
Abstract
Background and Purpose:
Open nephroureterectomy (ONU) rather than laparoscopic nephroureterectomy (LNU) is still regarded as the standard of care for extirpative surgical management of upper urinary tract urothelial-cell carcinoma (UUT-UCC). The longest published follow-up of LNU is 7 years. We report outcomes for patients having surgery ≥10 years ago.
Patients and Methods:
Consecutive patients with UUT-UCC who were treated with ONU (n=39) or LNU (n=23) between April 1992 to September 2000 were included. Preoperative, tumor, operative and postoperative characteristics, recurrence, and outcomes were collated. Survival was estimated using the Kaplan-Meier method.
Results:
Median follow-up of censored patients was 163 months (13.6 y). Estimated mean overall survival (OS) was 111 months for ONU and 103 months for LNU. Mean progression free survival (PFS) was 175 months for ONU and 143 months for LNU. Probability of PFS at 10 years was 79% for ONU and 76% for LNU and was unchanged at 15 years. There was no significant difference between ONU and LNU in terms of OS (P=0.51, log-rank test), PFS (P=0.70) or cancer-specific survival (CSS; P=0.43). There were no prognostic differences between ONU and LNU after correcting for confounding variables. There was no increase in the probability of a bladder cancer recurrence from 10 to 15 years postoperation.
Conclusion:
Long-term follow-up of patients who were operated on more than 10 years ago suggests that LNU has oncologic equivalence to ONU because there were no significant differences in OS, PFS, or CSS between ONU and LNU patients followed for a median of 13 years.
Introduction
Concordant with other laparoscopic operations, LNU has been shown across multiple institutions to offer a superior morbidity profile to ONU. 4 LNU outcome data over the short-to-medium term have been promising; there is now extensive evidence that shows comparable outcome of LNU with ONU up to a median of 5.7 years postoperation (Table 1 shows relevant studies performed over the last 5 years). In addition, studies that assess oncologic outcomes of LNU alone have been published with 7-year median follow-up. Several large studies have been completed, including two multicenter studies with more than 1000 patients 5,6 ; however, before LNU can be accepted as the gold standard treatment option for UUT-UCC, information on long-term efficacy is needed.
ONU=open nephroureterectomy; LNU=laparoscopic nephroureterectomy; CSS=cancer–specific survival; N/A=not applicable; NS=not significant; PFS=progression–free survival.
As such, the aim of this study was to compare the long-term oncologic outcomes of patients who were undergoing ONU or LNU in a cohort of patients having surgery a minimum of 10 years ago.
Patients and Methods
To have a minimum follow-up period of 10 years, patients who underwent ONU (n=39) or LNU (n=23) for clinically localized UUT-UCC between April 1992 and September 2000 at the department of urology, Western General Hospital, in Edinburgh were included in the analysis. All LNU procedures were performed by one surgeon (DAT). ONUs were performed by six different surgeons. Patients with tumors of the upper ureter or renal pelvis and calices had initial transurethral resection of the intramural ureter. LNU was performed using a transperitoneal approach.
The initial laparoscopic dissection in patients with tumors in the renal pelvis or upper ureter was similar to that of a routine laparoscopic radical nephrectomy, with early identification of the ureter, which was clipped in continuity with Ligaclips (Ethicon Endo-surgery Inc, Cincinnati, OH) before mobilization of the kidney. The ureter was mobilized into the pelvis beyond the bifurcation of the common iliac artery and down to the resected end at the bladder wall. The specimen was then removed intact in an impermeable laparoscopic entrapment bag.
Patients with tumors of the distal ureter were treated with initial laparoscopic mobilization of the kidney and ureter into the pelvis, followed by formal open cystotomy, and combined extra- and transvesical dissection to mobilize the distal ureter and remove the kidney, ureter, and bladder cuff en bloc. Other than minor technical adjustments, LNU technique and management of the distal ureter did not change during the duration of the study.
Patients who were undergoing ONU had preliminary mobilization of the kidney and proximal ureter followed by extra- or transvesical mobilization of the lower ureter and bladder cuff, depending on tumor location and surgeon preference. A formal lymphadenectomy was not performed in either ONU or LNU.
Hospital medical records were retrospectively reviewed to assess preoperative staging, postoperative course, pathology (as per World Health Organization classification of 1973), follow-up, disease recurrence, death, and cause of death. If causes of death were not available in clinical notes, they were obtained from death certificates from the General Registry Office of Scotland. Postoperative complications were recorded using the Clavien-Dindo classification. 7 The follow-up protocol was similar across the entire period of the study and consisted of history, examination, urinary cytology, cystoscopic evaluation of bladder, radiographic imaging of the upper urinary tract, and chest radiography, CT, or MRI when indicated.
Follow-up took place at 3 months postoperation, then at 6-month intervals for 2 years and annually following this. The last follow-up date was considered as the last time there was upper tract imaging conducted in disease-free patients or date of death in patients with a known recurrence. Length of follow-up was determined by the time between surgery and the most recent clinical contact.
Disease recurrence was defined as UCC recurrence in the operative site, regional lymph nodes, or distant metastasis. UUT-UCC development in the contralateral collecting system was not included as recurrence after the original surgery and was analyzed separately. From the date of disease recurrence, progression-free survival (PFS) duration could be calculated. Cancer-specific survival (CSS) was determined if the cause of death was directly attributable to UUT-UCC (including contralateral UUT-UCC) according to clinical notes or death certificates. Because of the high frequency of bladder recurrence in patients with UUT-UCC, intravesical recurrence was considered separately. Bladder recurrence was diagnosed by cystoscopy and subsequent histologic confirmation.
Continuous variables were compared using an unpaired t test and, categorical variables were analyzed using the chi-square test or Fisher exact test. PFS, CSS, overall survival (OS), and bladder cancer recurrence-free rate were estimated using the Kaplan-Meier method. The Cox proportional hazards model was used to correct for potentially confounding factors. Statistical analysis was performed using PASW version 18.0 (SPSS Inc., Chicago, IL), P<0.05 was taken to indicate significance.
Results
Table 2 outlines the characteristics of the 62 patients who were included in this analysis. Other than tumor location, there were no significant differences between ONU and LNU in terms of patient, tumor, or operative characteristics. There were a significantly greater number of patients with ureteral tumors who underwent ONU, whereas, there were a significantly higher proportion of patients with renal pelvis tumors who underwent LNU. There were three laparoscopic conversions: one for a vascular injury and two because of failure to progress. The converted LNU cases were included in the LNU group because the analysis was undertaken on an intention to treat basis. There was a significantly shorter hospital stay after LNU compared with ONU (P=0.003, unpaired t test).
ONU=open nephroureterectomy; LNU=laparoscopic nephroureterectomy; N/A=not applicable.
Overall median follow-up of censored patients for OS (ie, were still alive at the last follow-up) was 163 months (13.6 years). The median length of follow-up for censored ONU patients was 177 months and 146 months for LNU. The follow-up of patients in this cohort extends up to 18 years.
Figure 1 and Table 3 outline the OS of the cohort as estimated by the Kaplan-Meier method. There was no significant difference in OS (P=0.51, log-rank test) between LNU and ONU using Kaplan-Meier estimation. Estimated median OS was 109 months for ONU and 122 months LNU. OS at 10 years was estimated to be 56% for LNU and 48% for ONU and at 15 years was 11% and 34%, respectively. Figure 2 and Table 3 detail the PFS of LNU vs ONU; there was no significant difference between the two operative approaches (P=0.70, log-rank test). After the use of the Cox proportional hazards model to adjust for confounding factors, there remained no significant difference in PFS between ONU and LNU. The estimated mean PFS was 174 months for ONU and 143 months for LNU. Estimated PFS at 5 years was 76% for LNU and 79% for ONU; the PFS remained unchanged at 10 and 15 years postoperation.
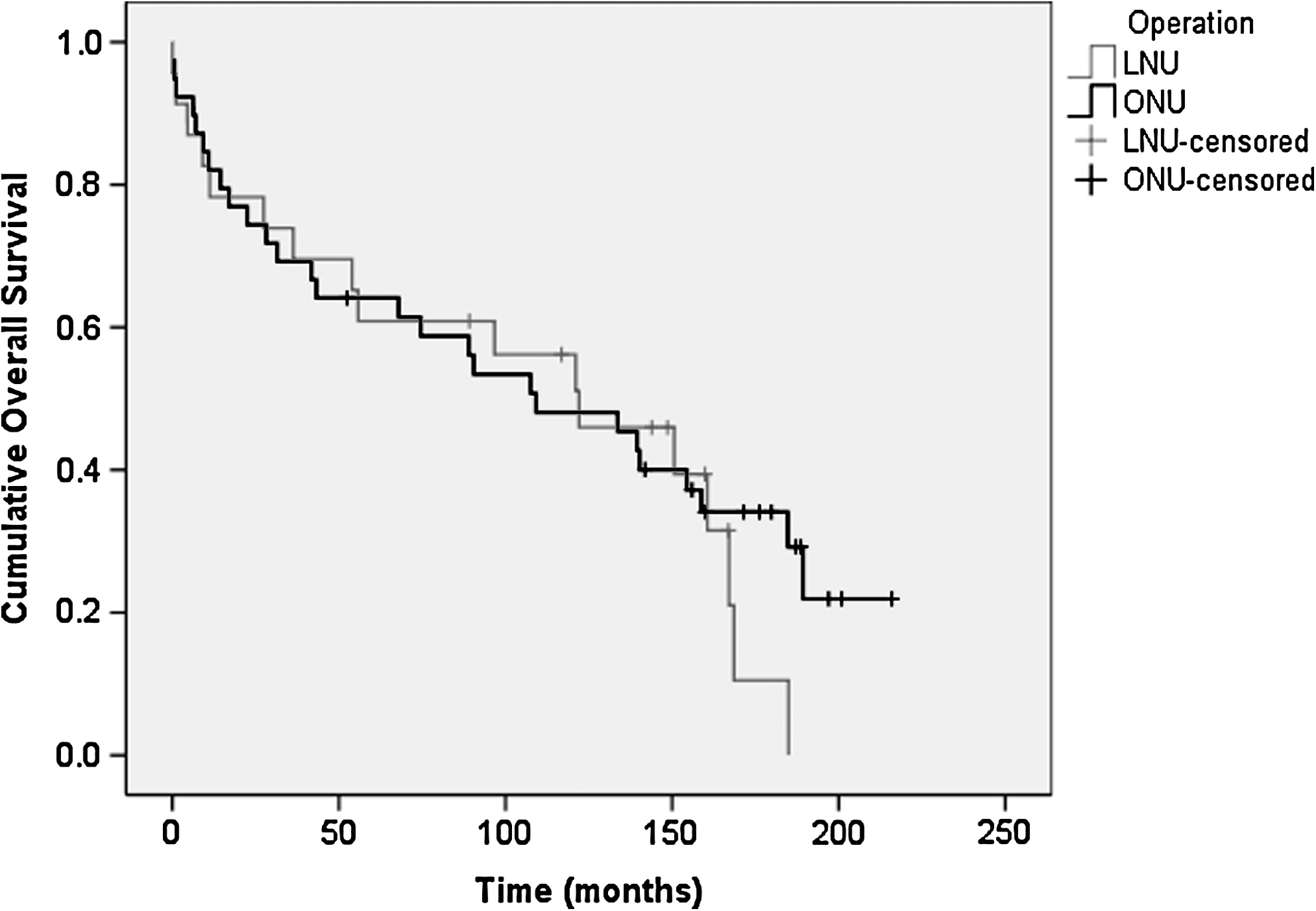
Overall survival for laparoscopic nephroureterectomy (LNU) and open nephroureterectomy (ONU) estimated using the Kaplan-Meier method, P=0.51 (log-rank test).
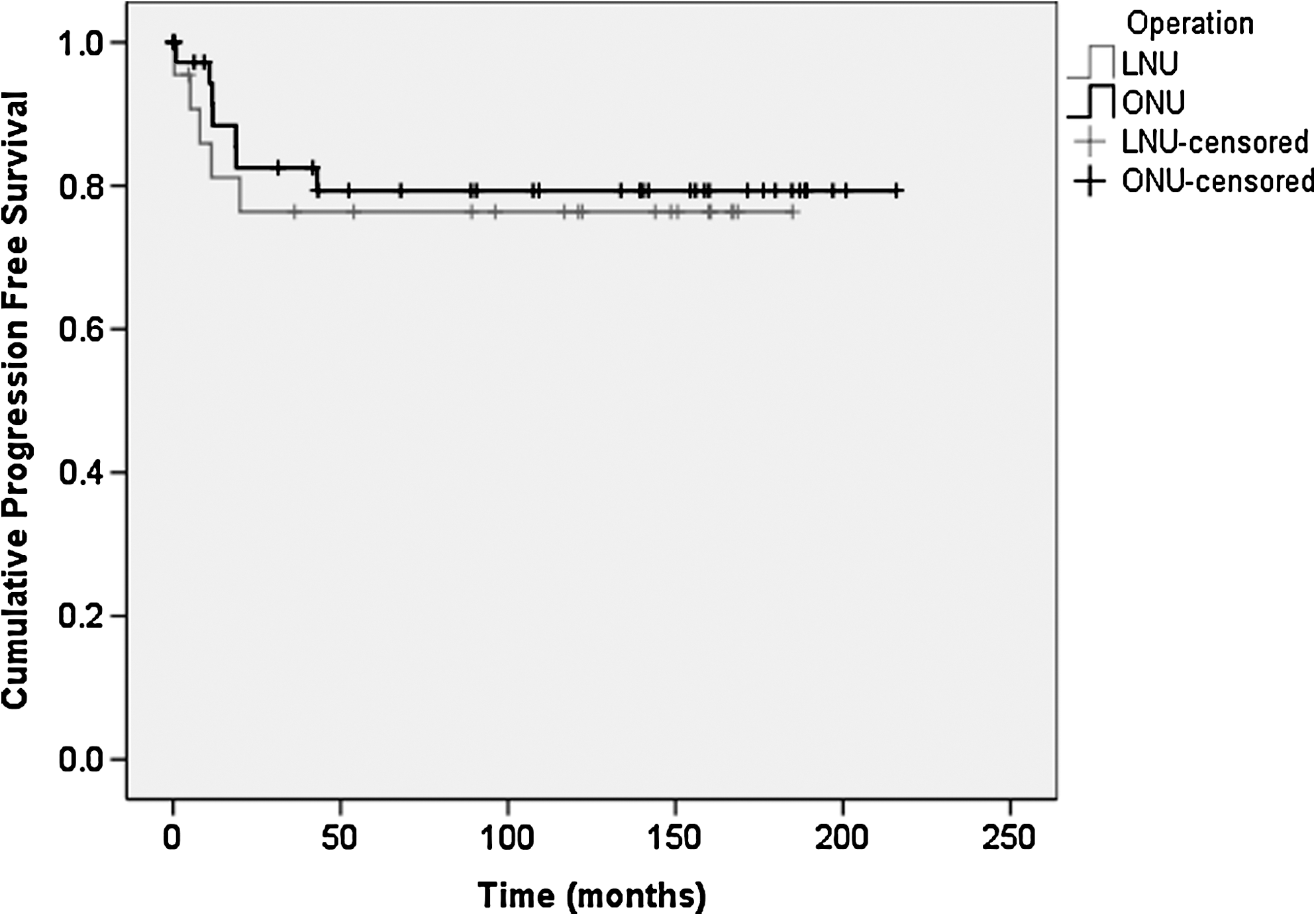
Progression-free survival comparing laparoscopic nephroureterectomy (LNU) and open nephroureterectomy (ONU) as estimated by the Kaplan-Meier method, P=0.70 (log-rank test).
OS=overall survival; LNU=laparoscopic nephroureterectoy; ONU=open nephroureterectomy; PFS=progression-free survival; N/A=not applicable; CSS=cancer-specific survival; bladder cancer=bladder cancer recurrence-free survival.
Figure 3 and Table 3 detail the estimated CSS of the cohort; there was no significant difference in CSS between ONU and LNU (P=0.43, log-rank test). The Cox proportional hazards model was used to adjust for confounding factors, and there remained no significant difference in CSS between ONU and LNU. Mean CSS was estimated at 172 months for ONU and 134 months for LNU. Probability of CSS at 10 years was 71% for LNU and 80% for ONU and at 15 years was 64% and 74%, respectively.

Cancer-specific survival for laparoscopic nephroureterectomy (LNU) and open nephroureterectomy (ONU) estimated using the Kaplan-Meier method, P=0.43 (log-rank test).
In summary, 15 patients in the cohort died as a result of UUT-UCC. There were eight UUT-UCC related deaths in the ONU group (21%): One patient with UCC in the contralateral ureter, four patients with liver metastases, one patient with lung metastasis, one patient with spine metastasis, and one patient with groin metastasis. In the LNU group, there were seven (30%) cancer-specific deaths: Two patients with UCC in the contralateral ureter; one patient with recurrence in the course of the resected ureter; one patient with bone metastasis; one patient with small bowel metastasis; one patient with widespread recurrences in the ipsilateral renal bed, liver, and lungs; and one patient with death recorded as secondary to metastatic UCC, location not noted.
Bladder recurrence-free survival was analyzed separately; there were 9 (39%) bladder cancer recurrences in the LNU group and 15 (39%) in the ONU group. There was one LNU patient with a preoperative bladder cancer; this bladder tumor reoccurred post-LNU. There were four ONU patients who had bladder cancer pre-ONU; none of these patients had vesical recurrence post-ONU.
Figure 4 and Table 3 detail the bladder cancer recurrence-free survival. Estimated mean time to development of bladder cancer recurrence was 103 months in the LNU group and 126 months in the ONU group (P=0.90). Probability of being bladder cancer recurrence-free at 5 years was 55% for LNU and 58% for ONU. Estimated bladder cancer recurrence-free rate at 10 years was 52% for ONU and 48% for LNU. There was no change in the probability of a bladder cancer recurrence from 10 to 15 years postoperation.

Bladder cancer recurrence-free survival for laparoscopic nephroureterectomy (LNU) and open nephroureterectomy (ONU) estimated by the Kaplan-Meier method, P=0.90 (log-rank test).
Discussion
Studies with long-term oncologic follow-up are essential before LNU can be considered equivalent to ONU. To date, oncologic outcome data have been too immature to make any claims about long-term oncologic equivalence of LNU with ONU. UUT-UCC disseminates readily, and there has been concern that LNU may potentiate such spread. The current study illustrates long-term follow-up data, from patients operated on more than 10 years ago, which suggests that LNU has oncologic equivalence to ONU because there was no significant difference in OS, PFS, or CSS between patients having LNU or ONU followed for ≤18 years. Furthermore, if an intravesical recurrence has not been identified by the 10-year follow-up time point, it is unlikely to develop. As far as we are aware, the comparison of oncologic outcomes from LNU vs ONU treatment of patients with UUT-UCC presented here has the longest follow-up of any published series, with a median of 13.6 years follow-up in censored patients.
There are a number of strengths of the study presented here. First, one surgeon performed all LNUs, and all ONUs were performed in the same center by surgeons using a uniform approach. Second, consecutive patients with complete follow-up information have been analyzed. Third, a uniform follow-up protocol has been followed in these patients.
A limitation of this series is the inclusion of relatively few patients in each operative group. The rarity of UUT-UCC, however, means that the number of patients in this study is comparable with that of most other single center studies. We have continued to perform LNU in our department. To date, we have performed approximately 120 cases over an 18-year period. This rate of six to seven cases per year demonstrate that it is unlikely that even in a tertiary referral center, high numbers of cases will be accrued to allow well-powered comparisons.
Capitanio and associates 5 were able to perform a multicenter comparison of ONU and LNU including 1249 patients (270 LNU patients), but this required recruitment of 13 centers from nine countries on three continents. Likewise, Kamihira and colleagues 6 recruited 1002 UUT-UCC patients having LNU, but this was across 51 different Japanese centers. These two multicenter studies demonstrate how challenging it is to identify high numbers of patients from individual centers. It is also recognized that the LNU cases included in this study incorporate the learning curve of the surgeon performing them. Despite the inclusion of a learning curve, however, there was no statistical difference between LNU and ONU; one would expect that patients operated on once the learning curve has been overcome will have a superior outcome.
The two operative approach cohorts were well matched, other than a different distribution of tumor location between the ONU and LNU groups. In particular, there was a greater proportion of lower ureteral tumors in the ONU group. Some single-center studies have found that UUT-UCC tumor location had a prognostic effect 8,9 ; however, we analyzed the effect of location on PFS, CSS, and bladder cancer recurrence rate and found no significant difference (P<0.05, log rank test). A recent multicenter analysis by Raman and coworkers 10 that compared survival of 1249 patients based on UUT-UCC location also found no significant effect on survival.
The distribution of grade and stage of the cancer was equivalent between ONU and LNU patients, unlike some other studies comparing LNU and ONU, in which there were more favorable pathologic characteristics for the LNU group. 5 In the study presented here, 57% of the LNU group had a tumor determined to be grade 3, compared with 39% of the ONU group. Muntener and colleagues 11 had a proportion of high grade tumors similar to that of the current study, perhaps explaining the similarity of the 5-year CSS for LNU found by the Muntener group (68%) to that identified in the current study (71%). Pathologic factors have consistently been shown to have an effect on CSS. 6,12,13 Grade (P≤0.008 log rank test) and stage (P<0.0005, log rank test) were the only two variables included in our study that had a significant effect on PFS and CSS.
The estimated 5-year CSS for LNU of 71% presented here is comparable with previous studies, which range from 68% to 95% (Table 1). As far as we are aware, there are no data with which to compare the 10-year CSS for LNU of 71% nor the estimated 15-year CSS of 64% presented here. The 10-year results for LNU presented above, however, are comparable to previous ONU reports. A series of 92 ONU patients followed up by Charbit and associates 14 reported 10-year CSS after ONU as 65%.
The 5- and 10-year bladder recurrence-free survival for LNU was 55% and 48%, respectively. The 5-year bladder cancer recurrence-free survival is comparable with that of other LNU studies; the Japanese multicenter study reported a 57% bladder cancer free survival at 5 years. 6 The data presented above show that beyond 10 years postnephroureterectomy, there were no further new intravesical lesions identified, suggesting that if a bladder lesion has not been identified by this point in the follow-up, it is unlikely to do so.
Long-term oncologic outcome in terms of PFS, CSS, and bladder recurrence is equivalent between ONU and LNU. The results of this study help to confirm that we have now reached a stage where LNU can be recommended as the first choice for UUT-UCC necessitating extirpative treatment. Ideally, a randomized controlled trial (RCT) should be undertaken to confirm the findings of this study. It is unlikely that a RCT will be performed, because LNU is well established in most major urology units, and UUT-UCCs are relatively rare tumors, making trial recruitment rate a potential issue. In the absence of a RCT, a meta-analysis of studies with prolonged follow-up such as that presented here should be conducted to obtain results with satisfactory statistical power.
Footnotes
Disclosure Statement
No competing financial interests exist.