
Abstract
Purpose:
To evaluate the effect of equivalent doses of local anesthetic administered at different concentrations and volumes on pain scores in patients undergoing prostate biopsy.
Patients and Methods:
This study was a single-center, randomized trial. A total of 120 patients were randomized into two groups with 60 patients in each group. In group 1, 2.5 mL of 2% lidocaine (low volume-high concentration) and in group 2, 5 mL of 1% lidocaine (high volume-low concentration) was injected just lateral to the junction between the prostate base and seminal vesicle on each side under ultrasonographic guidance. Patients were given an 11 point visual analog scale (VAS) to evaluate the level of pain encountered during transrectal ultrasonographic (TRUS) probe insertion, injection of the local anesthetic, and the biopsy procedure.
Results:
In both groups, TRUS probe insertion was the most painful stage of the procedure. With regard to local anesthetic injection, the VAS pain score was significantly lower in group 1 (1.56 vs. 2.41, P=0.001). Concerning sampling of the prostate, group 1 had a significantly lower VAS pain score compared with group 2 (1.71 vs. 2.48, P=0.008). Neither major complications nor side effects related to local anesthetic absorption occurred in both groups.
Conclusion:
Low volume-high concentration lidocaine administration provides superior analgesia compared with high volume-low concentration lidocaine during transrectal biopsy of the prostate.
Introduction
Different local anesthetic techniques for TRUS-guided prostate biopsy have been described. 2 –5 Periprostatic nerve block has been reported as the most effective and commonly used method to diminish pain. 6 The instillation of the local anesthetic, however, may be painful, and discomfort from injection may be comparable to that of obtaining core biopsies. 7 Decreasing local anesthesia-related pain may assist in diminishing pain encountered during the sampling procedure. Administration of equivalent doses of local anesthetic at high concentration and low volume may be beneficial. Attempts to optimize local anesthesia technique have led to changes in the type and volume of anesthetic agents as well as the site of injection. 2,3
We report on the effect of equivalent doses of local anesthetic administered at different concentrations and volumes on pain scores in patients who were undergoing prostate biopsy.
Patients and Methods
This study was a single-center, randomized trial. The pain during probe insertion, local anesthetic injection, and sampling was evaluated by visual analog scale (VAS) pain score (Fig. 1). After institutional research committee approval, a total of 120 patients were recruited for the study between January 2010 and July 2010. Biopsy indications were increased serum prostate-specific antigen (PSA) level and/or an abnormal digital rectal examination. Men with a history of biopsies, chronic prostatitis, chronic pelvic pain, inflammatory bowel disease, anorectal problems, and allergy to lidocaine were excluded from the study. Anticoagulation or antiagregant therapy was discontinued 7 days before the biopsy procedure. A written informed consent was obtained from all patients. Patients were randomly assigned to two groups, each group including 60 patients. Oral levofloxacin, 500 mg daily, was started on the night before the biopsy and continued for 7 days to prevent infection. In addition, patients received 1 g of ceftriaxone intramuscularly 10 minutes before the procedure. Bowel cleansing with a self administered fleet enema was performed in the morning of the biopsy.
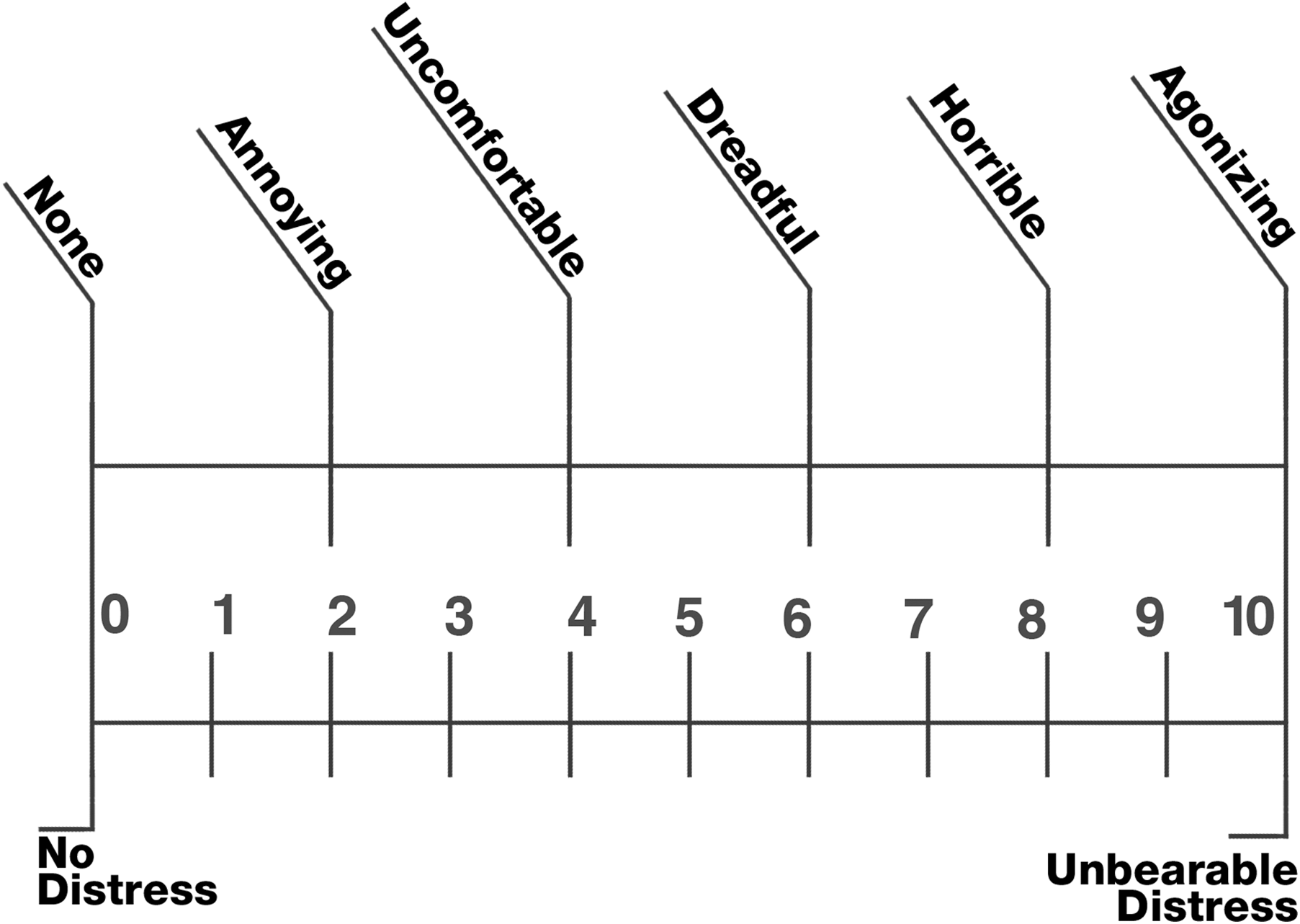
Visual analog scale (VAS) pain score.
All procedures were performed by the same surgical team in an outpatient setting. For local anesthesia, ultrasonographic examination, and biopsy, the patient was in placed in the left lateral decubitus position. Patients were unaware of the local anesthesic volume and concentration administered and were blindly and respectively randomized to group 1 or 2.
A Siemens Acuson Antares Premium Edition color Doppler ultrasonography scanner with 9-4 MHz broad band endocavitary end firing probe with biopsy attachment was used. Parameters such as frequency, dynamic range, depth were automatically set for optimal image quality. The focus level was at midlevel of the prostate gland. A 22-gauge, 20 cm Chiba aspiration biopsy needle was used to inject the local anesthetic. In group 1, 2.5 mL of 2% lidocaine and in group 2, 5 mL of 1% lidocaine was injected just lateral to the junction between the prostate base and seminal vesicle on each side using ultrasonographic guidance (Fig. 2).
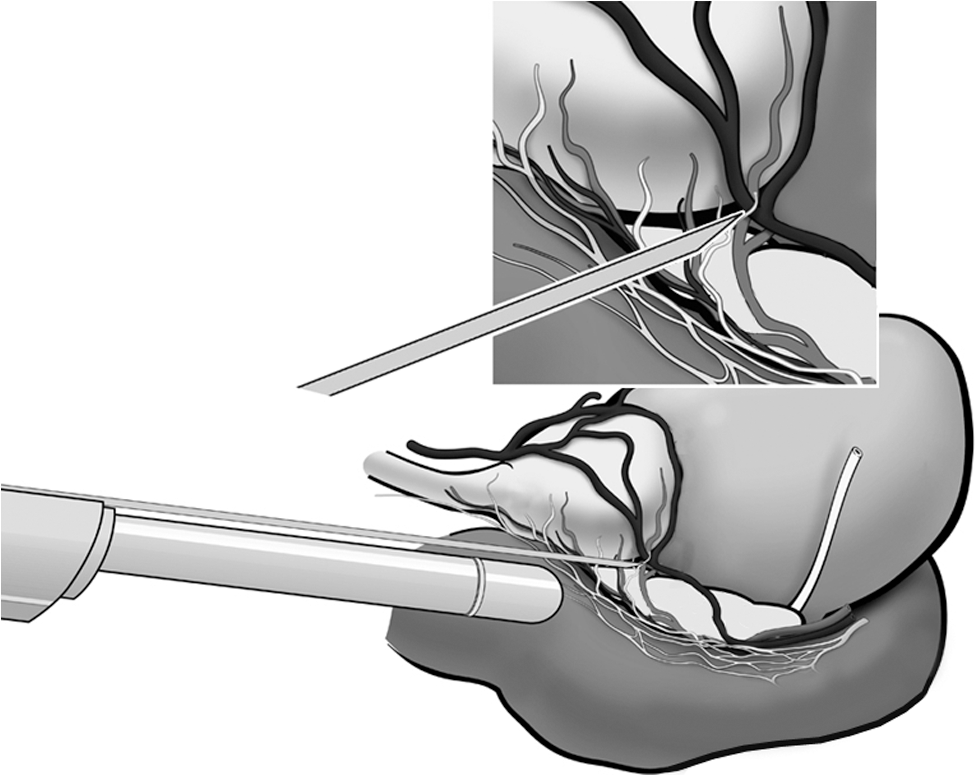
Local anesthetic injection between the prostate base and seminal vesicle.
During infiltration, hitting or traversing the prostate capsule was avoided. In both groups, the syringe was aspirated before local anesthetic injection to avoid intravascular injection. After local anesthetic infiltration, the prostate was examined in sagittal and transverse planes. Prostate volume was calculated with prolate ellipsoid formula (length×width×height×0.52). Five minutes after the local anesthetic injection, prostate biopsy was performed in the transverse plane using a 12-core technique (conventional parasagittal sextant biopsies+6 laterally targeted biopsies covering apex, midzone, and base bilaterally). Biopsy samples were obtained with 18 gauge, 25 cm Angiotech Pro-Mag biopsy needle (FL) using a Pro-Mag Ultra Biopty Gun (Inter V, Wheeling, IL).
Five minutes after the biopsy, all patients were given an 11 point VAS to evaluate the level of pain encountered during TRUS probe insertion, injection of local anesthetic, and biopsy procedure by a blinded staff nurse.
Statistical analyses
The overall patient sample consisted of 120 patients. The sample provided a maximum error estimate of 22.2% in VAS pain score responses with a 99% confidence level. The error estimate was considered to be in acceptable limits when the statistically significant differences were evaluated in percentages.
After conducting a Shapiro-Wilk normality assumption test, nonparametric Kruskal-Wallis and parametric t tests on both group characteristics and VAS pain score responses were performed to examine whether the differences between the two patient groups were statistically significant. Parametric Satterthwaite t test was used for age while comparisons of PSA, prostate volume, and VAS pain score responses were performed using nonparametric Kruskal-Wallis tests.
Results
Patient characteristics including age, PSA level, prostatic volume, and pain score responses for the two groups are summarized in Table 1, along with the statistical tests comparing the two patient groups in terms of both patient characteristics and pain score responses. The difference between the two patient groups in terms of patient characteristics, such as age, PSA level, and prostate volume, was not statistically significant with the resulting P values of 0.4, 0.37, and 0.21, respectively.
Satterthwaite t test.
Kruskal-Wallis chi-square test.
SD=standard deviation; PSA=prostate specific antigen; VAS=visual analog scale.
In both groups, TRUS probe insertion was the most painful part of the procedure. The difference between the patient groups in terms of pain score during probe insertion, however, was not statistically significant (P=0.77).
Regarding local anesthetic injection, mean VAS pain score in group 1 (low volume-high concentration group) was lower than group 2 (high volume-low concentration group). The difference was statistically significant (P=0.001).
Concerning sampling of the prostate, mean VAS pain score in group 1 (low volume-high concentration group) was significantly lower than group 2 (high volume-low concentration group) (P=0.008).
No side effects related to local anesthetic absorption occurred in both groups. Also, there were no major complications such as sepsis or severe rectal or urethral bleeding. One patient from each group was catheterized for urinary retention after the biopsy.
Discussion
There are various explanations for the pain experienced during TRUS-guided prostate biopsy. Stretching of the anus that is below the dentate line occurs during probe insertion. Traversing the prostatic capsule, which occurs during harvesting of biopsy cores, is also thought to elicit pain. The rectal mucosa that is perforated during the biopsy procedure is above the dentate line and has decreased sensorial innervation. Therefore, most of the pain encountered during the biopsy procedure is considered to be associated with the biopsy needle perforating the prostate capsule. 3,6 Strategies to reduce pain have mainly been through attenuating nociceptive stimuli in this latter barrier. There is inferential evidence supporting the latter. 3,6,8
Nash and associates 9 first reported that a periprostatic nerve block decreased pain during TRUS biopsy in 1996. 9 Soloway and Obek 10 popularized this technique in which a local anesthetic was injected laterally into two points on each side of the prostate—at the apex and into the base.
Meta-analytic studies of randomized clinical trials demonstrated that injection of a periprostatic local anesthetic was associated with significantly diminished pain compared with placebo or no injection. 3,6,11,12 Periprostatic nerve block has been reported to be the most effective method in eliminating pain during TRUS-guided prostate biopsy. 6 There are a number of factors that may influence pain control with the administration of local anesthetics for prostate biopsy, including the type of the anesthetic, the amount and concentration of the agent administered, and the site of instillation. Bilateral basal injection is the most common method for periprostatic nerve block. 11 Some studies investigated the efficiency of intraprostatic administration of local anesthesia alone or combined with periprostatic nerve block. Mutaguchi and colleagues 13 reported that intraprostatic administration of local anesthesia significantly decreased the pain associated with prostate biopsy compared with periprostatic nerve block. 13 Lee and coworkers 14 combined intraprostatic anesthesia with periprostatic nerve block and reported better results compared with individual modalities. 14 Akan and associates 5 compared bilateral basal injection with single apical injection for periprostatic nerve block and found no significant difference. In fact, some investigators have reported as many as six injection sites and a total volume of as much as 22 mL. 15 Regarding the variability of the local anesthetic volume and concentration in the literature, 8,11,12,15 we decided to focus on the volume and concentration of the local anesthetic using bilateral basal injections.
This study was designed to compare the effect of equivalent doses but different concentration and volume of lidocaine for periprostatic nerve block before TRUS-guided prostate biopsy. Placebo and no intervention arms were intentionally not used in this study, given the strong evidence that injection of a local anesthetic reduces pain. 3,6,11,12 In this study, pain level was evaluated 5 minutes after the biopsy. Performing the pain assessment after each step of the procedure might have provided more reliable scores. We chose not to do it, because it is somewhat impractical.
Different type, dose, and concentration of local anesthetic material have been reported for periprostatic nerve block. 11,12,15 Some data suggest that infiltrating a larger volume of local anesthetics (10 mL) is associated with lower pain scores compared with lower volume of local anesthetics (2.5–5 mL). 16,17 On the other hand, the use of low volume and high concentration local anesthetic has also been reported to suppress pain and discomfort associated with prostate biopsy. 18,19 In a randomized study, Martella and colleagues 18 compared two different low volume-high concentration local anesthetics and found both to be effective to suppress pain and discomfort associated with prostate biopsy. 18
In a recent publication, discomfort experienced during transrectal biopsy of the prostate was not significantly decreased with periprostatic nerve block and, interestingly, pain from the injection itself was similar to pain from core biopsies. 7 In our study, we found that pain during injection was lower than pain during sampling in both groups. Anxiety was found to be significantly related to pain scores in patients who underwent transrectal prostate needle biopsy. 20 Consequently, one could assume that the pain level at the initiation of the procedure associated with local anesthetic injection may have an impact on patient anxiety, resulting in different pain scores during sampling. In other words, if we can perform a painless local anesthetic infiltration, this may result in a lower state of anxiety, which may lead to a decreased perception of pain throughout the rest of the procedure. To accomplish this, we planned to administer local anesthetic in low volume and high concentration (2.5 mL, 2%) and compare the effect on pain scores with equivalent local anesthetic at high volume and low concentration (5 mL, 1%).
Although the same dose of local anesthetic was injected, we found that high concentration-low volume infiltration significantly reduced pain during lidocaine infiltration compared with low concentration-high volume application. Moreover, patients felt significantly less pain during prostate sampling in the low volume-high concentration group. Bulbul and coworkers 19 also reported their observation that patients were more comfortable with 2 vs. 3 mL of 2% lidocaine infiltration.
Ashley and associates 4 have reported that anesthetic injection was the most painful part of the biopsy procedure. 4 Although their injection site and local anesthetic volume and concentration were similar with our high volume-low concentration local anesthetic group (group 2), in our study, lidocaine administration caused less pain than the biopsy itself in both cohorts.
Diminished pain with lower volume lidocaine may at least be partly explained with less stretching of the nerve endings at the injection site. Better tolerance of pain during the actual prostate sampling in the lower volume and higher concentration group may be explained with a lower level of anxiety after a less painful infiltration and consequently less pain during the biopsy.
Thus, we demonstrated that high concentration-low volume local anesthetic injection with lower pain scores enables a more comfortable prostate sampling.
Footnotes
Disclosure Statement
No competing financial interests exist.