
Abstract
Background and Purpose:
Laparoendoscopic single-site (LESS) surgery through the retroperitoneal approach has been seldom reported. We aimed to compare the feasibility and outcomes of LESS and conventional laparoscopic surgery via the retroperitoneal approach in the management of large, impacted ureteral stones.
Patients and Methods:
From June 2010 to May 2011, LESS ureterolithotomy through the retroperitoneal approach was performed in 10 patients (the LESS group). Another 15 patients who underwent conventional retroperitoneal laparoscopic ureterolithotomy (the conventional laparoscopic group) by the same surgeon were involved and compared. The operative time, complications, and surgical outcomes were evaluated.
Results:
All the operations were completed successfully, without conversion to conventional laparoscopic or open surgeries. The operative time of the LESS group and of the conventional laparoscopic group were 132.7±16.3 and 128.1±20.1 minutes, respectively (P=0.782). The estimated blood loss were 30.7±5.9 vs 28.0±4.5 mL (P=0.620). Duration of analgesia postoperatively was 2.0±0.8 vs 3.5±0.5 days (P=0.005). All targeted stones were successfully extracted without major complications. Postoperative urine leakage was noted in one patient in each group. Cosmetic results were superior in the LESS group according to both the study nurse's and the patients' assessments (8.5 vs 5.3; P=0.012, and 8.3 vs 5.6; P=0.025, respectively). All patients showed no obstructions or stricture formations on postoperative follow-up.
Conclusions:
In experienced hands, LESS for ureterolithotomy through the retroperitoneal approach is feasible and can acquire outcomes equal to those of conventional multiport laparoscopic surgery. Prospective long-term follow-up studies with a larger number of patients are needed to further evaluate its benefits.
Introduction
In recent years, laparoendoscopic single-site (LESS) surgery has been developed. It improves cosmesis in the skin by placing all instruments through a 2 to 3 cm incision 4 –6 and has been demonstrated to be feasible and effective in treating ureteral calculi in selected patients. 7,8
Until now, many cases of LESS ureterolithotomies reported were performed through the transperitoneal approach. 9,10 In our practice, however, the preferred approach is retroperitoneal. Although it is not easy to performed complex procedures in the limited retroperitoneal cavity during the surgeon's learning-curve period, the advantages of the retroperitoneal approach in selected patients have been well demonstrated by many recent studies. 11,12 The retroperitoneal pathway has less chance of intraperitoneal contamination by urine leakage or infection, and absence of peritoneal irritation by CO2. It is especially valuable for patients who need to maintain peritoneal integrity or those with an abnormal or obliterated peritoneal space. In experienced hands, both transperitoneal and retroperitoneal approaches are feasible, and the choice depends on personal preference. 13,14
Currently, no studies that compare LESS and conventional ureterolithotomy have been reported. We present our initial experience of retroperitoneal LESS ureterolithotomy in 10 patients and compare the surgical outcomes with those of conventional laparoscopic ureterolithotomy. Meanwhile, tips and tricks applied during the operations to conquer the manipulation difficulties were also introduced.
Patients and Methods
Between June 2010 and May 2011, retroperitoneal LESS ureterolithotomy was performed in 10 patients (the LESS group) in our institute. Fifteen patients who underwent conventional retroperitoneal laparoscopic ureterolithotomy in the same period were involved as the control (the conventional laparoscopic group). The patients were allocated into the two groups randomly with ethical approval. All patients gave appropriate consent. Each patient signed an informed consent document before the operation. All the operations were performed by the same skilled urologist. Preoperative urologic ultrasonography, kidneys-ureters-bladder (KUB) radiography, intravenous urography (IVU), or CT was performed to make the detailed diagonosis of ureteral calculi.
The indications were: Large (the long axis of the stone >15 mm), impacted calculi in the upper or middle part of the ureter. Patients with severe blood coagulation disorder, strictured ureter, abnormal ureteral anatomy, and ipsilateral renal stones were excluded. Detailed characteristics of the patients aree listed in Table 1. In this study, the stones were large and had caused significant obstruction to the ureter segments. Shockwave lithotripsy (SWL) or ureteroscopy (URS) treatments had failed in five patients in each group before laparoscopy treatments. In the traditional laparoscopic group, there were four patients who received URS treatment initially but in whom the treatment failed. They were then treated with SWL without success. The fifth patient received SWL and the treatment similarly failed. Laparoscopic treatment was offered as a salvage procedure to these five patients subsequently. In the LESS group, there are five patients who were treated with URS unsuccessfully; they were then treated with SWL but treatment similarly failed. LESS treatment was also offered as a salvage procedure. There were no significant differences in the preoperative characteristics between the two groups.
P>0.05.
BMI=body mass index.
Patients were placed in the full flank position with flexion under general anesthesia. Skin and fascial incisions (2–3 cm) were made at the site of 3 cm above the iliac crest in the middle axillary line. The retroperitoneal cavity was established by balloon dilation as reported previously. 15
In the LESS group, once the retroperitoneal cavity was established, a homemade multichannel single-port access was inserted (Fig. 1). This device was made by a surgical glove (size 7) and two plastic rings. The bigger ring had a diameter of 7 cm, the smaller ring had a diameter of 3 cm that was fixed at the middle part of the glove. The wrist part of the glove was turned over, the smaller ring was inserted into the retroperitoneal cavity; the bigger ring was left outside and was fixed to the margin of the glove. Two 10-mm conventional trocars and one 5-mm trocar were fixed to the glove fingers, followed by insufflations of the retroperitoneal cavity with CO2 to 13 to 14 mm Hg (1 mmHg=0.133 kPa). A 5-mm, 0-degree lens laparoscope with a flexible tip (Olympus) (Fig. 2a), was inserted through the central 10-mm trocar. Precurved, flexible-articulating graspers and clamps (Cambridge Endoscopic Devices, Framingham, MA; Figs. 2b, 2c) were applied that had flexible joints in the parts of the wrist and the tip. The instruments were helpful in providing efficient retraction for optimizing surgical exposure. No additional ports were used.
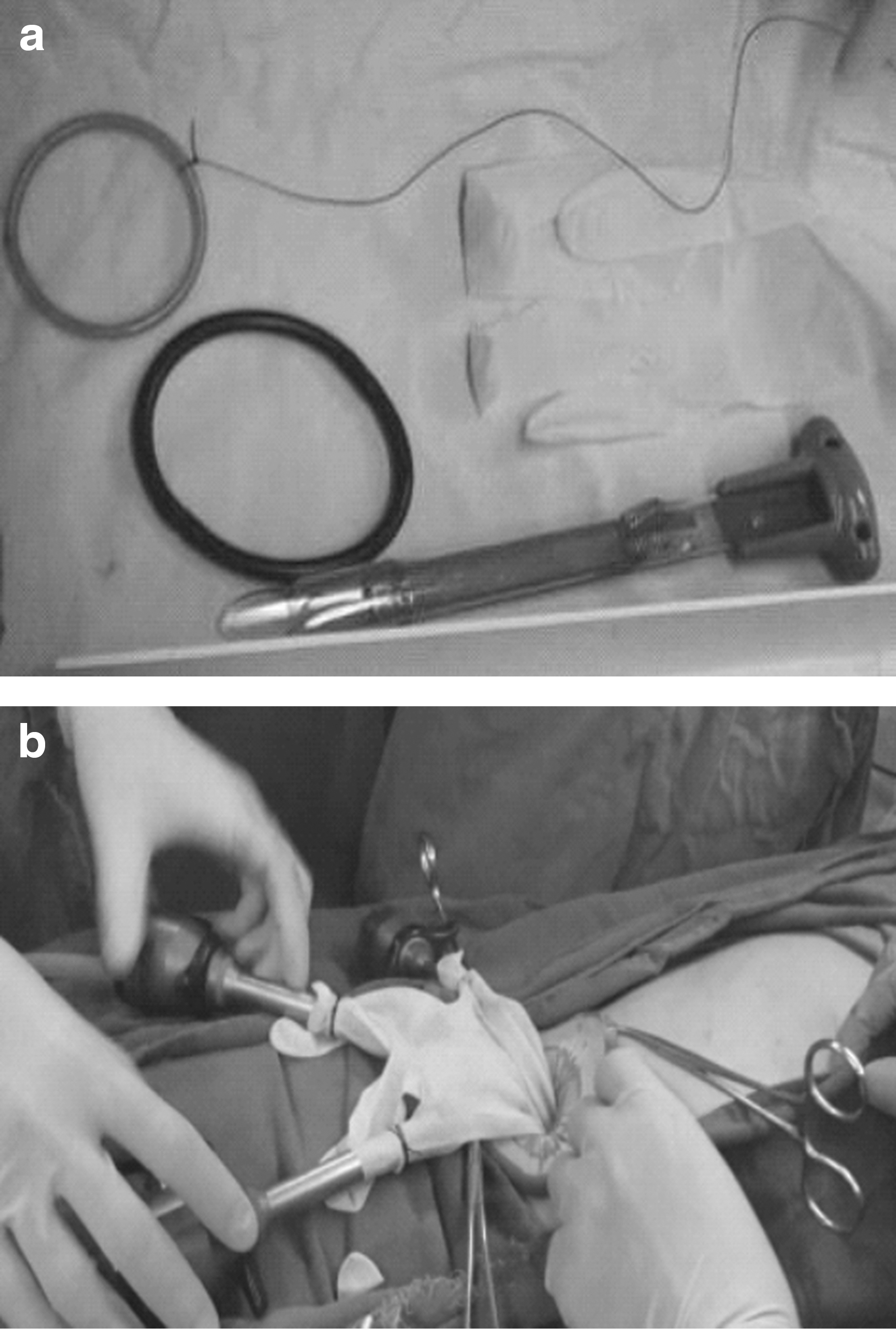
The homemade single-port access device.

Instruments used in the LESS ureterolithotomy.
The ureter was located next to the psoas muscle. 12 The stone was identified by a grasper. In case of severe hydronephrosis in the upper segment of the ureters or in the kidneys, a temporary ureteral clamp, made by a bulldog arterial clamp, was applied as described in our previous report. 15 It was placed at the ureter above the stone to prevent the stone sliding when the calculus was identified. A longitudinal 5 to 10 mm incision was made on the ureter wall over the surface of the stone. After extraction of the stone by the graspers, the clamp was released. When inserting the ureteral stent, the clamp was placed again in the proximal part of the ureter to temporarily block the urine flow (Fig. 3). A tiny guidewire was inserted into the 4.5F Double-J ureteral stent. The stent was placed into the distal part of the ureter with the aid of flexible clamps and grasper; the ureteral clamp was then released; the stent was inserted into the proximal ureteral segment and the renal pelvis. The internal guidewire was removed. When suturing the ureter, the clamp was placed again to block the urine flow.
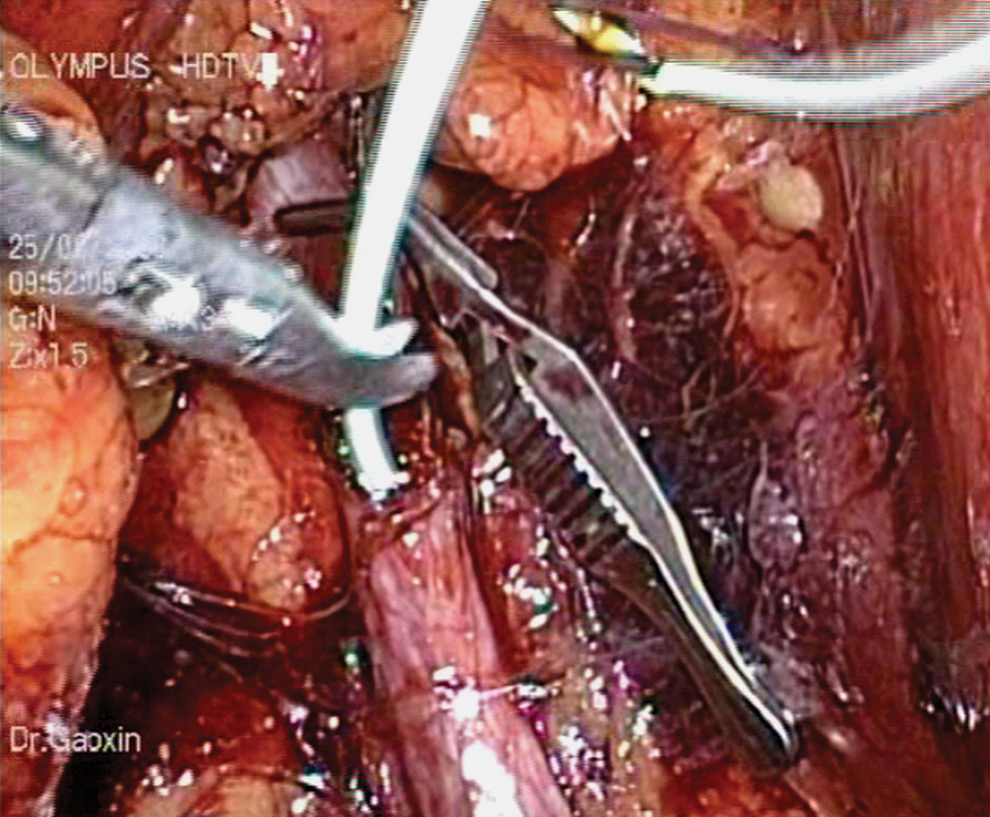
The use of a temporary ureteral clamp can help to fix the stone and block the urine flow, providing a clear operative field while performing the incision, intubation, and suturing of the ureter.
Under a clear operative field without disturbance of urine leakage, the 3-0 absorbable polyglactin was used to place two or three intermittent sutures of the ureter. The two ends of the suture threads were fixed by double Lapro-Clips (United States Surgical, Tyco Healthcare Group) instead of the difficult knot tying (Fig. 4). The stones were removed from the retroperitoneal cavity at the end of the operation.
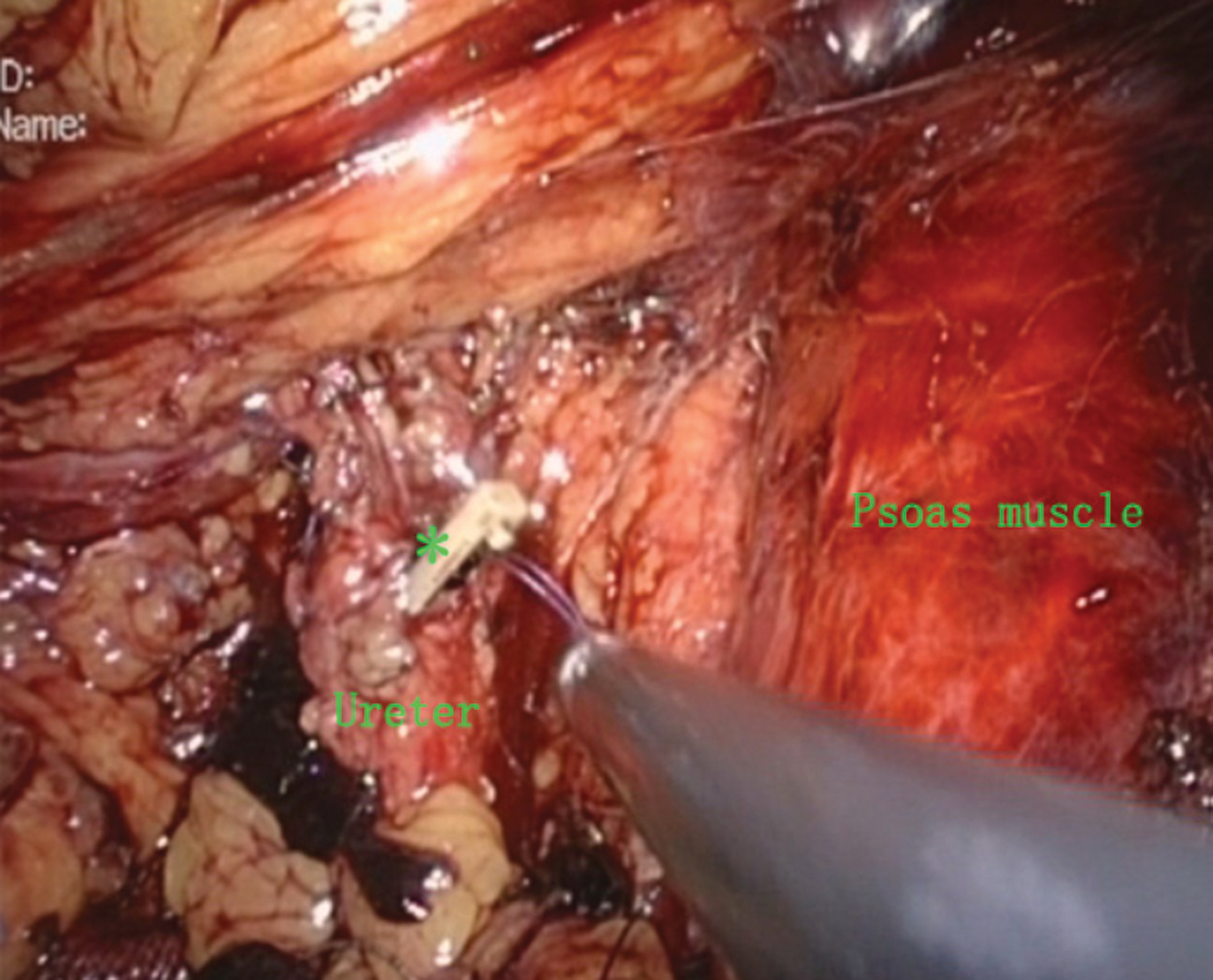
The two ends of the suture threads were fixed by laproscopic clips, instead of the difficult knot tying (*the Lapro-Clip).
In the conventional laparoscopic group, the major procedures such as establishing retroperitoneal cavities, placing trocars, using instruments, extracting stones, and suturing of the ureter were performed as described in our previous report. 15 The ureteral clamp was also applied in selected patients. Traditional knot tying was performed during the suturing procedure.
At the end of the operations, a retroperitoneal drainage tube was placed through the incision, which was removed 1 to 3 days postoperatively when no urinary leakage occurred. The ureteral stent was removed 4 to 6 weeks later.
Postoperative pain control was achieved by patient-controlled analgesia with fentanyl 15 μg/kg
The patients were followed up by using KUB radiography and ultrasonography at the second day and the fourth week postoperatively for stent position and hydronephrosis surveillance. Further follow-up using renal ultrasonography and IVU was performed to check for recurrence and ureteral stricture at the third month after removal of ureteral stents. We monitored ureteral strictures postoperatively by IVU. We also used ultrasonographic examination to monitor the relief degree of hydroureter or hydronephrosis after laproscopic or LESS ureterolithotomy.
Statistical analysis was performed with SPSS 17.0 software. The data were expressed as mean±standard deviation. Independent-samples T test and chi-square test (Fisher exact test) were used. A Wilcoxon rank sum test was used for data not normally distributed and/or ordinal data (cosmesis scores). A P value <0.05 was considered to be statistically significant.
Results
All procedures in both groups were completed successfully, without conversion to open surgeries. No severe intraoperative complications occurred. Postoperative urine leakage was recorded in one case of each group. The difference of postoperative urine leakage rate between the two groups did not reach statistical significance (LESS vs traditional laparoscopy: 1/10 vs 1/15, P=1.000, Fisher exact test). The urine leakage was stopped at the third day in the LESS group and at the fifth day in the conventional group without new intervention. No patient needed blood transfusion. The cosmetic result was better in the LESS group than in the conventional group (Table 2).
Independent-samples T Test, P<0.05.
Patients were followed up for 7.5 months on average (range 2–12 mos) in the LESS group and for 8.2 months on average (range 1–12 mos) in the conventional laparoscopic group. All patients were asymptomatic and had no obstructions or stricture formations on postoperative follow-up.
Discussion
To our knowledge, this is the first study to compare the efficacy and outcomes between the LESS ureterolithotomy with conventional laparoscopic surgery via the retroperitoneal approach, although the sample size is limited. Currently, many cases of LESS ureterolithotomy reported previously were performed through the transperitoneal approach rather than the retroperitoneal pathway. 9,10 Our initial experiences demonstrated that although the retroperitoneal cavity is limited and is difficult for complex procedures during the surgeon's learning-curve period, LESS ureterolithotomy via the retroperitoneal approach can obtain outcomes equal to those of conventional multiport laparoscopy surgery in expert hands.
Traditionally, conventional laparoscopic surgery needs three to six ports for a given procedure, with each port increasing the potential morbidity of bleeding, port site hernia, internal organ damage, and decreasing cosmetic outcomes. 16,17
Recently, as a new step to reduce the invasiveness of standard laparoscopy, 5,6 LESS was introduced and applied in the clinical practice. Only one small incision was needed in this procedure, which has good cosmetic effect in the skin and was welcome by a certain number of patients. LESS has been reported for various kidney and pelvic procedures; initial results showed that it is feasible and effective in selected patients. 5,6
LESS surgery has a unique learning curve, 6 principally because of the difficulty in navigating the instruments within a limited range of motion and the need for significant coordination between the surgeon and the camera holder. Because all the instruments are closely packed together, clashing of instruments and the laparoscope is common. During ureterolithotomy, placing several parallel instruments makes triangulation more difficult, especially when suturing the ureter. Another limitation is lack of additional assistant trocars and effective retraction, which is difficult for inserting the ureteral stents properly.
In this study, we introduced our own experience on conquering the limitation. The application of the flexible and curved instruments can decrease the difficulties of manipulation, reduce instrument crowding, and acquire correct exposition of the structures. In addition, use of the 5-mm, 0-degree lens scope with a flexible tip (Olympus) is suggested. The tip of the flexible scope can be steered to center the surgical field without moving the straight segment, and avoid clashing with the operator's instruments.
The use of a temporary ureteral clamp can help to fix the stone when operating on the ureter. It was also helpful in blocking the urine flow, which provides a clear surgical field while performing the incision, intubation, and suture of the ureter. 15 When inserting the ureteral stent, we use flexible instruments, which makes this procedure easier to perform. It should be noted that the bulldog clamp over the ureter was applied only in selected cases in which there was moderate or severe hydroureter or hydronephrosis. The tension of this clamp is not high enough to cause significant injury to the ureteral wall based on our animal studies and our clinical experience. Moreover, the clamping time was usually less than 10 minutes, which was shorter than the time needed for clamping the renal artery during partial nephrectomies. Moreover, before laparoscopic operations, placing an external ureteral stent may help to locate the ureter more easily, and thus may reduce the difficulty of the laparoscopic and the LESS ureterolithotomy. More practical experience is needed to demonstrate this method.
When suturing the ureters, the two ends of the suture threads were fixed by double Lapro-Clips, instead of the difficult knot tying. In our hands, placing Lapro-Clips is not very difficult or technical demanding. We use 2 or 3 sutures to close the ureteral incison. These clips were placed in parallel with careful adjustments to avoid any compression, damage, or clashing onto the ureter. This operative procedure can be finished quickly with increased experience. This trick had been demonstrated to be feasible and can shorten the operative time significantly.
By using these technical improvements and tricks mentioned above, we acquired satisfactory outcomes compared with other previous reports. 4,7 The average operative time was 132.7 minutes in the LESS group, less than the 155.3 to 176.7 minutes reported. The mean blood loss was 30.7 mL, less than the 37.5 to 101.7 mL reported. 4,7
As described by other reports, 6,14 surgical experience is an important factor for better efficacy of laparoscopy. In this study, the operative time and complication rate in both groups of this study did not differ significantly. The main operator in both groups has skillful experience in laparoscopic operations. This indicates that, in expert hands, LESS ureterolithotomy via the retroperitoneal approach can accomplish outcomes similar to those of conventional laparoscopic procedure.
LESS ureterolithotomy should not be overused. For stones larger than 1 cm in diameter, SWL, retrograde ureteroscopy, and percutaneous antegrade ureteroscopy are all acceptable choices. 1 LESS ureterolithotomy can only be considered to treat patients with difficult, large upper ureteral stones that cannot be adequately managed by SWL or ureteroscopy alone.
Patients who accepted LESS ureterolithotomy in this study have their own unique social-economic background. This article summarized our own experience in treating this kind of patient. In undeveloped areas, sometimes patients presented with moderate or severe hydroureter or hydronephrosis when they were referred to the urologists in tertiary care facilities. To remove these larger stones and to relieve the urinary obstruction in a simple way, invasive surgeries were needed for these patients, especially when SWL or ureteroscopic treatments failed. In these conditions, LESS ureterolithotomy can be considered as a choice that offers significant advantages over traditional open surgery.
In the future, with the development of various single-port devices, flexible laparoscopes, and other instruments, the difficulties in LESS ureterolithotomy can also be reduced. 6 As a new step of laparoscopy, the LESS approach has been applied in various kidney and pelvic procedures. Initial results showed that it was feasible and effective in selected patients. More clinical data are needed to evaluate its long-term effects.
There are several limitations of this study. First, our homemade single-port device could decrease the medical cost and was easily made; however, it is easy to be broken. Meanwhile, gas leakage sometimes occurred. Application of commercial single-port access can get better results. Second, this study only described the short-term outcomes in a small number of patients; results of long-term follow-up and application in a larger population are warranted to further characterize the benefit of this technique.
Conclusions
Retroperitoneal LESS ureterolithotomy can be performed safely with good early surgical outcomes in selected patients with large, impacted ureteral stones. Short-term outcomes in limited cases appear similar to those of conventional laparoscopic ureterolithotomy. Prospective studies based on a larger number of patients are needed to further evaluate its benefits.
Footnotes
Acknowledgments
This study was supported by the Fundamental Research Funds for the Central Universities of China (Sun Yat-sen University, Grant 10ykpy06) and National Natural Science Foundation of China (Grant 81072115, 30872585 and 30901768).
Disclosure Statement
No competing financial interests exist.