
Abstract
Purpose:
The objective of this randomized in-vitro study was to compare the suturation time, integrity, and quality of the bladder closure in fresh cadaver pig bladders performed with barbed polyglyconate sutures vs polyglactin 910 sutures in running and interrupted fashion.
Materials and Methods:
Forty-eight pig bladders, each weighing from 120 to 150 g, were randomly divided into three groups: Group 1 (interrupted polyglactin 910 suture group), group 2 (running polyglactin 910 suture group), and group 3 (running barbed polyglyconate suture group). The bladder defects were closed laparoscopically, and the suturation times were noted. Two surgeons evaluated the integrity of each bladder closure. A cystometry was performed, and the filling and leak pressures were noted. A Kruskal-Wallis variance analysis test was used to compare the results of the three groups, and P<0.05 was considered significant.
Results:
There was a statistically significant difference between the mean suturation times of three groups: Group 1, 15.2 minutes; group 2, 9.14 minutes; and group 3, 7.13 minutes (P<0.05). Mean bladder capacity at the time of leakage was 276.2, 353.8, and 419.7 mL for groups 1, 2, and 3, respectively, and the difference was statistically significant (P<0.05).
Conclusion:
For the first time, we demonstrated laparoscopic knotless closure of bladder defects using the barbed polyglyconate suture material in an experimental in-vitro model. Closing the pig bladder with running knotless barbed suture provides a more effective and faster watertight bladder closure than traditional polyglactin 910 suture material.
Introduction
To simplify the urologic reconstructive operations, a barbed polyglyconate suture material (V-loc 180™; Covidien, Tyco Healthcare Group, Norwalk, CT) has been recently and successfully applied in vesicourethral anastomoses and posterior bladder reconstructions during laparoscopic radical prostatectomies and robot-assisted partial nephrectomies. 9 –11 Barbed sutures enable easier tissue approximation and overcome the problems of intracorporeal knot tying. The loop end makes the first knot needless, and the approximation of the suture anchors into the tissues negates the need for knots to hold the tissues in place. 9,10,12,13
We hypothesized that barbed sutures may reduce operative time and urine leaks for laparoscopic urinary bladder closures. The pig bladder model is an excellent approximation of the human urinary tract and has proved a good training model for laparoscopic suturing in many experimental studies. 6,14,15 Histologically, the pig bladder consists of urothelium, lamina propria, and inner and outer smooth muscle layers that are similar to the human bladder in thickness and arrangement. 16
The objective of this randomized in-vitro study was to compare the suturation time, integrity, and quality of the bladder closure in fresh cadaver pig bladders performed with barbed polyglyconate sutures vs polyglactin 910 (Vicryl, Ethicon, Johnson & Johnson Intl, Belgium) sutures in running and interrupted fashion.
Materials and Methods
Seventy nonpregnant female domestic pigs, each weighing approximately 25 kg, were slaughtered and their bladders and urethras were removed en bloc in a slaughterhouse. The bladders were prepared and used after a fine dissection during the same day in the study. Residual urine was gently removed, and the bladders were weighed. Forty-eight bladders, each weighing from 120 to 150 g, were selected accordingly. The selected bladders were then transferred to a heated organ bath (temperature maintained at 33°C–36°C) containing a saline solution.
Cystometry was performed with a 7F dual lumen vesical catheter as a first step. Filling volumes and pressures were noted in an Excel spreadsheet. The transducer was calibrated before each experiment. At the outset, each bladder was filled with saline at maximum filling speed of 40 mL/min to give a baseline volume of 500 mL, similar to that of a human bladder. 17
The bladder filling volumes and pressures were noted in an Excel spreadsheet, after which the bladders were randomized to three groups: Group 1 (interrupted polyglactin 910 suture group), group 2 (running polyglactin 910 suture group), and group 3 (running barbed polyglyconate suture group) (Fig. 1).

The bladders were equilibrated in the heated organ bath for at least 20 minutes before incision and suturing. A 3.5-cm longitudinal cystotomy incision was performed to the bladder dome and a single layer closure, using laparoscopically assisted suturing, was performed in a training box by one surgeon who has extensive experience in laparoscopic surgery (MA). The incision was closed in a watertight manner with a running or interrupted suture of 3/0 SH-plus polyglactin 910 stitch on a 26-mm needle and running suture with 3/0 polyglyconate barbed suture on a 26-mm needle (Fig. 1).
In group 1, the incisions were closed with interrupted polyglactin 910 sutures. For the interrupted technique, three knots were tied for each of the six stitches, and a suture interval of 0.5 cm was used to close the bladder. In group 2, the incisions were closed with running polyglactin 910 sutures. For the running technique, three knots were tied at both ends of the suture material, and a total of six suture passes through the bladder on each side of the approximation were performed. In group 3, the incisions were closed with running barbed polyglyconate sutures. The first suture passed the needle through the looped end, and the last suture was placed in the unincised tissue without tying a knot. After each stitch, the suture was gently tugged to seed the barbs into the bladder wall. Figure 2 shows the cohort diagram illustrating a randomization study design.
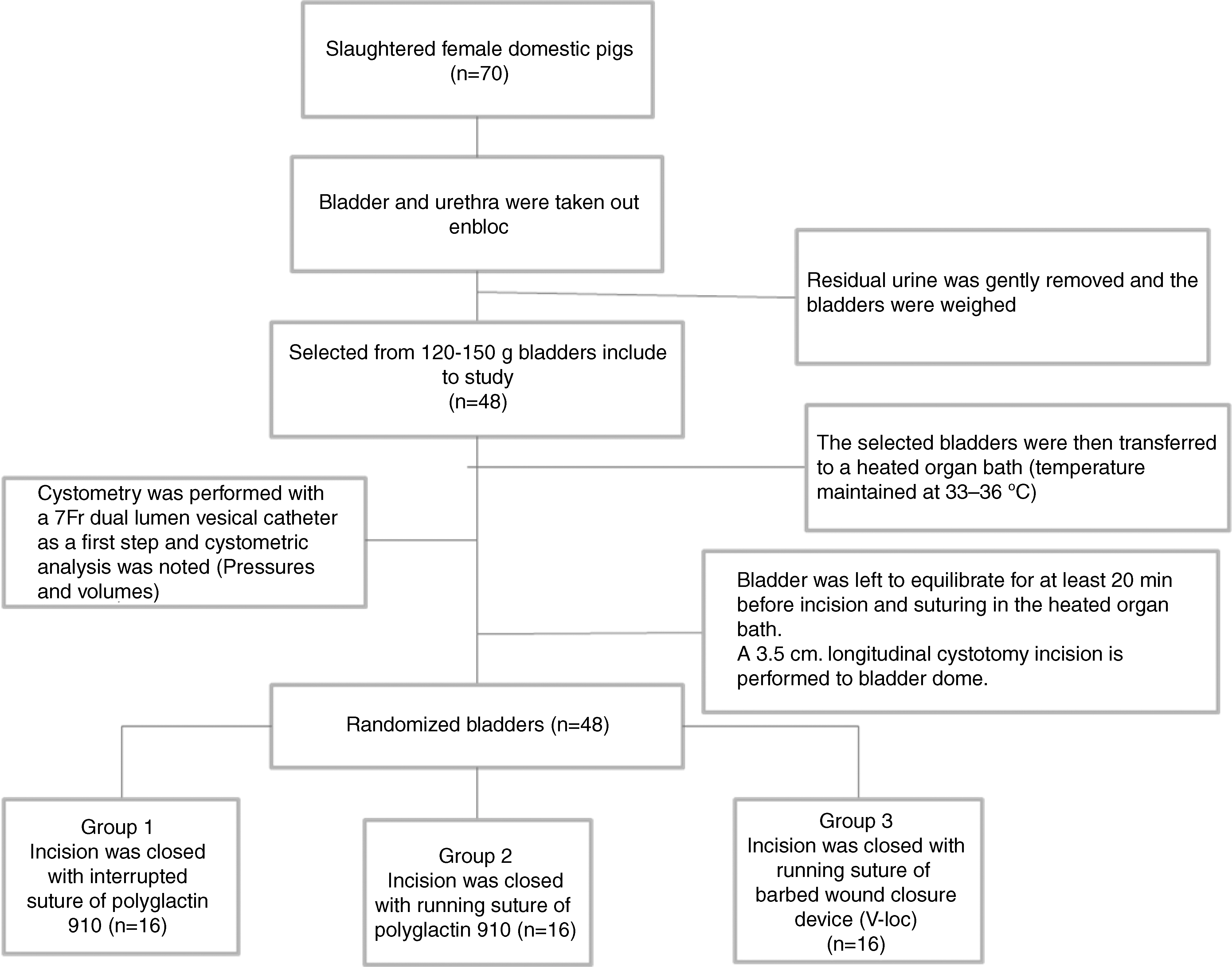
Study design diagram.
With all suture types, the distance of travel between the stitches was consistent and was believed to provide a watertight seal by two authors (ASG, MA). Closure time was defined as the time elapsed from entry of the suture into the training box to the time the needle was withdrawn and recorded for each group.
Using saline stained with povidone-iodine (to facilitate identification of leakage), the bladders were distended via the urethral catheter to a volume of 500 mL, depending on the capacity, and examined for evidence of extravasation. After the suturing studies, the filling and leak pressures were noted in the same Excel spreadsheet.
Data were documented using Microsoft Excel (Microsoft, Germany), and the three groups were compared statistically with the Kruskal-Wallis variance analysis test using SPSS software (SPSS, Inc, Chicago, IL). For all tests, P<0.05 was considered significant.
Results
Mean bladder weight, mean intravesical filling pressure, and mean filling capacity were similar in all three groups (Table 1). There was a statistically significant difference between the mean suturation times of the three groups: Group 1 (interrupted suture with polyglactin 910), 15.2 minutes; group 2 (running suture with polyglactin 910), 9.14 minutes; and group 3 (running suture with barbed polyglyconate), 7.13 minutes (P<0.05) (Fig. 3).
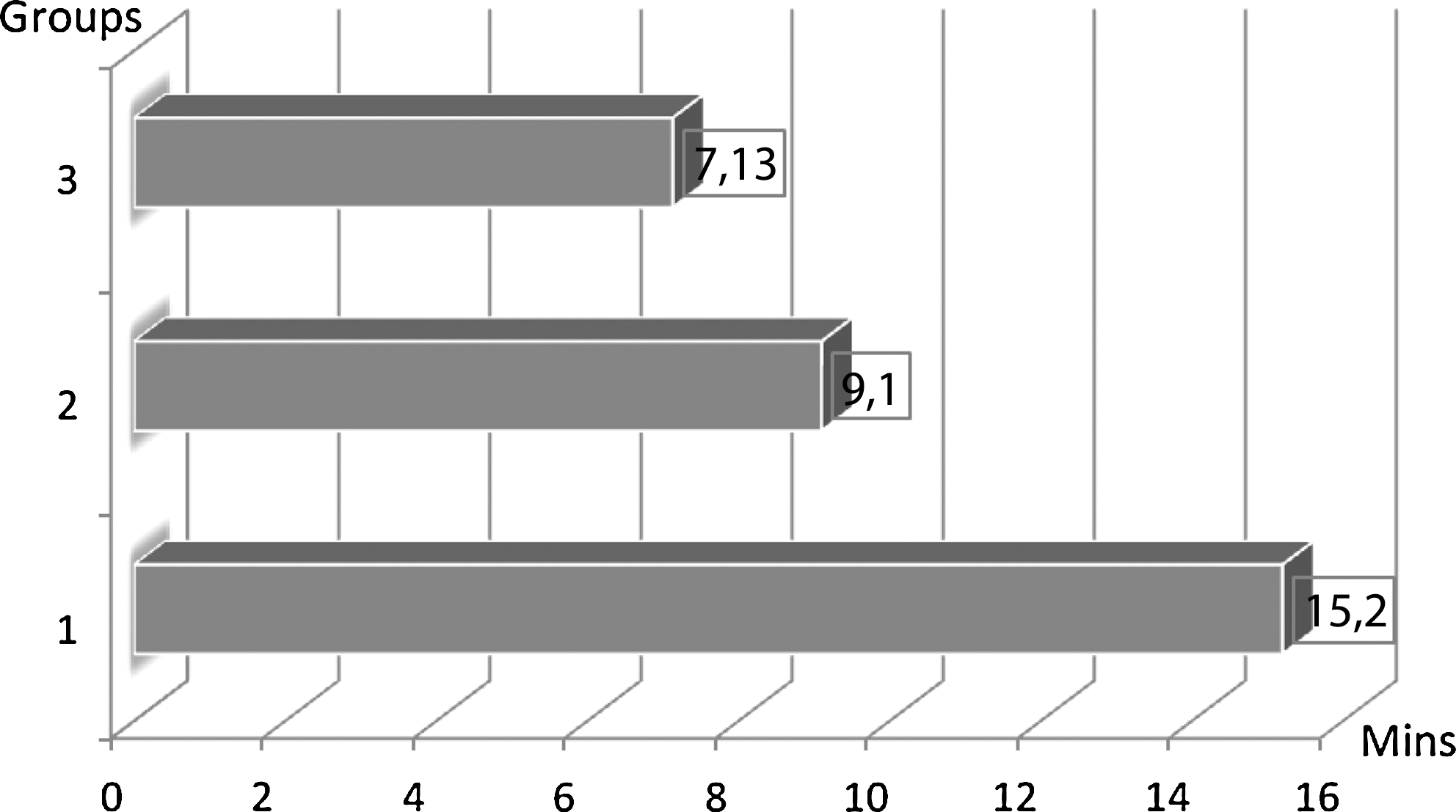
Suturation times of groups 1, 2, and 3.
Mean leak pressures of groups 1, 2, and 3 were 10.4, 14.4, and 19.5 cm H2O, respectively, and the difference between the groups was statistically significant (P<0.05) (Table 1). Only three of the bladders in group 1 leaked under the physiologic filling pressure in humans—specifically, 10 cm H2O. All bladders in group 2 and group 3 remained watertight under 10 cm H2O bladder pressure. Mean bladder capacity at the time of leakage was 276.2, 353.8, and 419.7 mL for groups 1, 2, and 3, respectively, and the difference was statistically significant (P<0.05) (Table 1).
Discussion
In urology, a watertight bladder closure is considered the optimal technique and is a standard part of many urologic laparoscopic operations. 1 –5 Bladder closure can be performed successfully during laparoscopy regardless of whether a cystotomy was performed intentionally for simple prostatectomy or for diverticulectomy, 1,4 or if the bladder injury was incidental. 18,19 Commonly, the preferred suture material is polyglactin, and the preferred technique is interrupted sutures or running suture with intracorporeal knots. 1,4
In recent years, a new barbed polyglyconate suture material has been introduced into the urologist's armamentarium and has been applied successfully in diverse reconstructive procedures. 9 –11,13,20 We investigated the efficacy of running barbed sutures for laparoscopic closures of bladder defects and compared it with polyglactin sutures in running and interrupted fashions with intracorporeal knots sutures. Sotelo and associates 1 reported the successful closing of a transverse cystotomy incision after laparoscopic retropubic simple prostatectomy in a watertight manner with running polyglactin sutures. Nezhat and colleagues 18 reported similar results when using multiple interrupted polyglactin sutures for the laparoscopic closure of bladder lacerations. Tewari and coworkers 9 demonstrated that the barbed suture effectively joins together the bladder and urethra during urethrovesical anastomosis (UVA).
We could effectively close the bladder defects in the three groups. Nonetheless, there was a statistically significant difference between the leaking pressures in the three groups (P<0.05).
In adult humans, the normal bladder capacity is in the range of 300 to 500 mL, and the bladder has a constant low pressure during the filling phase that usually does not reach more than 6 to 10 cm H2O. 17 The pig bladder model is proven as an excellent approximation of the human bladder in many filling-pressure studies. 21,22
Mean bladder pressure at the time of leakage in the polyglactin 910 interrupted (group 1) and running (group 2) suture groups were 10.4 and 14.4 cm H2O, respectively, while that of the barbed polyglyconate group (group 3) was 19.5 cm H2O. Although these data were above the filling pressure of the human bladder, they can be accepted as effective watertight bladder closures.
In addition, we observed that laparoscopic bladder closure using running polyglyconate barbed sutures is very effective during higher bladder pressures reaching 25 cm H2O. This might be because of optimal tissue approximation, with minimal tension and grasping of the bladder wall by the barbs at numerous points, resulting in equal transmission of tension across the wound.
Laparoscopic intracorporeal suturing and knot tying are now considered essential technical skills for laparoscopic surgery, but remain as technical challenges for novice and veteran laparoscopic surgeons. The studies in this field reflect investigation of novel concepts in suture fashion and ligation to simplify the technique and minimize the operative time. 6 –8,23 Obviously, knot tying is time consuming, but suturing time can be decreased by eliminating the need to tie knots. Barbed sutures have a looped end that makes the first knot needless and overcomes the problems of intracorporeal knot tying. 9,10,12 A faster, easier, and more effective bladder closing would undoubtedly facilitate laparoscopic bladder closure.
Previous animal studies have demonstrated that barbed sutures are effective for closing the collection system and renal parenchyma during laparoscopic partial nephrectomy, and for closing gastrointestinal enterotomies, reducing the time needed for suturing. 12,24,25 Williams and colleagues 10 and Tewari and associates 9 have used the barbed suture to perform UVA after robot-assisted radical prostatectomy and demonstrated that UVA using knotless barbed sutures was faster. Warner and Gutowski 26 report similar results for performing abdominoplasty, as does Alessandri and coworkers 20 for performing laparoscopic myomectomy in humans.
Our results are concordant with previous studies, and suturing times were comparable with similar tasks in previous studies performed by the surgeons with a high experience level. 6,14 We demonstrate that the time needed for completion of bladder closure with polyglyconate barbed suture in a running fashion without knot tying (group 3) was significantly decreased when compared with polyglactin 910 sutures in a interrupted or running fashion with knot tying (group 1 and group 2) (Fig. 2).
Another important issue is represented by iatrogenic bladder injuries, which are potential complications during laparoscopic gynecologic, urologic, and general surgery operations. It is highly desirable to recognize and to repair these injuries laparoscopically during the same procedure. 4,18,27 In the literature, the authors preferred a running one-layer 3-0 polyglactin suture and experienced good results. Our study is concordant with the literature in that the running 3-0 polyglactin sutures are effective below the maximal pressure of the human bladder during the filling phase.
Another interesting point is that iatrogenic bladder injuries occur mostly during the training of new laparoscopic surgeons, because a laparoscopic closure may be technically challenging, especially for those with limited intracorporeal knot tying experience. 28 A bladder closure using a barbed polyglyconate suture without knot tying in such situations may be advantageous and would require less time. The mean bladder suturation time with barbed polyglyconate group (group 3) was statistically shorter (P<0.05) than suturation times with polyglactin 910 groups in an interrupted and running fashion (Fig. 2).
Weld and coworkers 25 applied barbed suture for laparoscopic urinary tract reconstructions in pigs, and they have found that the barbed sutures produced a greater degree of fibrotic reaction after bladder neck anastomoses. The authors have claimed that fibrosis might be caused by the relatively traumatic mechanism of tissue gripping and the barbs could theoretically produce focal areas of ischemia. The clinical significance of these pathologic changes is still unproven, however. Our results encourage application of the barbed polyglyconate suture material for closure of bladder defects. Further in-vivo animal studies will be useful to define the role of barbed suture material for closure of bladder defects, and we are currently investigating in a fallowing study in an in-vivo pig model the wound healing of the bladder with the barbed suture material.
A potential disadvantage of the barbed polyglyconate suture is the cost. The barbed polyglyconate is approximately five-fold more expensive than polyglactin 910 suture material. 10 The cost can be negligible, however, considering the advantages of affectivity, safety, and ease and speed of handling, especially in stressful situations, such as iatrogenic bladder injuries.
The limitations of the study might be the in-vitro study design and the not very high prediction power of the used statistical test. However, this is a pilot study, and demonstrates for the first time laparoscopic knotless closure of bladder defects using barbed polyglyconate sutures.
Conclusion
For the first time, an experimental in-vitro pilot study demonstrates laparoscopic knotless closure of bladder defects using barbed polyglyconate suture material. The material and method were feasible, easy, and safe in an in-vitro pig bladder model. Closing the pig bladder with running knotless barbed polyglyconate suture provides a more effective and faster watertight bladder closure than traditional polyglactin 910 suture material. In addition, it improves the time for suturing, even in expert hands. This type of suture may be particularly useful for surgeons with less experience in laparoscopic surgery and in intracorporeal knot tying.
Footnotes
Disclosure Statement
No competing financial interests exist.