
Abstract
Background and Purpose:
Becoming proficient in laparoscopic surgery is dependent on the acquisition of specialized skills that can only be obtained from specific training. This training could be achieved in various ways using inanimate models, animal models, or live patient surgery—each with its own pros and cons. Currently, there are substantial data that support the benefits of animal model training in the initial learning of laparoscopy. Nevertheless, whether these benefits extent themselves to moderately experienced surgeons is uncertain. The purpose of this study was to determine if training using a porcine model results in a quantifiable gain in laparoscopic skills for moderately experienced laparoscopic surgeons.
Materials and Methods:
Six urologists with some laparoscopic experience were asked to perform a radical nephrectomy weekly for 10 weeks in a porcine model. The procedures were recorded, and surgical performance was assessed by two experienced laparoscopic surgeons using a previously published surgical performance assessment tool. The obtained data were then submitted to statistical analysis.
Results:
With training, blood loss was reduced approximately 45% when comparing the averages of the first and last surgical procedures (P=0.006). Depth perception showed an improvement close to 35% (P=0.041), and dexterity showed an improvement close to 25% (P=0.011). Total operative time showed trends of improvement, although it was not significant (P=0.158). Autonomy, efficiency, and tissue handling were the only aspects that did not show any noteworthy change (P=0.202, P=0.677, and P=0.456, respectively).
Conclusions:
These findings suggest that there are quantifiable gains in laparoscopic skills obtained from training in an animal model. Our results suggest that these benefits also extend to more advanced stages of the learning curve, but it is unclear how far along the learning curve training with animal models provides a clear benefit for the performance of laparoscopic procedures. Future studies are necessary to confirm these findings and better understand the impact of this learning tool on surgical practice.
Introduction
These models allow for the acquisition of various operative skills, reduce the learning curves for various surgical procedures, and make it easier to reproduce techniques learned and developed in an actual surgical environment. 2 The consequences of using these models are also relevant in other aspects. The process of surgical training is morally and economically costly; therefore, reduced learning curves and optimized resources can reduce the financial and ethical burden involved. 3,4
The use of these resources in a surgical setting deserves special emphasis in urology, especially in the field of laparoscopy. Training centers for laparoscopy are considered to be of great importance, especially because of the high risk of intraoperative complications during surgical procedures early in the learning curve. 5,6 The use of animal models for training and improving the surgical skills of urology residents has been widely advocated, because it elicits improved performance on patients in true surgical environments. 7 –9 The use of animals by these residents has also been of great importance, allowing for the characterization and reduction of learning curves. In addition, the use of animal models allows for training in specific surgical procedures, a resource already adopted in several international centers. 10,11
Given the clear benefits of surgical training using animal models at the beginning of the learning curve, the aim of our study was to assess whether laparoscopy procedures in animal models are also able to promote improvement in the performance of trained urologists with moderate surgical experience.
Materials and Methods
Six urologists with moderate experience in laparoscopy (between 30 and 50 procedures) conducted radical laparoscopic nephrectomies in pigs. Each surgeon performed 10 surgeries, one procedure per week. After approval by the Ethics Committee, each participant signed an informed consent form, without being aware of what would be evaluated (ie, blinded). The surgeries were videotaped and then evaluated by two surgeons experienced in laparoscopy. The evaluators also had no information about the surgeons who performed the procedures (blinded).
The animals were anesthetized with Telazol® (4.4 to 6.6 mg/kg intramuscularly), xylazine (1.1 to 2.2 mg/kg intramuscularly), and atropine (0.04 mg/kg intramuscularly). Anesthesia was maintained with isoflurane (1% to 4%) mixed with 1 to 2 L of oxygen through an endotracheal tube.
The pigs were placed in the flank position with the operative side facing up, and the operating table was partially flexed. The abdomen was insufflated with CO2 via transperitoneal Veress needle access to a maximum pressure of 15 mm Hg. Two 10-mm and two 5-mm trocars were placed. After insufflation was observed, the kidney was exposed from the lower pole to the upper pole. The Gerota fascia was dissected over the kidney. The renal artery, renal vein, and ureter were dissected. The renal artery was clamped with two clips proximally and one distally and then divided. The same was done with the renal vein. The urether was then clamped with one clip proximally and one clip distally and divided. Finally, the kidney was removed, the incisions were closed, and the procedure was considered completed. After the procedures, the pigs were sacrificed.
The criteria for evaluation of the surgical approaches were based on quantitative and qualitative aspects. The quantitative aspects consisted of the total operative time and estimated blood loss. The qualitative aspects were assessed according to the Global Operative Assessment of Laparoscopic Skills published by Vassiliou and associates 12 (Table 1). This method of evaluation involves a rating scale of five aspects of minimally invasive procedures: Depth perception, dexterity, efficiency, tissue handling, and autonomy. For each aspect, the subject receives a score from 1 to 5. Thus, the total score has a minimum of 5 points and a maximum of 25 points.
Adapted from Vassiliou et al. 12
Finally, each parameter was subjected to statistical analysis by the Friedman test for comparison and verification of changes among the 10 analyzed surgical procedures with a level of significance of 5%.
Results
The results can be seen in Figures 1 to 7. Estimated blood loss was statistically significant (P=0.006), with a reduction of approximately 45% when comparing the averages of the first and last surgical procedures. The parameters “depth perception” (P=0.041) and “bimanual dexterity” (P=0.011) also achieved statistical significance, showing increases close to 35% and 25%, respectively, when comparing the averages of the first and last surgical procedures.
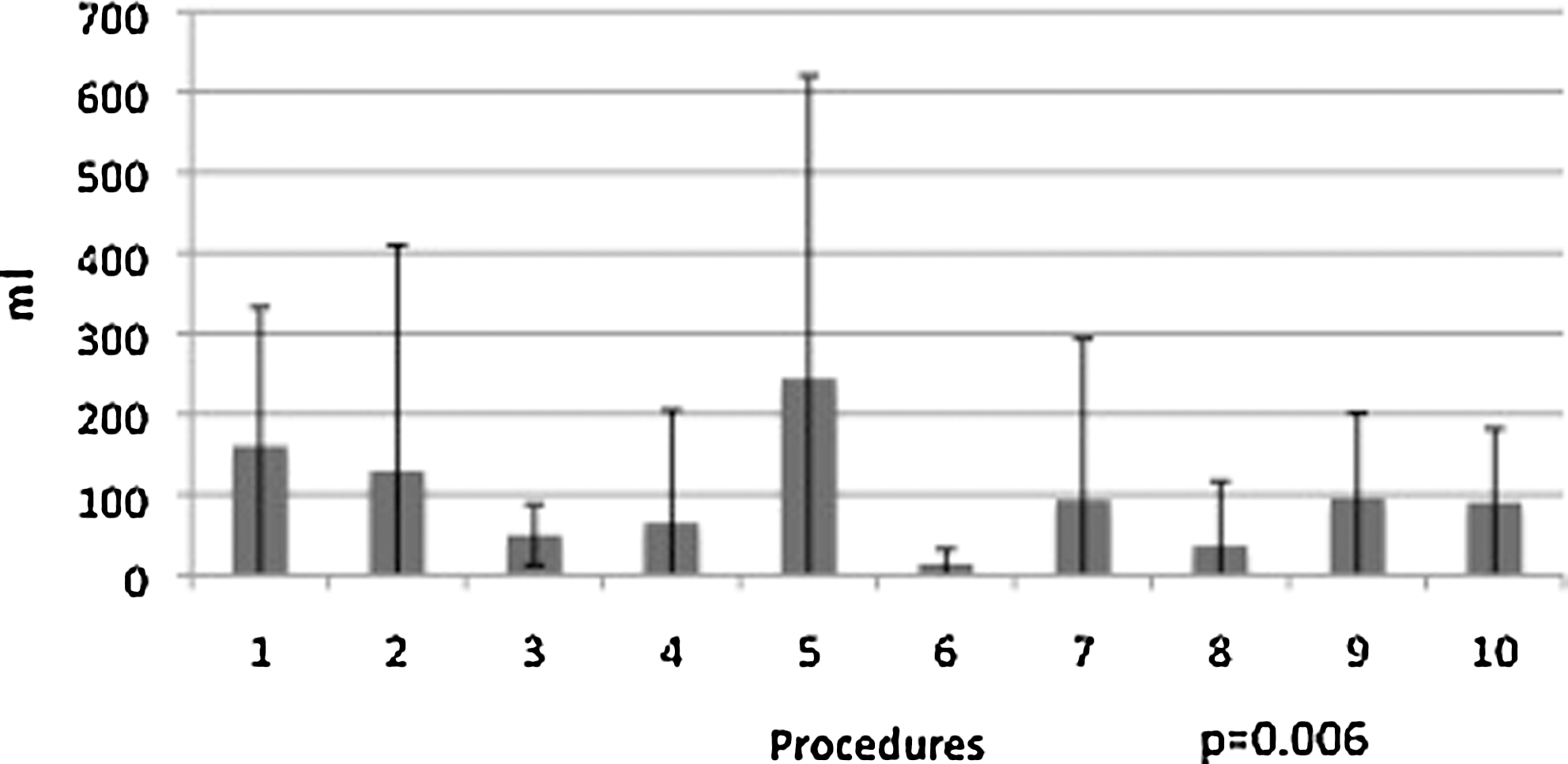
Estimated blood loss.
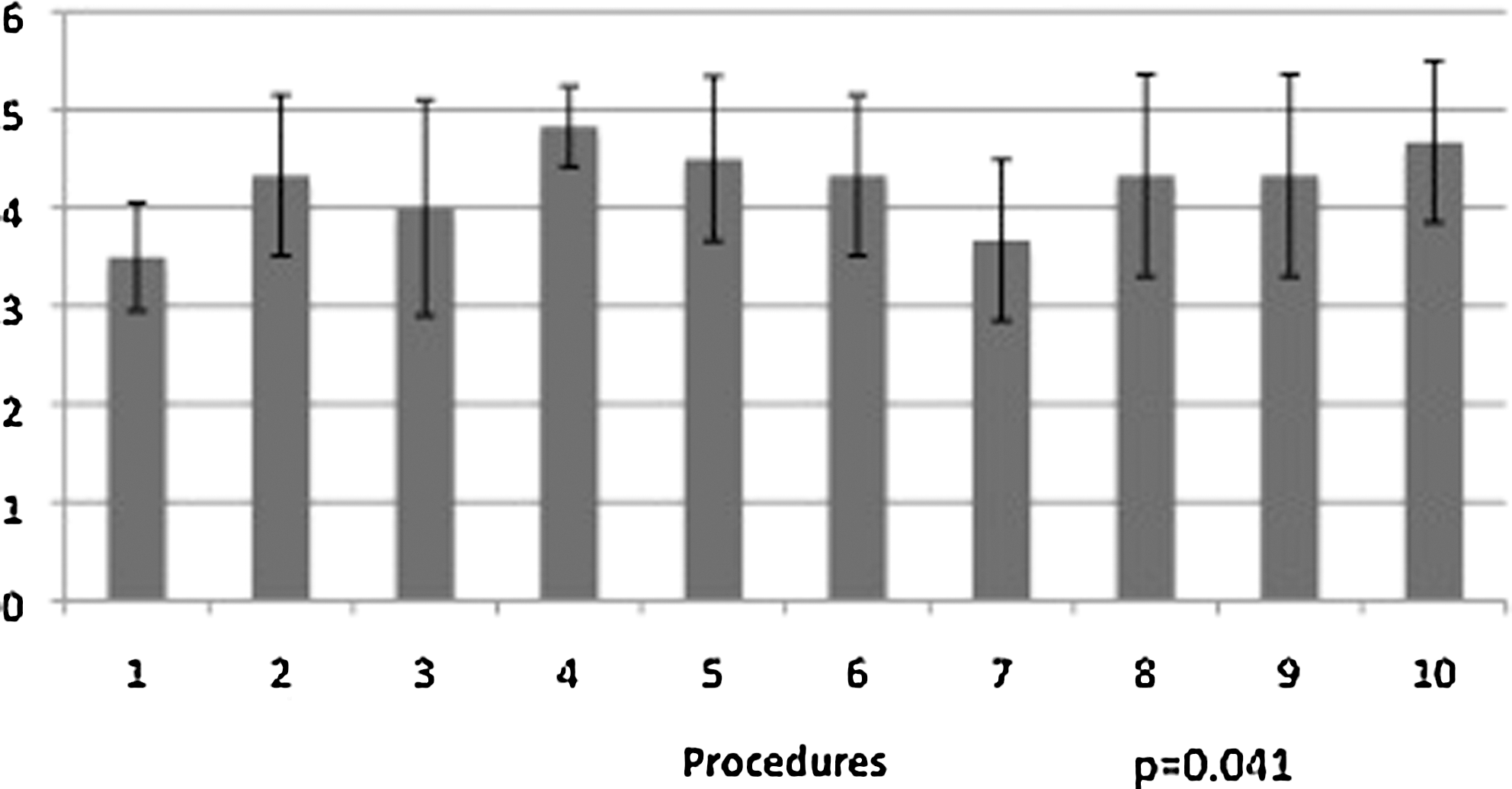
Depth perception.
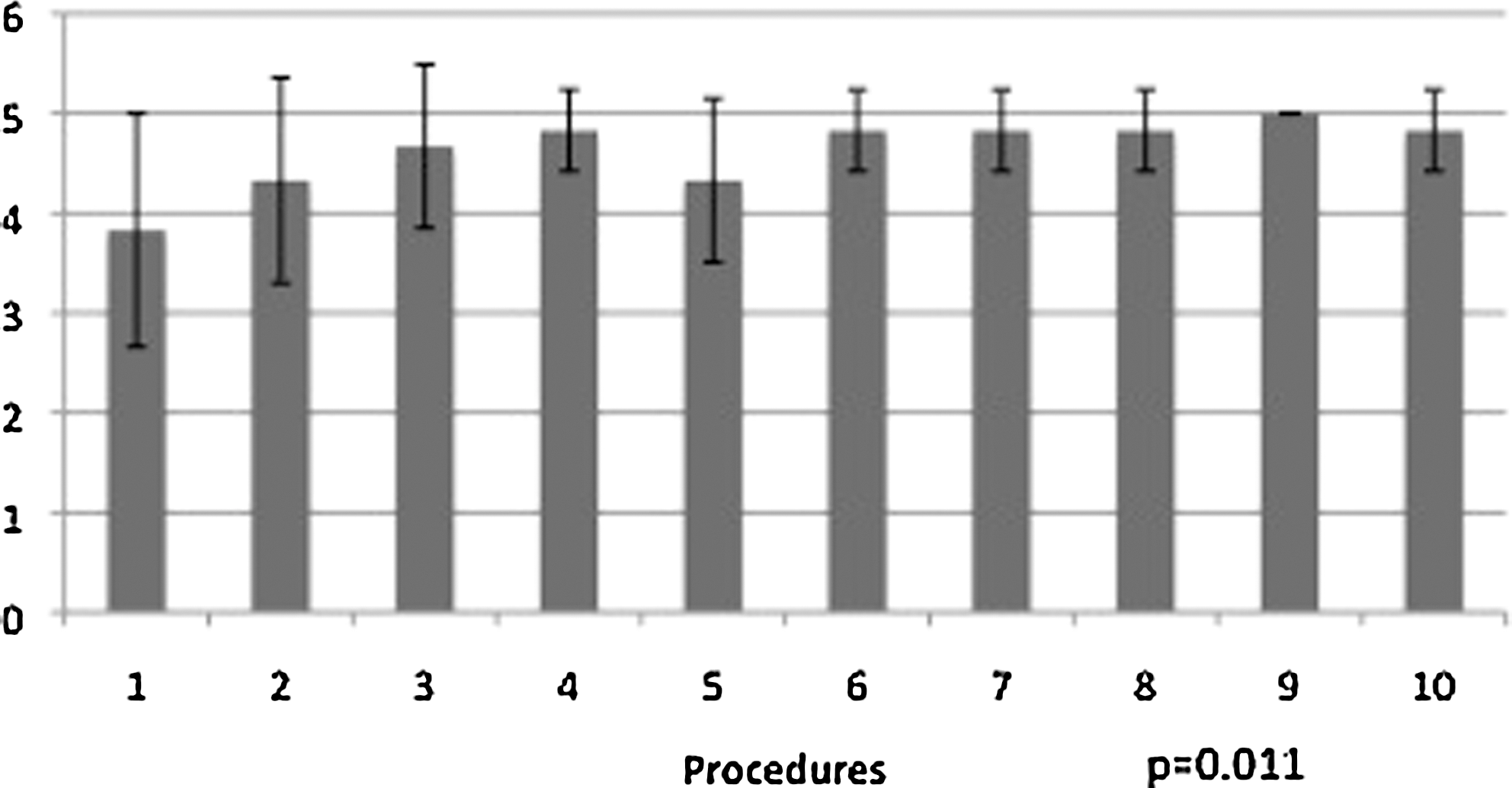
Bimanual dexterity.
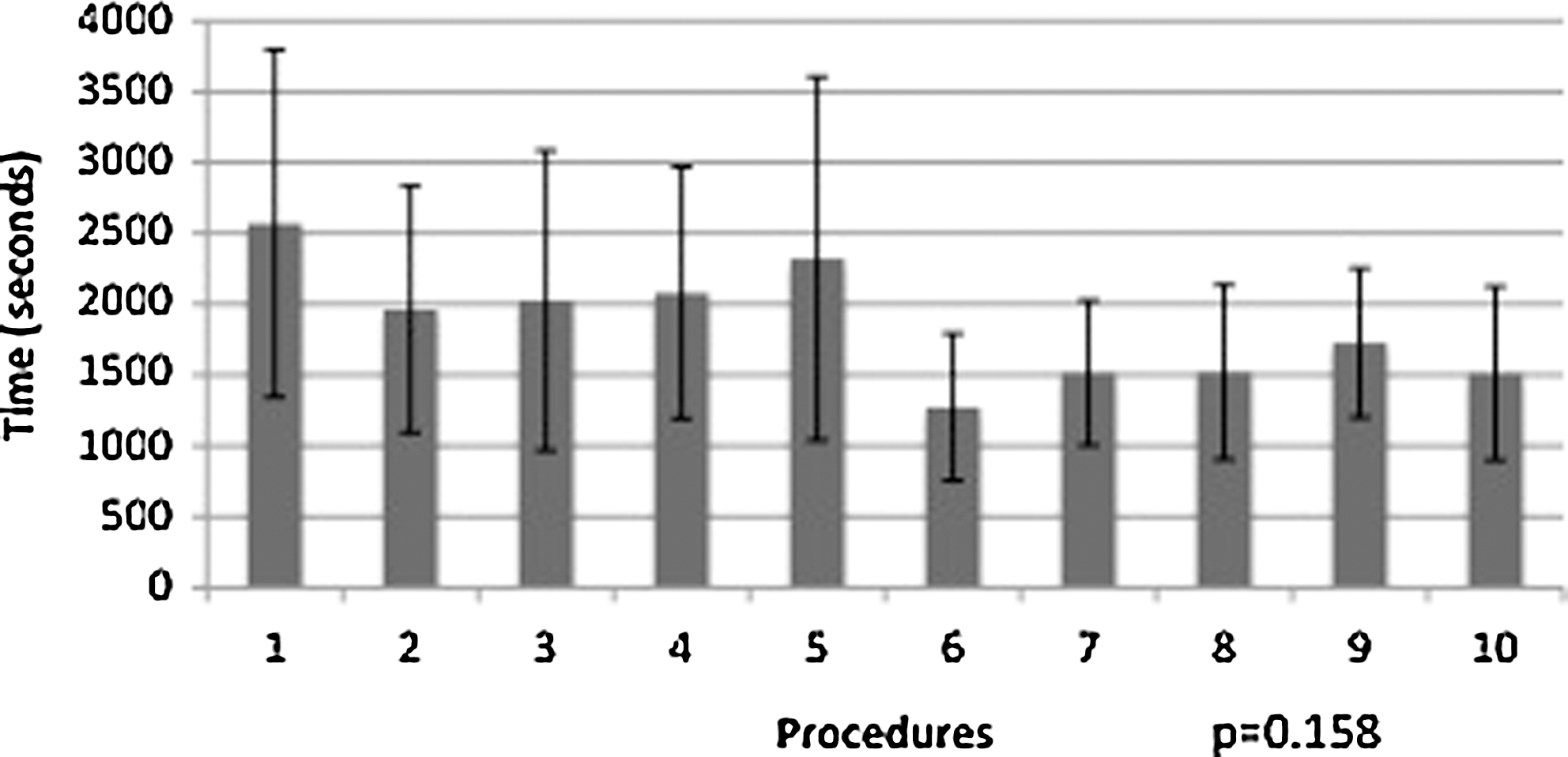
Total operative time.
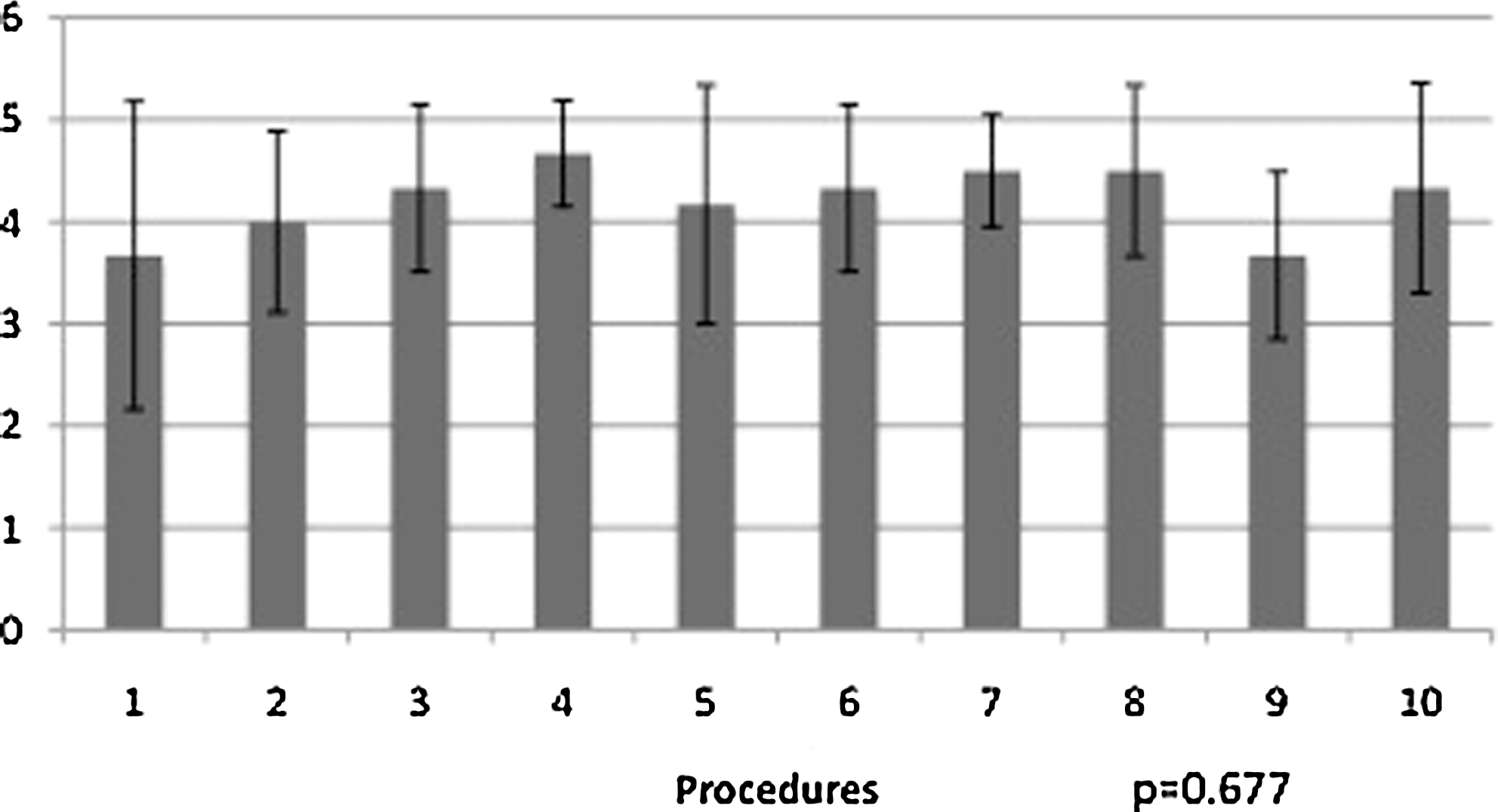
Efficiency.

Tissue handling.

Autonomy.
Although total operative time did not present statistical significance (P=0.158), it showed trends of improvement. Thus, with a larger sample, statistically significant values could be achieved for this parameter. Autonomy, efficiency, and tissue handling were the only aspects that did not show any noteworthy change (P=0.202, P=0.677 and P=0.456, respectively).
Discussion
In recent years, the laparoscopic surgical approach has been of great importance, especially in the field of urology. Currently, laparoscopy is favored over open surgery for several procedures. 13 The initial training for laparoscopic surgery, however, beyond increasing the total financial cost of the surgical procedure, is closely related to the number of intraoperative and postoperative complications. 14,15
For this reason, several studies have been directed at developing methods of surgical training to determine and reduce the learning curve for laparoscopic procedures, especially for residents and surgeons lacking previous experience with laparoscopic operations. Despite the large number of studies focused on learning surgical procedures, there are no published studies that address training for surgeons who have had previous experience with laparoscopy.
In our study, we find that some training benefits obtained for residents and surgeons without previous experience with laparoscopy are also observed for surgeons who have some familiarity with laparoscopy but have not yet reached the plateau of their learning curves. Some studies have evaluated urology residents and trained surgeons learning laparoscopy and have observed better performance after a short series of surgical training sessions (between 10 and 15 procedures). 16 –18 In our study involving the performance of 10 radical laparoscopic nephrectomies in an animal model by surgeons with moderate experience, there was a statistically significant reduction in intraoperative bleeding (P=0.006) as well as improvement in various qualitative measures of surgical performance.
Another parameter to note is the total operative time. Both for urology residents and surgeons learning laparoscopy, there seems to be a significant decrease in total operative time throughout training in surgical procedures. 16,17 In our study, the total operative time showed a declining trend, but it was not statistically significant. This result may be related to the small size of our sample and to the previous experience of the participants.
Regarding autonomy, no trend was found. This result is expected, because our sample consisted of graduated urologists, who already know the steps for performing most laparoscopic procedures in urology.
The present study has several limitations; among them is the small number of participants, which reduces the statistical power of our data. The study also does not correlate training with animal models with any benefit in surgical skill quantifiable in real surgical environments. Moreover, it lacks to determine if a surgeon, even with previous laparoscopic experience, has benefits in his real-life surgical performance by periodically training in animal models.
The use of animal models is a valuable tool for learning surgery, especially laparoscopic surgery. Even surgeons with some experience in laparoscopy seem to present better results in surgical skills with animal models. Whether this gain is reflected in the actual surgical environment in terms of improvement of performance and operative results is still unknown. Further studies are needed to confirm these findings and better define possible new roles for training with animal models in laparoscopy.
Conclusions
The use of animal models for training is already widespread within the surgical community, and there are clear learning benefits for students, residents, and surgeons without previous experience in laparoscopy. Our results suggest that these benefits may also extend to more advanced stages of the learning curve, but it is unclear how far along the learning curve training with animal models provides a clear benefit for the performance of laparoscopic procedures. Future studies are necessary to confirm these findings and better understand the impact of this learning tool on surgical practice.
Footnotes
Acknowledgments
This article was funded by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) and by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Disclosure Statement
No competing financial interests exist.