase in 8-isoprostane from baseline level to clamp was 1.88 pg/mL/g of kidney and from baseline to postclamp was 6.20 pg/mL/g. The 30-minute clamp period demonstrated an increase in 8-isoprostane from baseline to clamp of 0.41 pg/mL/g and an increase from baseline to postclamp of 4.67 pg/mL/g. When the renal artery was clamped for 45 minutes, the increase in 8-isoprostane from baseline to clamp was 1.18 pg/mL/g and from baseline to postclamp was 15.09 pg/ml/g. Finally, the increase in 8-isoprostane after a 60-minute clamp period was 11.78 pg/mL/g and from baseline to postclamp level, the increase was greatest at 22.95 pg/mL/g.
The data demonstrated a trend, showing higher 8-isoprostane levels after renal clamping compared with 8-isoprostane levels before renal clamping. The differences, however, in 8-isoprostane levels were not significantly different between preclamp and clamp or postclamp levels of 8-isoprostane in the 15-minute clamp group (n=6, P=0.080), or in the 30-minute clamp group (n=9, P=0.52), or in the 45-minute clamp 45 (n=6, P=0.63). There was a distinct, statistically significant difference, however, between preclamp and clamp levels of isoprostane in the 60-minute clamp group (n=8, P=0.039). Overall, the data suggested linear correlations with higher 8-isoprostane levels as WITs increased (Table 1).
Analysis to investigate ischemic protection using allopurinol was performed only with the 60-minute clamp period, because this was the only group that was statistically significant without allopurinol administration. When the renal hilum was clamped for 60 minutes, there was a statistically significant difference between the allopurinol group compared with the group without allopurinol, at the postclamp time point of 30 minutes (t=2.590, P=0.022), with allopurinol offering protection to the kidney from ischemic damage caused by clamping the renal hilum. Figure 4 shows a comparison of 8-isoprostane concentrations in rats with and without allopurinol pretreatment for the 60-minute clamp period.
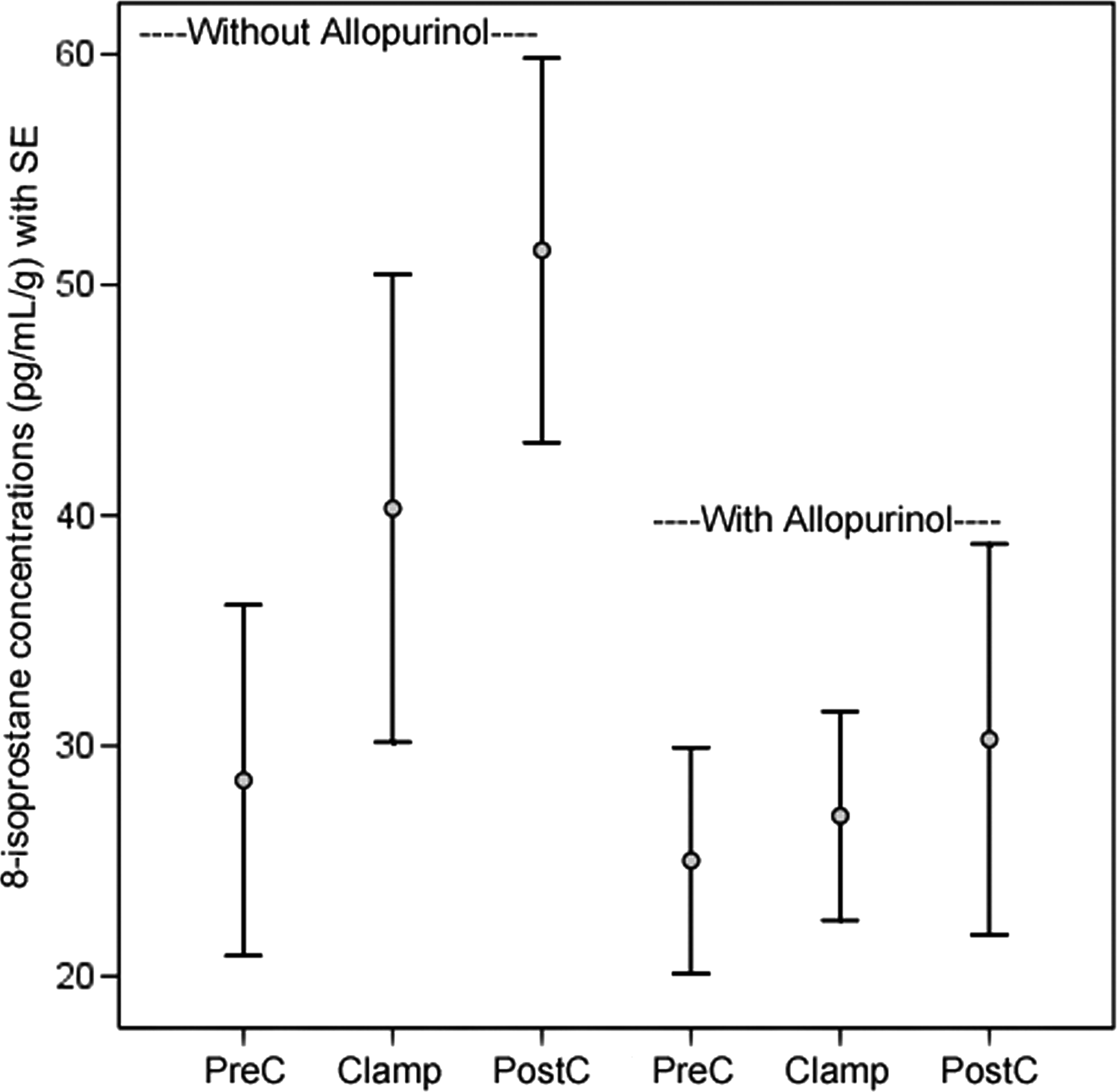
8-Isoprostane concentrations in the renal interstitium of rats with and without allopurinol pretreatment. SE=standard error; PreC=preclamp 30 minutes; Clamp=60 minutes; PostC=postclamp for 30 minutes.
In rats with allopurinol pretreatment, there was no statistically significant differences between levels of 8-isoprostane when comparing the preclamp and clamp or postclamp levels for the 30-minute (n=6, P=0.205), 45-minute (n=6, P=0.091), and 60-minute (n=7, P=0.214) time points (Table 2).
Discussion
Ischemia-reperfusion injury is known to be a risk factor that affects renal graft function after transplantation. In 2006, Waller and colleagues 11 performed a study to evaluate oxidative damage after ischemia-reperfusion using an isolated organ perfusion model of the transplanted kidney to identify a biomarker for ischemia-perfusion injury. 11 The conclusion of their study suggested that 8-isoprostane is a reliable biomarker to predict ischemic injury in the transplanted kidney. Using this concept in a different renal ischemia model, we sought to further investigate 8-isoprostane as a biomarker to indicate ischemic injury during renal hilar clamping as performed during partial nephrectomies.
Previous studies have evaluated renal ischemia and reperfusion injury caused by clamping the renal hilum during partial nephrectomy. 3,4 Kidney ischemia/reperfusion injury is histologically characterized by tubular damage. 12 Investigators have attempted to elucidate the mechanisms by which renal ischemia and reperfusion injury lead to the development of chronic kidney disease. 13 In addition, many researchers have evaluated a variety of therapeutic agents to prevent renal injury induced by renal ischemia and reperfusion injury. 12,13 Mejía-Vilet and coworkers 13 found that spironolactone administration prevents renal injury induced by ischemia/reperfusion injury. Recently, nicotine administration has been shown to be a powerful inhibitor of ischemia-induced renal toxicity through cholinergic and anti-inflammatory pathways. 13
Testosterone administration to female mice increases kidney susceptibility to ischemia, and castration of male mice reduces the ischemia-induced kidney injury. 14 Testosterone has been found to increase ischemia-induced renal damage in the mouse by inhibiting postischemic activation of nitric oxide synthases and extracellular signal-related kinases through nonandrogen receptor-medicated mechanisms, leading to increased inflammation and increased functional injury to the kidney. 15 Although estrogen administration can partially reduce kidney injury associated with ischemic injury, studies have revealed the presence of testosterone, more than the absence of estrogen, plays a critical role in gender differences in susceptibility of the kidney to ischemic injury. 15 These findings are important to our understanding of the pathophysiology of renal failure after ischemic injury, and provide a new paradigm for the design of therapies for ischemia reperfusion injury.
Our study aimed to investigate the relationship between WIT, renal ischemia reperfusion injury, and concentration of 8-isoprostane using a rat kidney model. Our results showed 8-isoprostane levels to be higher after renal clamping compared with preclamping in all time periods. In addition, as WIT increased, 8-isoprostane levels also increased. Last, in all the time models tested, 8-isoprostane levels rose even higher during the reperfusion period, suggesting that further cellular damage was occurring after the kidney was revascularized. These results suggested that 8-isoprostane levels are a potential real-time marker of renal ischemia and reperfusion injury. Previous researchers have demonstrated 8-isoprostane's potent renal vasoconstrictive activity and have theorized that this may the mechanism of renal injury during renal ischemia. 16 –18 Therefore, future development of pharmacotherapy to block 8-isoprostane's potent renal vascoconstrictive effects may prove to limit renal damage during times of ischemia. 16 –18
In addition, because 8-isoprostane represents a marker of renal ischemia, this model was also used to test other medications' potential renoprotective ability by measuring changes in 8-isoprostane levels after administration of the test drug before renal hilar clamping. The medication we chose to study was allopurinol, because previous studies in transplant kidneys have demonstrated pretreatment with allopurinol offered protection from ischemic damage. 19,20 Testing for ischemic changes was performed only in the 60-minute group because this was the only group that was statistically significant without allopurinol administration. In our study, we found allopurinol administration did demonstrate a trend toward renoprotective abilities in the hilar occluded kidney.
This study is limited by small numbers, and we are continuing these experiments to expand our data. While allopurinol has resulted in lower levels of isoprostane, further studies are needed to determine if the lower isoprostane levels correlate with less ischemic damage to the renal unit. Future studies, include performing the study with a live solitary kidney model and obtaining postoperative creatinine clearance of the renal unit after unclamping to determine if allopurinol has preserved renal function, and potentially performing biopsies at different time points. Ultimately, further clinical studies are needed to determine if allopurinol is renoprotective in humans.
Conclusion
Clamping of the renal artery and vein produced increases in 8-isoprostane levels during the ischemic period, and larger increases were found during the reperfusion period. In addition, there was a trend for increased postclamp 8-isoprostane levels as clamp times increased from 30 and 45 to 60 minutes. Overall, our data have demonstrated that 8-isoprostane levels are potential real-time markers of renal ischemia and reperfusion injury. We also found that pretreatment with allopurinol demonstrated protector effects against renal ischemia during renal hilar clamping. With this evidence, we believe that a clinical trial to investigate potential protective effects of allopurinol to the ischemic kidney during renal hilar clamping is justified. This has particular clinical importance when periods of warm ischemia are unavoidable, as in laparoscopic and robot-assisted partial nephrectomies.
Footnotes
Disclosure Statement
No competing financial interests exist.