
Abstract
Background and Purpose:
Laparoendoscopic single-site (LESS) surgery has been implemented recently in many laparoscopic (LAP) surgical procedures. We report our initial experience with LESS totally extraperitoneal (LESS-TEP) inguinal hernia repair in relation to conventional LAP-TEP.
Patients and Methods:
Between November 2008 and May 2009, 25 LESS-TEP repairs of inguinal hernia and 29 LAP-TEP repairs of inguinal hernia were performed in 44 patients. Data regarding patient demographics, type of hernia, operative time, complications, postoperative hospital stay, and recurrence were prospectively collected and analyzed.
Results:
All 44 patients were men, aged 17 to 84 years. Of 44 men, 3 had bilateral inguinal hernias in the LESS-TEP group and 7 in the LAP-TEP group. The operative time for bilateral LESS-TEP was 60±15.3 min (range 40–70 min) and 40±21.6 min (range 20–100 min) for unilateral LESS-TEP, while for bilateral hernia LAP-TEP it was 60±24.8 min (range 40–100 min) and for unilateral LAP-TEP it was 50±14.2 min (range 40–80 min). Comparison of operative times in the LESS-TEP and LAP-TEP groups between the first and second half cohort resulted in significant reduction of operative time in the second half of the LESS-TEP group (P<0.001). There were no intraoperative complications. Discharge was within 72 hours for most patients in both groups. There was one early recurrence (mesh displacement) during a median follow-up period of 11.5±2.5 months in the LESS-TEP group and no recurrences during the 11±1.6 months in the LAP-TEP group.
Conclusion:
In our experience, LESS-TEP is a safe and feasible procedure with a short learning curve. In all analyzed parameters, it is comparable to conventional LAP-TEP. Further studies that compare LESS-TEP and conventional multiport LAP-TEP repairs with long-term follow-up evaluation are needed to confirm the initial experience.
Introduction
A further step into less invasive procedures is laparoendoscopic single-site (LESS) surgery, which was introduced in 1998 for LAP appendectomy 2 and cholecystectomy. 3 Lack of technical support kept it hibernating until recently, when it was rediscovered in many urologic, bariatric, and general surgery procedures.
LESS balances between technical challenge, because of minimal triangulation and crossover of instruments, and benefit of single incision, such as minimization of potential bleeding, incisional hernia, organ damage, and visible scars.
LESS can be performed with conventional LAP equipment, although technical upgrades, such as development of several ports for single incision surgery as well as special LAP instruments such as angulated instruments, are being introduced.
In this research, we evaluated LESS-TEP in comparison with LAP-TEP inguinal hernia repair based on technical aspects, operative data, and morbidity on 22 patients in each group and evaluated the learning curve of LESS-TEP.
Patients and Methods
The prospective study included 22 patients in the LESS-TEP hernia repair group and 22 patients in the LAP-TEP hernia repair group operated on between November 2008 and May 2009. In the LESS-TEP group, we have included all successive patients, including the first patient, to evaluate the learning curve measured as a reduction and plateauing of operative time.
Only reducible inguinal hernias were included in the study. Obstructed and strangulated hernias, inguinoscrotal hernias, and patients with associated other hernias, such as ventral hernias, were excluded. Indications for bilateral hernia repair in both groups were a presence of bilateral hernia as well as the presence of bubonocele on cough impulse on the other (asymptomatic) side.
Randomization in groups was generated preoperatively using permuted block randomization in blocks of four. The surgical team was blinded regarding the size of the randomization block. We have collected data regarding patient demographics (age, sex), type of hernia, operative time, complications, postoperative hospital stay, and recurrence (Table 1).
LESS-TEP=laparoendoscopic single-site totally extraperitoneal; LAP-TEP=laparoscopic totally extraperitoneal.
All patients were fully informed about the characteristics of the LESS-TEP procedure and other possible therapeutic options, including open surgery and conventional LAP procedures, as well as the possibility of conversion to the open procedure or LAP-TEP if needed at the time of operation. The study was approved by the hospital ethics committee. All 44 subsequent patients matching inclusion criteria agreed to participate in this study.
We compared operative times for unilateral hernia repairs to display the learning curve for LESS-TEP. For this purpose, patients in the LESS-TEP and in the LAP-TEP groups were divided into cohorts, first half and second half, of patients; the cohorts were compared using the Mann-Whitney U test.
The statistical analysis of continuous variables was performed by Mann-Whitney U test. Two-sided P value < 0.05 was considered significant. Data are presented as median±standard deviation.
Surgical technique
Preoperatively, patients received antibiotic prophylaxis (intravenous cefuroxime 1.5 g). A single surgical team performed all the operations. The team started performing LAP-TEP in 1996 and has performed more than 1000 procedures. The previously described LAP-TEP technique 4 was used for patients in the LAP-TEP group. For patients in the LESS-TEP group, we slightly modified the previously reported technique 5 and its description follows:
A single midline infraumbilical skin incision—in later cases, an intraumbilical horizontal skin incision—on average 2 cm in length was used. Dissection of subcutaneous tissue to the anterior sheet of the rectus abdominis was performed. The anterior sheet was incised 1 cm in length; through this incision, the preperitoneal space was formed with a balloon. A 10-mm port was placed in place of a balloon ditator, and a 30-degree laparoscope (Visera, Olympus, Ishikawa, Tokyo, Japan) was inserted. Two 5-mm ports were inserted through the anterior sheet of the abdominal rectus muscle into the now existing preperitoneal space, each placed 1 cm laterally from the laparoscope.
In six patients, we used a 0-degree angled camera with a working port (Video telescope “OP EndoEYE,” 10 mm, 0' direction of view, WA50120A, Olympus, Ishikawa, Tokyo, Japan) with only one 5-mm port placed 1 cm laterally. In all procedures, standard LAP instruments were used.
Dissection, reposition, and mesh placement were performed in the same way as in LAP-TEP. Because of mesh displacement just a few hours after the operation in the fifth LESS-TEP patient, who was increasingly restless and had a chronic obstructive pulmonary disease (COPD) exacerbation, in the following patients, we routinely used mesh fixation as described previously. 5
The drain was inserted in the first six LESS-TEP patients through the right 5-mm port. Based on the experience from these five cases and previous practice with LAP-TEP, we did not use drainage for subsequent patients.
Results
During the study period, 25 LESS-TEP hernia repairs and 29 LAP-TEP hernia repairs were performed for 44 patients in our hospital (Table 1). All patients were male ranging from 20 to 84 years (58.5±17.2 y) for the LESS-TEP group and 17 to 79 years (55±20.1 y) for the LAP-TEP group.
Of 22 men in the LESS-TEP group, 19 had a unilateral inguinal hernia (10 on the left side); 3 had bilateral hernias. Of 22 men in the LAP-TEP group, 15 had a unilateral inguinal hernia (7 on the left side) and 7 had bilateral hernias. Indirect hernia was found in 22 patients in the LESS-TEP group and 21 patients in the LAP-TEP group, while there were three direct hernias—one in the LESS-TEP group and two in the LAP-TEP group.
The operative time for bilateral LESS-TEP was 60±15.3 min (range 40–70 min) and 40±21.6 min (range 20–100 min) for unilateral LESS-TEP, while for bilateral hernia, LAP-TEP was 60±24.8 min (range 40–100 min) and for unilateral LAP-TEP it was 50±14.2 min (range 40–80 min). The average length of incision was 2 cm (range 1.5–2.5 cm) (Fig. 1).

Intraumbilical transverse incision, 6 months after surgery.
Comparison of operative times in the LESS-TEP and LAP-TEP groups between the first and second half cohorts resulted in a significant reduction of operative time in the second half of the LESS-TEP group (P<0.001) (Fig. 2).
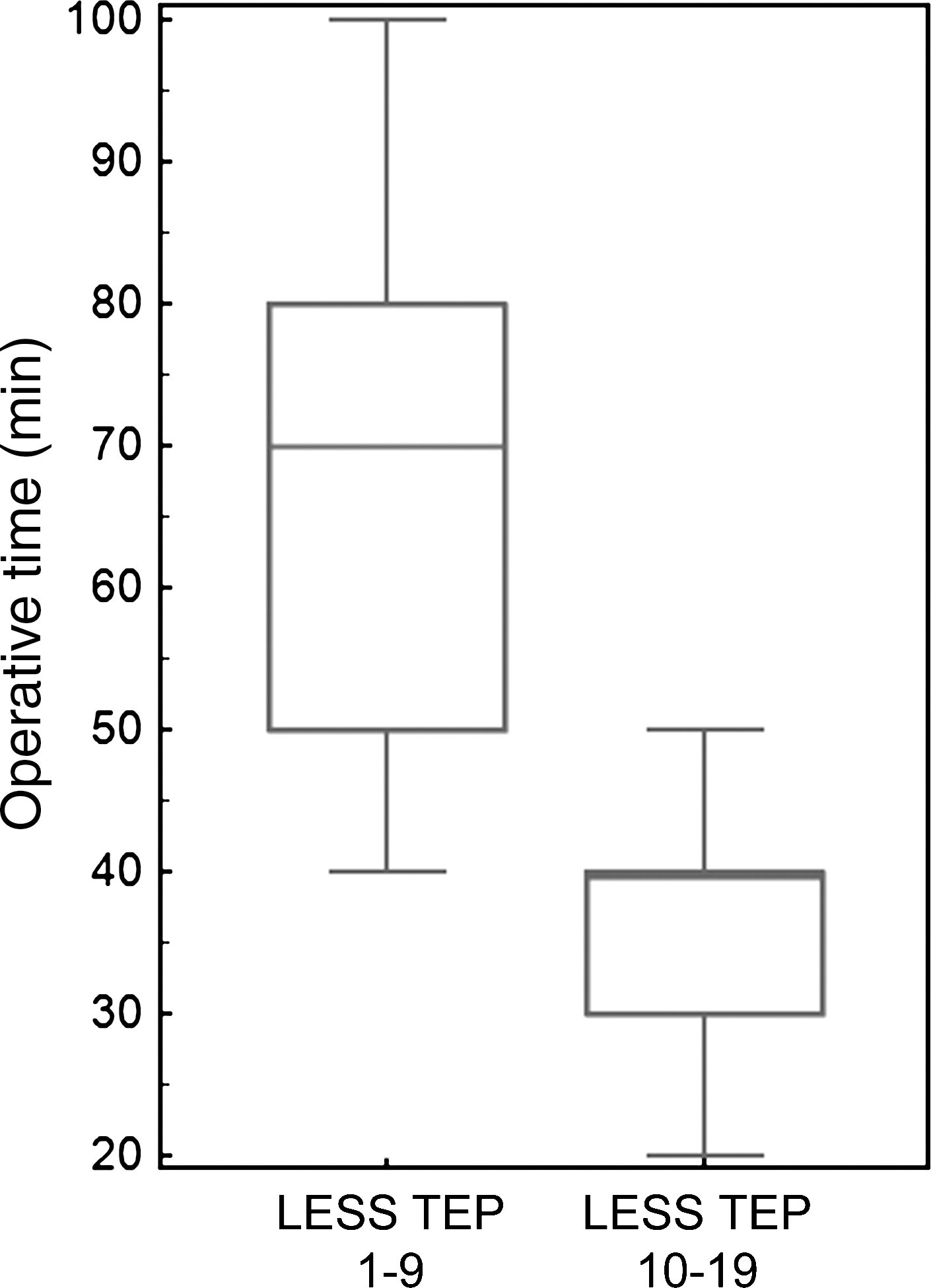
Box plot representing operative times of laparoendoscopic single-site totally extraperitoneal (LESS TEP) surgical procedure performed for unilateral inguinal hernia divided in two cohorts: First nine patients; next 10 patients.
Hospitalization was 2±1.6 days (range 1–9 d) for the LESS-TEP group and 2±1.3 days (range 1–6 days) for the LAP-TEP group, with no significant deference between the two groups. There was one early recurrence, mesh displacement, during a median follow-up period of 11.5±2.5 months in the LESS-TEP group and no recurrences during the 11±1.6 months in the LAP-TEP group (P=0.32) (Table 1). None of the patients was lost from follow-up, and all patients were followed through our standard LAP-TEP scheme. The length of stay of the reoperated LESS-TEP patient was 4 days.
Discussion
The scope of this study was to evaluate the feasibility and technical aspects of LESS-TEP. First, we compared LESS-TEP with LAP-TEP with regard to operative time, duration of hospitalization, and number of complications whereby no statistically significant difference was found. Second, ease of introduction of this technique was evaluated through a learning curve that proved to be acceptable despite the number of technical difficulties that were anticipated.
In our first few cases, incision was placed in the midline a few centimeters below the umbilicus, as described for LAP-TEP. 4 Later, we placed a horizontal incision within the umbilicus. By moving the skin incision closer to the umbilicus, we created a longer channel to the extraperitoneal space, and initial CO2 leakage problems were minimized. LESS-TEP with intraumbilical incision had the most satisfying cosmetic effect, and it did not compromise the surgical approach.
A 30-degree angled camera and a 0-degree angled camera with a working port were both used. 30-degree camera allowed greater comfort to both assistant and the operator with regard to span of hand movement and visual aspects.
Standard LAP instruments were used: Three trocars placed in the same incision. Despite the introduction of specialized instruments, either bent or flexible, which have been developed for single-incision surgery to facilitate viewing, dissection, or both, we still found them insufficient in terms of grasping grip and size of trocars. In our series, LESS-TEP did necessitate adaptation because of clashing and crossing of instruments and reduced triangulation, but there was no need for adjusting to different instruments. In series published to the present date, both approaches have been described. 6
In standard LAP-TEP, there have been several publications in favor of nonfixation of mesh. 7,8 The arguments for this approach were shorter operative time, less postoperative pain, and cost reduction. We did not use mesh fixation in the first few cases of LESS-TEP, but decided to do so after the mesh slippage in a COPD patient (severe cough episode) occurred in the immediate postoperative period. The patient was reoperated on the same day, using the LAP-TEP technique, and mesh was fixed with tucker. Fixation proved to facilitate mesh deployments in subsequent cases.
Operative time was reduced in the LESS-TEP group and stabilized after the first five patients at the median of 40 minutes, which is comparable to the LAP-TEP group. This pointed out how little time was needed for an experienced team to adjust to requirements of LESS-TEP. Similar findings have been observed in LESS cholecystectomy. 9,10 Furthermore, after dividing LESS-TEP and LAP-TEP into two groups, there was statistically significant operative time reduction between the first and second LESS-TEP groups (Fig. 2.). These data describe the learning curve as short and acceptable.
The median hospital stay for both groups was 2 days. This variable, however, cannot be compared directly because of characteristics of healthcare practice in Croatia, which does not provide an incentive for a short hospital stay. Nevertheless, the length of hospital stay is in accordance with data published elsewhere. 6
The average length of the single incision was 2 cm (1.5–2.5 cm) while the sum of three incisions used in LAP-TEP is 3.5 cm (2.5–4.5 cm). Influence of the 1 cm difference on patients' perception of their scar, however, is to say, at least, disputable. Moreover, all patients are male with a substantial amount of hair covering the area. Nevertheless, placing the incision within the umbilicus hides the LESS-TEP scar almost completely and to the observer presents as a cosmetically more acceptable result. In terms of long-term results and larger number of patients, it will be valuable to evaluate patients' scar perception. In this study we did not evaluate patients' scar perception because of variable incision placement in the LESS-TEP group, which was the result of adjustments in operative technique.
There has been an argument saying that this approach was not single-port surgery because of multiple incisions in the anterior rectal fascia 11 ; we argue that there is only one minimal skin incision and that two to three separated fascia (two of which being 5 mm) poses less morbidity than multiport devices designed so far. Furthermore, this approach enables the centers with limited finances to practice LESS, until the costs or/and further development of specialized instruments and ports do not reach an acceptable practical threshold and financial limit range.
The shortcomings of this study and to our knowledge other published studies are small series and short follow-up time; larger series and longer follow-up time are necessary to properly evaluate this approach.
Presently, LAP-TEP is recommended for management of bilateral inguinal hernia, 12 for which LESS-TEP also proved adequate. At this point, we would not recommend LESS-TEP for management of recurrent, incarcerated, or irreducible inguinal hernia until sufficient data are collected to confirm its safety. Nevertheless, patients' choice of procedure in LESS-TEP might present a strong drive in embracing this procedure and extending the indications for it.
Conclusion
Our data show that LESS-TEP has a short learning curve in a team experienced in LAP-TEP. In all analyzed parameters, it is comparable to conventional LAP-TEP. Still, further studies comparing LESS-TEP and LAP-TEP repairs with long-term follow-up evaluation are needed to confirm the initial experience.
Footnotes
Disclosure Statement
No competing financial interests exist.