
Abstract
Background and Purpose:
Extrinsic ureteral compression challenges a ureteral stent's ability to facilitate urinary drainage and to protect the kidney. Our purpose was to evaluate the performance of new metallic coil-based ureteral stents in terms of tensile strength and radial compression force.
Materials and Methods:
Three stent designs tested from Prosurg Inc included Passage 7.0F, Snake 6.0F, and Snake 7.0F with the straight section covered with a biocompatible polymer tubing. A MTS Microbionix Testing System using Testworks II software, vibration isolation table, and a 5-N load cell were used to measure tensile and compressive strength. Stents were placed in hydraulic grips and stretched at a rate of 5 mm/s for 1 second under uniaxial tension. Extrinsic compression was exerted in 0.1-mm increments to maximum compression. The Young Modulus, E, was calculated from each trial using engineering stress. Data were analyzed using Mann-Whitney and t tests.
Results:
The Passage, Snake 6F, and Snake 7F stents had tensile strengths of 27±3, 5±0.1, and 73±26 kPa, respectively. Mann-Whitney tests show statistically significant difference between stents (P<0.05). Elastic modulus needed to cause extrinsic compression was highest for Snake 6F (145,842±14332 Pa) compared with that of Passage (124,999±3182 Pa) and Snake 7F (126,132±19316 Pa), (P<0.05).
Conclusion:
The Snake 6F stent had the lowest tensile strength and was least resistant to extrinsic compression. The Snake 7F had the highest tensile strength and was most resistant to extrinsic compression. All three stents are more resistant to extrinsic compression than the Applied Silhouette or Cook Resonance, yet have lower tensile strengths.
Introduction
Metal and coil-reinforced stents have evolved over the last decade to combat the challenges that have been encountered with polyurethane Double-J stents, such as extrinsic compression and early occlusion of the lumen from urinary debris or crystals. Examples of these include the Resonance® (Cook Urological, Spencer, IN) coiled metal wire and Silhouette (Applied Medical, Cleveland, OH) coil-reinforced Double-J stent. Animal and clinical studies have shown that the Cook Resonance stent can safely and efficiently resist extrinsic ureteral obstruction. 1,2,4 –6
New stent designs are evolving, looking to gain on the clinical successes seen by metal and coil-reinforced stents. In this study, novel metal stents were tested using in-vitro models for physical characteristics known to differentiate ureteral stents, including coil strength, tensile strength, and resistance to extrinsic compression. 7 –9 Understanding these features can support the selection of the best clinical tool based on known and anticipated clinical performance.
Materials and Methods
The three new stent designs tested were the Passage™ (Prosurg Inc, San Jose, CA) 7.0F metallic coil stent, Snake™ (Prosurg Inc, San Jose, CA) 6.0F gold-plated stainless steel coil stent, and Snake 7.0F gold-plated stainless steel coil stent that includes a biocompatible polymer tubing on the straight portion of the stent. Coil strength was defined as the maximum force needed to pull the proximal coil through artificial tissue (bologna).
An 8-ounce package of Oscar Meyer beef light bologna was frozen, then drilled with holes spaced evenly apart using a 5/64 inch (2-mm diameter) drill bit. All plastic bologna coverings were removed except for a small rim of plastic casing around the peripheral edge of the surfaces, and the bologna was allowed to thaw overnight in a refrigerator. For testing, individual stents were inserted using a guidewire through a bologna hole centered above the gap between two wooden tables (Fig. 1). The proximal coil was allowed to reshape, and then the distal end of the stent was attached to a handheld Force Five™ FDV force gauge that was used to slowly pull the stent through the bologna, which resulted in straightening of the proximal coil. This process was repeated five times for each stent, switching to a new hole in the bologna for different stents. The maximum force reading was recorded for each trial.

Coil strength test.
Next, a MTS Microbionix Testing System using Testworks II software, a vibration isolation table, and a 5-N load cell were used to measure tensile and compressive strength. Stents were placed between clamp and hydraulic grips spaced 19 to 32 cm apart, depending on the length. After preconditioning, stents were stretched at a rate of 5 mm/second for 1 second under uniaxial tension (Fig. 2). The force was allowed to reduce down to zero between tests, with each stent being repositioned after every 4 tests for a total of 12 tests. Extrinsic compression was exerted in 0.1 mm increments (Fig. 3). Cycles of compression and a 15-second hold time were repeated for each stent. Six trials were completed for each stent, with the stent being repositioned after each trial.
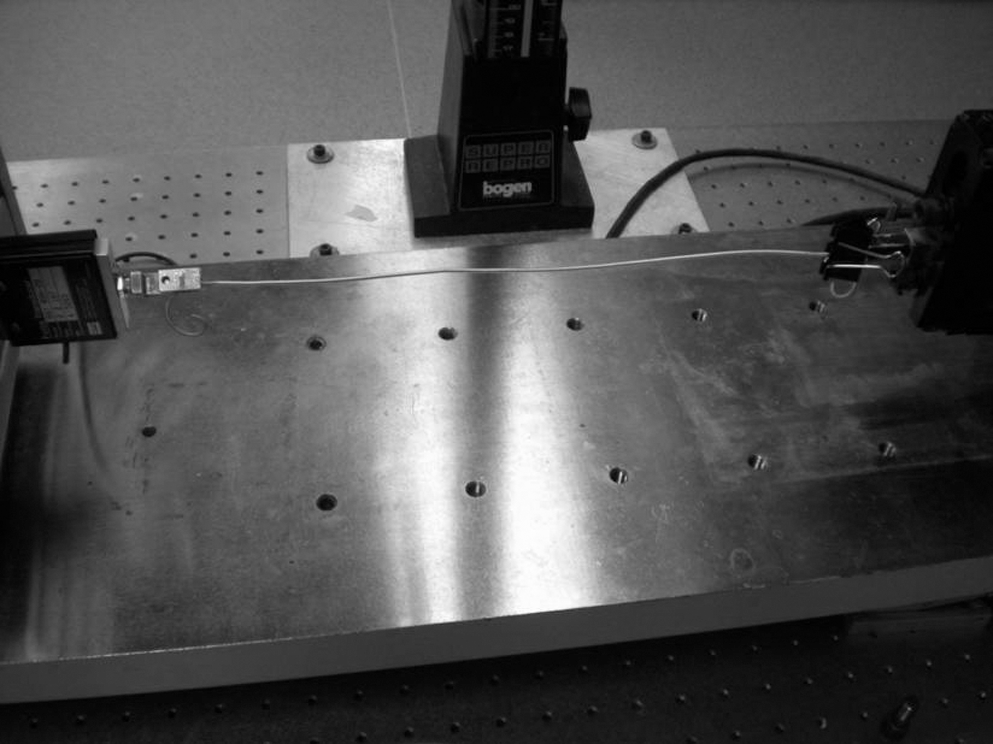
Tensile strength test.
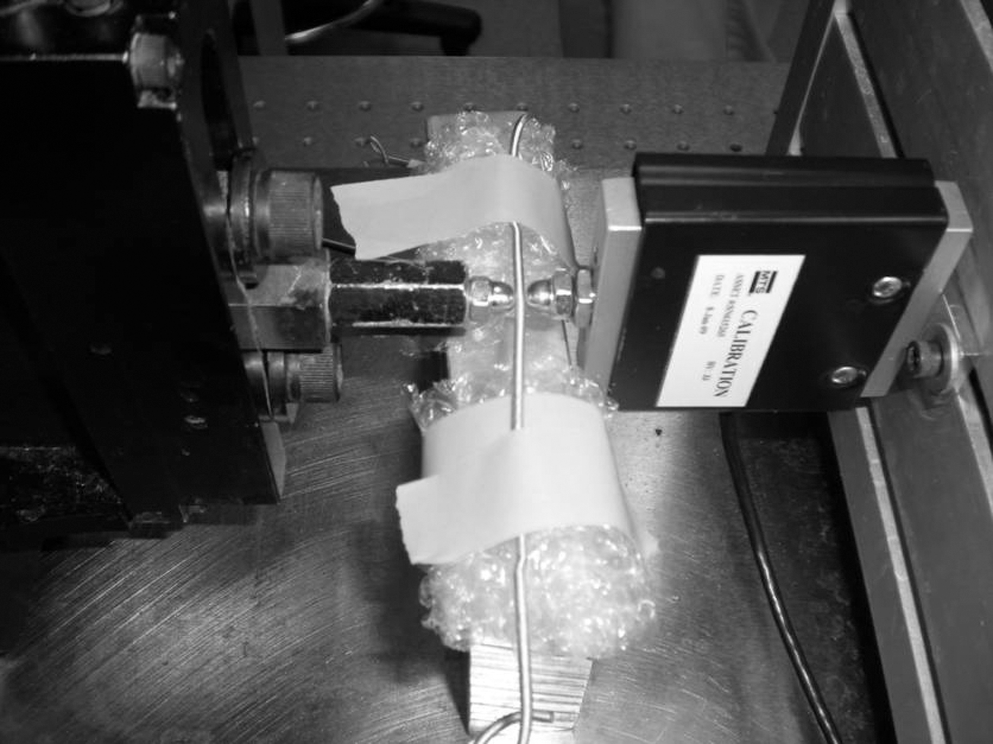
Compression test.
The Young modulus, E, which is the proportionality constant of stress to strain, was calculated for each trial under both tension and compression. E represents the stiffness of the stent. Linear elastic assumptions, infinitesimal strain, and engineering stress were used for all calculations. Comparisons were made with the Cook Resonance and Applied Silhouette, which in previous studies demonstrated greater stiffness and higher resistance to compression than other metal and coil reinforced stents. 8 Based on the number of each stent designs tested, sufficient data points were collected for each testing method for statistical analysis that consisted of analysis of variance, confidence intervals, two-tailed t tests within stent models and Mann-Whitney tests between stent models.
Results
Results for coil strength, tensile strength, and compression are presented in Table 1. Coil strength was similar between all stents (P>0.05). Mann-Whitney tests showed a statistically significant difference between tensile strength of stents (P <<0.05). The Snake 6Fr stent demonstrated the lowest tensile strength followed by the Passage and Snake 7Fr stents. The elastic modulus needed to cause extrinsic compression was highest for the Snake 6Fr stent compared with that of the Passage and Snake 7Fr stents (P=0.01).
P value applies to asterisked compression results.
≪=much less than.
Discussion
The designs of these stents differ from those of existing ureteral metallic and coil-reinforced stents in several ways (Fig. 4). The Passage stent released in 2010 by Prosurg is a metallic coil stent with a spiral winding configuration allowing for flexibility combined with durable radial compression strength. Another new stent also made by Prosurg is the Snake gold-plated metallic spring-coiled ureteral stent with flexible pigtails. These stents are less tightly wound and open at both ends in contrast to Cook's Resonance stent, which is tightly coiled around a stainless steel guidewire and closed at both ends. The technique for placement of the Prosurg Passage and Snake does not differ from traditional stents with insertion over a 0.035" or 0.038" guidewire.

Snake and Passage ureteral stent designs.
Compared with previous testing of Cook Resonance and Applied Medical Silhouette stents using the same methods, all stents evaluated in this study had a much lower tensile strength and higher resistance to radial compression than both the Cook Resonance 6F (936±485 kPa and 63±3 kPa, respectively) and Applied Medical Silhouette 4.6F (770±82 kPa and 106±12 kPa, respectively) stents. 8 A low tensile strength along with the selection of a proper stent length are important factors for patient comfort as well as prevention of stent migration. 10 Moreover, a high resistance to extrinsic radial compression is important for preventing reobstruction from tumor in-growth or stent compression. It is not clear, however, how differences in these physical characteristics would play a role in other failure modes, such as encrustations or urothelium hyperplasia.
The polymer tubing or sheath present over the body of the Snake 7F stent that was absent from the Snake 6F stent comparatively increased the tensile strength. In addition, the increase of 1F in stent diameter weakened the resistance of radial compression despite the presence of the additional sheath. Thus, stent thickness seemed to play a more important role in compressive strength over configuration or design. Therefore, in situations where a metal stent is typically used for alleviation of extrinsic ureteral obstruction, a 6F stent may be more effective in sustaining ureteral patency over a 7F stent. 3,5
Any enhancement of physical characteristics of metal stents that may increase the length of time between stent exchanges can greatly improve patient quality of life. This is primarily achieved by reducing the number of hospitalizations and exposure to anesthesia along with the risk of complications that can occur with a stent exchange. 11 While metallic stents have shown patency rates greater than the 3 to 6 months seen with polymer stents, patients still need to be followed closely for evidence of obstruction, encrustation, infection, or painful stent symptoms because there is no well-established optimal dwelling time for these devices. 11 –13 Cystoscopy can be a tool for monitoring stent encrustation, because the visual appearance of encrustation at the distal end of a stent may correlate with upper stent encrustation. 12 Placement times, however, need to be balanced with the likelihood of safe and efficient removal. Furthermore, increased time between stent exchanges has also been shown to provide a significant cost benefit. 14,15
Conclusion
Both the Passage and Snake stent designs offer a lower tensile strength and high resistance to extrinsic radial compression compared with previously tested Cook Resonance and Applied Medical Silhouette stents and may offer more efficacious management for extrinsic-etiology ureteral obstruction.
Footnotes
Disclosure Statement
No competing financial interests exist.