
Abstract

In our institution, which is a tertiary referral center for renal stone disease, we, too, make a great effort to minimize patient radiation exposure. When performing PCNL, we access the caliceal system using combined ultrasonography and fluoroscopy guidance in a bid to reduce radiation dose to the patient.
The use of room air to perform retrograde pyelography is interesting, yet we would postulate the role is limited to that described. In our institution, we sometimes perform retrograde magnetic resonance urography (MRU) in patients in whom we are keen to restrict radiation exposure.
The technique involves the injection of dilute gadolinium (0.1 mmol per 10 mL 0.9% saline) through a retrograde catheter placed in the standard fashion. Multiple temporal MRU phases are acquired with repeated contrast injection as needed to distend the renal pelvis and to image the entire ureter. We use a thick slab T1 FLASH (fast low angle shot)—TR 3.8, TE 1.160, ST 2 mm, Matrix 256×256) sequence in the coronal plane with maximal intensity projection reconstructions and using a phase array surface coil.
The advantages of this technique include the lack of ionizing radiation, the ability to perform multiplanar imaging on any abnormalities detected, and the detection of ancillary findings. Furthermore, we think that the image quality obtained allows confident assessment of the caliceal anatomy and urothelium (Fig. 1).
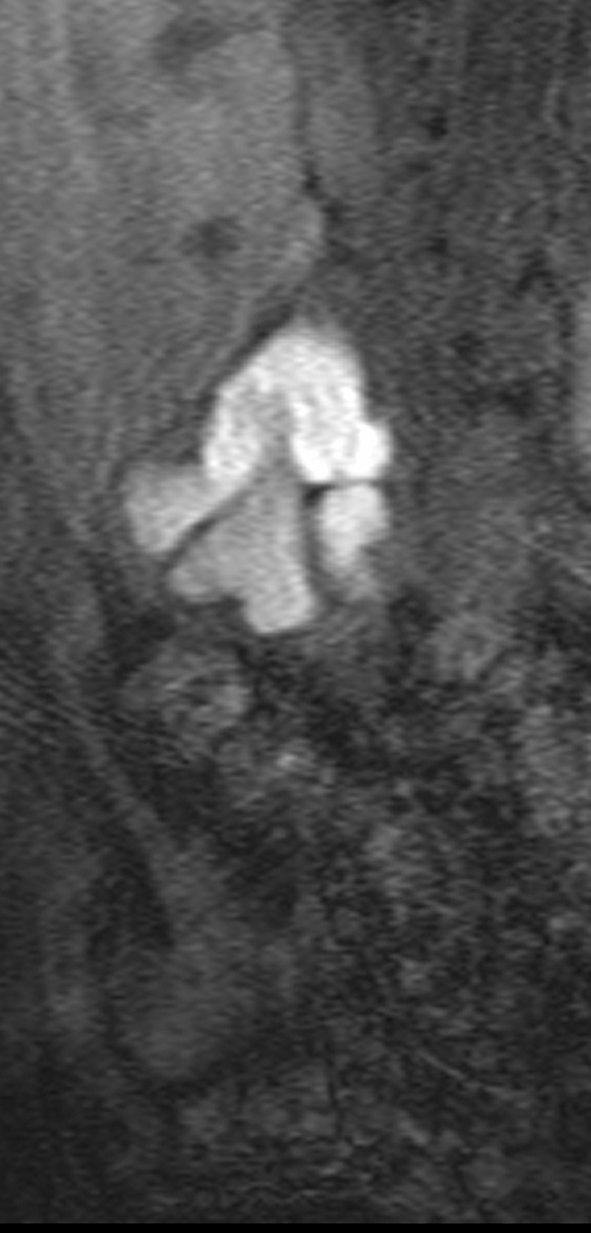
Image from a T1 fast low angle shot (FLASH) magnetic resonance urogram with intraureteral gadolinium. The right kidney is malrotated with caliceal clubbing. Excellent urothelial detail is demonstrated of the lower pole system on T1 FLASH imaging.
We congratulate the authors on a well-written article and on their commitment to reducing patient radiation exposure. We think that our experiences with retrograde MRU complements their work and emphasizes the importance of adapting techniques to reduce patient radiation dose.